Hole in the heart
Woman
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrial septal defect" AND women
Reading File
Reading File
Reading File
Reading File
Searching Images
atrial septal defect types diagram heart
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compose a thorough, well-structured answer covering the types, pathophysiology, clinical features (with emphasis on women), diagnosis, management, and pregnancy considerations.
"Hole in the Heart" — Cardiac Septal Defects
"Hole in the heart" refers to an abnormal opening in the walls (septa) separating the heart's chambers. The two main types are Atrial Septal Defect (ASD) and Ventricular Septal Defect (VSD). ASDs are notably more common in women (~2:1 female predominance) and are the most common congenital heart defect diagnosed in adults.
Types and Anatomy
Atrial Septal Defect (ASD)
An opening between the left and right atria. Classified by location:
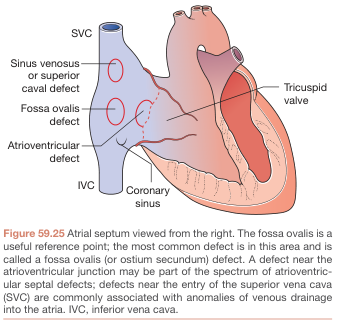
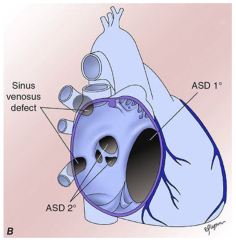
| Type | Frequency | Location | Notes |
|---|---|---|---|
| Secundum ASD | ~90% | Fossa ovalis (center of septum) | Most common adult CHD; incomplete closure of septum primum |
| Primum ASD | ~5% | Adjacent to AV valves | Associated with AV valve defects; ECG shows left axis deviation |
| Sinus venosus | ~5% | Near SVC entry | Associated with anomalous pulmonary venous return |
Ventricular Septal Defect (VSD)
An opening between the left and right ventricles. Classified by location:
| Type | Frequency | Notes |
|---|---|---|
| Perimembranous (infracristal) | ~80% | Below aortic valve; most common VSD type |
| Infundibular/supracristal | ~5–7% | Conal septum; may cause aortic regurgitation |
| Inlet | ~5–8% | At crux of heart; often part of AV canal defects |
| Muscular/trabecular | ~10% | Near apex; can be multiple |
Key distinction: VSDs are more common overall but most close spontaneously in childhood. ASDs rarely close on their own, which is why ASD is the most common congenital heart defect in adults. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathophysiology
Both defects create a left-to-right shunt (oxygenated blood recirculates to the lungs) because left-sided pressures normally exceed right-sided pressures after birth.
ASD → left-to-right shunt at atrial level:
- Right heart volume overload → RV and RA enlargement
- Increased pulmonary blood flow
- Large shunts (Qp/Qs >3:1) → progressive right heart failure
- Risk of paradoxical embolism (thrombus crosses to systemic circulation)
- Long-term: pulmonary hypertension → can reverse to right-to-left shunt (Eisenmenger syndrome)
VSD → left-to-right shunt at ventricular level:
- Small defects: minimal effect, often asymptomatic
- Moderate/large defects: LV and LA dilation, elevated pulmonary artery pressure
- ~10% of large VSDs develop Eisenmenger complex
— Goldman-Cecil Medicine
Clinical Features
ASD in Women — Why It Matters
- ASDs are often silent for decades — many women are diagnosed for the first time during pregnancy or routine workup in their 30s–50s
- >70% become symptomatic by the fifth decade
Symptoms:
- Dyspnea on exertion, fatigue
- Palpitations (atrial fibrillation/flutter — more common in older women)
- Syncope
- Stroke (paradoxical embolism — classically in young women with no obvious cause)
- Signs of right heart failure (leg swelling, elevated JVP) — in advanced disease
Signs on examination:
- Wide, fixed splitting of S2 ← hallmark sign
- Soft pulmonary ejection systolic murmur (2nd left intercostal space)
- Mid-diastolic murmur at lower left sternal border (if large shunt → increased tricuspid flow)
VSD
- Small VSD: Loud pansystolic murmur (Grade 4+), widely radiating, maximal at left sternal border — but paradoxically, louder murmur = smaller defect (restrictive VSD)
- Large VSD: Signs of heart failure, dyspnea, poor feeding (in infants), eventually Eisenmenger syndrome
Investigations
| Test | ASD Findings | VSD Findings |
|---|---|---|
| ECG | Incomplete RBBB; right axis deviation (secundum); left axis deviation (primum) | Normal to LVH/BVH; may have LBBB |
| CXR | Pulmonary plethora, dilated PA, RA/RV enlargement | Cardiomegaly, pulmonary plethora |
| Echo (TTE/TEE) | Diagnostic — shows defect, shunt direction, PA pressure | Confirms location, size, shunt ratio |
| Cardiac catheterization | Quantifies shunt (Qp/Qs), PVR | Same |
Sinus venosus ASDs can be missed on TTE — TEE or cardiac MRI is needed if clinical suspicion remains. — Goldman-Cecil Medicine
Treatment
ASD Closure
Indications: Right heart enlargement, with or without symptoms.
| Approach | Used When |
|---|---|
| Catheter-based device closure (e.g., Amplatzer occluder) | Secundum ASD ≤3.5 cm, adequate septal rim; now >60% of ASD closures |
| Open surgical repair (patch or direct suture) | Primum ASD, sinus venosus ASD, anomalous pulmonary veins, device not feasible |
- In patients >40 years with symptoms + significant shunt: closure improves functional status and survival
- Closure is not indicated when pulmonary vascular resistance is severely elevated (Eisenmenger)
VSD
- Small VSDs: Observation; prophylaxis against infective endocarditis
- Moderate/large VSDs: Surgical patch closure or catheter-based device closure
- Eisenmenger VSD: Medical management (pulmonary vasodilators); transplant consideration
Pregnancy Considerations (Women)
ASD + Pregnancy:
- Uncomplicated ASD without pulmonary hypertension = low risk pregnancy overall
- The physiologic murmur of pregnancy can mask ASD — diagnosis may be missed; clue is fixed S2 splitting
- Small risk of paroxysmal atrial flutter/fibrillation → managed with low-dose β-blockers or calcium channel blockers
- IV line precautions during labor: air bubbles or thrombus can cause paradoxical embolism
- Previously repaired ASD (surgical patch): risk of intraatrial reentrant tachycardia; echocardiographic evaluation recommended before pregnancy
- DOACs contraindicated in pregnancy for anticoagulation if AF develops
If a woman with unrepaired ASD is unwilling to undergo closure pre-pregnancy, she can be reassured that the risk is low provided pulmonary hypertension is absent. — Creasy & Resnik's Maternal-Fetal Medicine
Maternal pre-pregnancy obesity is an independent risk factor for congenital heart defects (including septal defects) in offspring (PMID 38629488, meta-analysis 2024).
Key Clinical Pearls for Women
- Stroke in a young woman with no obvious cause → think PFO/ASD and paradoxical embolism
- New AF in middle-aged woman → screen for undiagnosed ASD
- Fixed splitting of S2 is not a normal finding in pregnancy — investigate
- ASD closure before pregnancy is preferred when feasible — reduces arrhythmia risk
- Non-coding RNA dysregulation (particularly miRNAs) is emerging as a mechanism in ASD pathogenesis (PMID 39172906, systematic review 2024)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Sabiston Textbook of Surgery; Creasy & Resnik's Maternal-Fetal Medicine; Bailey & Love's Short Practice of Surgery; Harrison's Principles of Internal Medicine
The woman has been told to maintain constant weight and will never be able to conceive.
Finding Sources
Finding Sources
Searching PubMed
"Eisenmenger syndrome" AND management
Reading File
Reading File
Reading File
Reading File
Searching Images
Eisenmenger syndrome cyanosis clubbing pulmonary hypertension
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, clinically rich answer. Here it is:
Eisenmenger Syndrome — The Diagnosis This Woman Has
The two clinical clues — maintain constant weight and pregnancy absolutely contraindicated — are the hallmarks of Eisenmenger Syndrome, the end-stage complication of an untreated "hole in the heart."
What Has Happened: The Progression
| Stage | Shunt Direction | Pathology |
|---|---|---|
| Early (unrepaired defect) | Left → Right | Pulmonary overcirculation |
| Progressive | Left → Right (large) | Pulmonary vascular remodeling, rising PVR |
| Eisenmenger Syndrome | Right → Left (reversed) | Irreversible pulmonary arterial hypertension (PAH), PVR ≥ SVR |
When pulmonary vascular resistance (PVR) rises to match or exceed systemic vascular resistance (SVR), the shunt reverses direction — deoxygenated blood now flows into the systemic circulation, causing chronic cyanosis.
"Eisenmenger syndrome occurs when patients with a left-to-right shunt develop irreversible pulmonary vascular injury and severe PAH in response to pulmonary overcirculation. When PVR surpasses SVR, shunt direction reverses, leading to cyanosis." — Braunwald's Heart Disease
Most common causes:
- Large unrepaired VSD, PDA, AVSD → Eisenmenger develops in early childhood
- Unrepaired ASD (<10%) → Eisenmenger develops in adulthood — and is more common in women
Clinical Features

Cyanosis and digital clubbing in a patient with Eisenmenger syndrome (right) compared to a healthy family member (left). — Braunwald's Heart Disease
Signs & Symptoms
| System | Findings |
|---|---|
| Cardiovascular | Central cyanosis, digital clubbing, prominent JVP a-wave, right parasternal heave, loud P2, S3/S4, high-pitched diastolic murmur of pulmonary regurgitation |
| Pulmonary | Dyspnea on exertion, hemoptysis |
| Hematologic | Secondary erythrocytosis (compensatory polycythemia), hyperviscosity, iron deficiency, thrombocytopenia |
| Rheumatologic | Hyperuricemia, gout, arthritis, myalgias |
| Neurological | Risk of paradoxical emboli → stroke, intracranial abscess |
| Infectious | Endocarditis, pneumonia |
Multi-organ Imaging

CXR (cardiomegaly, dilated pulmonary trunks), Echo (dilated RV/RA), CT (pulmonary artery aneurysm + thrombus), V/Q scan (perfusion defects), PET (RV hypertrophy with increased glucose uptake). All features of advanced Eisenmenger syndrome.
Why "Maintain Constant Weight"
Weight management is advised because of hyperviscosity — a dangerous state where the thickened, polycythemic blood becomes prone to:
- Sluggish flow → thrombosis → stroke/paradoxical embolism
- Hemorrhage (paradoxically — platelet dysfunction)
Conditions that worsen hyperviscosity must be avoided:
| ⚠️ Condition to Avoid | Why |
|---|---|
| Volume depletion (dehydration, fasting, vomiting) | Concentrates blood → worsens viscosity |
| Excessive heat (hot baths, saunas) | Vasodilation + fluid loss → hyperviscosity |
| Iron deficiency | Worsens symptoms; iron-deficient red cells are less deformable → worsens viscosity |
| Extreme/strenuous exercise | Drops SVR → worsens R→L shunt |
| Routine phlebotomy | Increases stroke risk; worsens iron deficiency |
| Nonessential surgery | High anesthetic risk |
| Estrogen-containing contraception | Increases thrombotic risk |
Maintaining stable weight keeps fluid balance constant, avoids dehydration, and prevents the hyperviscosity crises that could be life-threatening. — Braunwald's Heart Disease
Why Pregnancy is Absolutely Contraindicated
This is one of the most critical points in all of cardiology:
"Pregnancy is absolutely contraindicated in Eisenmenger syndrome as it is associated with very high levels of maternal mortality (>30%) and fetal loss." — Braunwald's Heart Disease
"Cyanosis associated with Eisenmenger syndrome carries an extremely high maternal mortality rate (at least 50%). Women with Eisenmenger syndrome are advised against pregnancy." — Fuster & Hurst's The Heart
Why pregnancy is so lethal in Eisenmenger:
- Drop in SVR (normal in pregnancy) → worsens right-to-left shunting → worsening cyanosis
- Hypercoagulable state of pregnancy + erythrocytosis → catastrophic thromboembolism risk
- Increased cardiac demand cannot be met by a fixed pulmonary circuit
- Fetal loss rate ~27% even if mother survives
- Valsalva maneuver during labor → acute R→L shunt surge → cardiovascular collapse
Safe Contraception Options for Women with Eisenmenger:
- ✅ Intrauterine device (IUD) — hormonal or copper
- ✅ Depo-Provera (progesterone injection)
- ✅ Nexplanon (progesterone subdermal implant)
- ❌ Estrogen-containing pills/patches — contraindicated (thrombosis risk)
- Surgical sterilization — less commonly recommended now given less invasive options, but remains an option at an experienced ACHD center
If pregnancy does occur, early termination is strongly encouraged, carried out at a center with Adult Congenital Heart Disease (ACHD) expertise due to anesthetic risks. — Creasy & Resnik's Maternal-Fetal Medicine
Management of Eisenmenger Syndrome
Where to Be Managed
Must be followed at a comprehensive Adult Congenital Heart Disease (ACHD) centre — at minimum annually with imaging and labs.
Medical Treatment
| Drug Class | Examples | Evidence |
|---|---|---|
| Endothelin receptor antagonists | Bosentan | BREATH-5 trial: improved exercise capacity and hemodynamics in Eisenmenger (ASD/VSD/PDA) |
| PDE-5 inhibitors | Sildenafil | Epidemiologic data + smaller trials show benefit |
| Macitentan | — | MAESTRO trial: did NOT show benefit in heterogeneous Eisenmenger group |
| Calcium channel blockers | — | Contraindicated — negative inotropy worsens RV function |
Advanced/End-Stage
- Combined heart-lung transplantation or lung transplantation + cardiac repair
- 15-year post-transplant survival: ~41%
- Only for refractory disease with advanced symptoms
NOT Appropriate
- Septal defect closure — contraindicated once Eisenmenger is established; closing the shunt removes the "pressure release valve" for the right heart and can be acutely fatal
Prognosis
Survival depends on the underlying shunt type. Patients with pre-tricuspid shunts (ASD) generally survive longer than those with post-tricuspid shunts (VSD, PDA) because Eisenmenger develops later and more gradually. Many patients live into their 4th–5th decade with appropriate management, but the disease is ultimately progressive and incurable without transplantation.
Sources: Braunwald's Heart Disease; Fuster & Hurst's The Heart 15th Ed.; Creasy & Resnik's Maternal-Fetal Medicine; Harrison's Principles of Internal Medicine 22nd Ed.; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.