History of stapes surgery
Reading File
Searching the Web
history of stapes surgery stapedectomy stapedotomy timeline
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the key content I need. Let me compile a comprehensive, well-structured response.
History of Stapes Surgery
The history of stapes surgery is one of the most dramatic narratives in surgical medicine - a field that was declared dead by the medical establishment, then resurrected and transformed within a single generation.
1. The Pre-History: Valsalva and Early Anatomists
The foundation was laid in 1704 when Antonio Maria Valsalva first identified stapes fixation as a cause of hearing loss. Over a century later, in 1841, Joseph Toynbee dissected 1,659 temporal bones and found 39 cases of stapes fixation linked to deafness. By 1893, Adam Politzer published histological studies identifying otosclerosis as the underlying pathological cause - abnormal bone growth fixing the stapes footplate to the oval window.
- Cummings Otolaryngology, p. 2781; ACTA Ital review 2024
2. First Surgical Attempts and Their Abandonment (1876-1900)
Kessel, in 1876-1879, was among the first to attempt stapes mobilization to relieve conductive hearing loss. Other early surgeons attempted similar operations, some even performing rudimentary stapedectomies.
Then came a catastrophic setback. At the 1900 International Congress of Otology, leaders of the specialty united in condemning surgery for deafness as "not only useless, but dangerous to life." The rejection was total:
- By 1919, Sir Charles Ballance's Surgery of the Temporal Bone made no mention of any operation to improve hearing.
- In 1930, Kerrison's Diseases of the Ear devoted less than a page to the topic, concluding that these operations "mentioned for their place in otologic history are quite obsolete today."
- Shambaugh Surgery of the Ear, p. 796
3. The Fenestration Era (1911-1952)
Despite this hostile climate, a few surgeons persisted:
Bárány (1911), Jenkins (1912), and Holmgren (1914) resumed operations on otosclerosis with "considerable courage in the face of this concerted opposition." Holmgren's key contribution was demonstrating that by careful aseptic technique, a semicircular canal could be opened safely to achieve temporary hearing improvement.
Nylén (1921), a young assistant in Holmgren's clinic, made a pivotal contribution: he was the first to use a monocular operating microscope in ear surgery during a radical mastoidectomy. Holmgren immediately recognized the advantage and adopted a binocular operating microscope for his otosclerosis operations - giving birth to otologic microsurgery.
Sourdille (1924-1937) observed Holmgren's work and returned to France, devising his multi-stage procedure called the tympanolabyrinthopexy - creating a fistula in the horizontal semicircular canal and covering it with a skin flap from the meatus. For the first time, permanent hearing improvements in otosclerosis were documented.
In 1937, Sourdille lectured at the New York Academy of Medicine, which prompted Julius Lempert to apply the technique. Lempert used the endaural approach (rather than postauricular) with a dental drill to create his one-stage fenestration operation - a major simplification. In 1938, G. Shambaugh Jr. became Lempert's first pupil and went on to perform over 5,000 fenestration operations. He further innovated by introducing the operating microscope, continuous irrigation, enchondralization, and a diamond drill for constructing the fenestra - achieving lasting hearing improvements in 80% of fenestrations.
- Shambaugh Surgery of the Ear, pp. 796-797
The key limitation of fenestration surgery was that it bypassed the fixed stapes entirely by creating a new window into the lateral semicircular canal, requiring a permanently open mastoid cavity and maintenance. It also did not fully restore normal hearing thresholds.
4. Stapes Mobilization: A Return to the Oval Window (1953)
In 1953, Samuel Rosen of New York accidentally rediscovered stapes mobilization while testing the stapes for fixation during a fenestration procedure and found that simply freeing the stapes restored hearing immediately. He reintroduced stapes mobilization as a surgical goal in its own right. This fundamentally shifted the operative target from the semicircular canal back to the oval window area.
Results were promising in the short term but recurrence of fixation was common, as otosclerotic bone re-anchored the stapes in most patients over time. The procedure was nonetheless a critical conceptual and anatomical stepping-stone.
5. The Stapedectomy Revolution: John Shea (1956)
On May 1, 1956, John J. Shea Jr. of Memphis performed the first modern stapedectomy - completely removing the stapes and replacing it with a Teflon replica of the stapes connected to a vein graft over the oval window. This was the procedure that changed everything.
Initially considered dangerous by the surgical community, the technique became the new standard by the 1960s. Key subsequent developments in the stapedectomy era:
- Schuknecht (1960) developed a steel-wire loop prosthesis, improving reliability.
- Plester proposed partial footplate removal, further refining technique.
- Zöllner and Wullstein (1955-1960s) contributed concepts of tympanoplasty and ossicular reconstruction, including connecting the incus to the oval window in stapedectomy cases.
- The vein graft was soon supplemented and sometimes replaced with perichondrium or fat tissue seals.
- Cummings Otolaryngology, p. 2781; Shambaugh Surgery of the Ear, p. 797
During the 1960s and 1970s, stapes surgery reached its peak volume. Surgeons like Harold Schuknecht at Massachusetts Eye and Ear Infirmary (Harvard) reportedly performed over 20,000 stapedectomies as the backlog of unoperated cases was worked through.
6. Stapedotomy: The Small-Fenestra Technique (1970s-1980s)
A refinement of stapedectomy came with the concept of stapedotomy - rather than removing the entire footplate, a small fenestra (0.6-0.8 mm) is drilled or perforated into the footplate, and a piston-type prosthesis is inserted through it. Key advantages:
- Preserves the footplate as a protective barrier to the inner ear
- Reduces risk of perilymphatic fistula
- Lowers the rate of sensorineural hearing loss (SNHL) and post-operative vertigo
- More stable long-term hearing outcomes
Guilford and others popularized the small-fenestra technique in the USA. The shift from stapedectomy to stapedotomy became the dominant trend from the 1980s onward, and most otologists today prefer stapedotomy whenever feasible.
7. The Laser Era (1980s-Present)
The introduction of laser technology into stapes surgery was another landmark. The CO₂ laser, KTP (potassium titanyl phosphate) laser, and argon laser have all been applied to:
- Precisely create the small fenestra in the footplate
- Divide the stapedial tendon and crura without mechanical trauma
- Reduce bleeding and the vibration transmitted to the inner ear during footplate penetration
Laser stapedotomy has been associated with reduced inner ear trauma in selected hands.
8. Endoscopic Stapes Surgery (2000s-Present)
The most recent phase of evolution is the adoption of endoscopic ear surgery (EES) for stapes procedures. The endoscope provides a wide-angle, high-magnification view of the oval window niche with a single-handed technique, often through a purely transcanal approach without any incision. While depth perception is reduced compared to the binocular microscope, endoscopic stapedotomy is now practiced in specialized centers and offers improved visualization of the oval window anatomy.
- ACTA Ital 2024 review
Summary Timeline
| Year | Surgeon | Development |
|---|---|---|
| 1704 | Valsalva | Identified stapes fixation causing deafness |
| 1841 | Toynbee | Linked stapes fixation to deafness in 1,659 temporal bone dissections |
| 1893 | Politzer | Histological identification of otosclerosis |
| 1876-1879 | Kessel | First stapes mobilization attempts |
| 1900 | International Congress of Otology | Surgery for deafness condemned |
| 1914 | Holmgren | Semicircular canal fenestration (temporary results) |
| 1921 | Nylén/Holmgren | First use of operating microscope in ear surgery |
| 1924 | Sourdille | Tympanolabyrinthopexy - first permanent improvements |
| 1938 | Lempert | One-stage endaural fenestration operation |
| 1940 | Shambaugh Jr. | Microscope + diamond drill for fenestration; 80% success |
| 1953 | Rosen | Reintroduction of stapes mobilization |
| 1956 | John Shea | First stapedectomy with Teflon prosthesis |
| 1960 | Schuknecht | Steel-wire prosthesis |
| 1970s-1980s | Guilford et al. | Small-fenestra stapedotomy |
| 1980s | Various | Laser-assisted stapedotomy |
| 2000s+ | Various | Endoscopic stapes surgery |
The arc of stapes surgery reflects a broader truth in medicine: transformative advances often require surgeons willing to persevere against institutional consensus. From Holmgren's defiance of the 1900 condemnation to Shea's "dangerous" Teflon prosthesis, each breakthrough came from those willing to challenge received wisdom.
- Shambaugh Surgery of the Ear, pp. 795-797
- Cummings Otolaryngology Head and Neck Surgery, p. 2781
Intractable epistaxis
Reading File
Finding Sources
Finding Sources
Searching the Web
intractable epistaxis management arterial ligation embolization guidelines
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the content and images needed. Here is the comprehensive response:
Intractable Epistaxis
Intractable (refractory) epistaxis is nosebleed that fails to respond to standard conservative and first-line measures - namely pressure, topical vasoconstrictors, anterior packing, and direct cautery. It requires escalating surgical intervention and demands a systematic approach to blood supply anatomy.
Vascular Anatomy - The Foundation
Understanding which vessels supply the nasal cavity determines which intervention to choose:
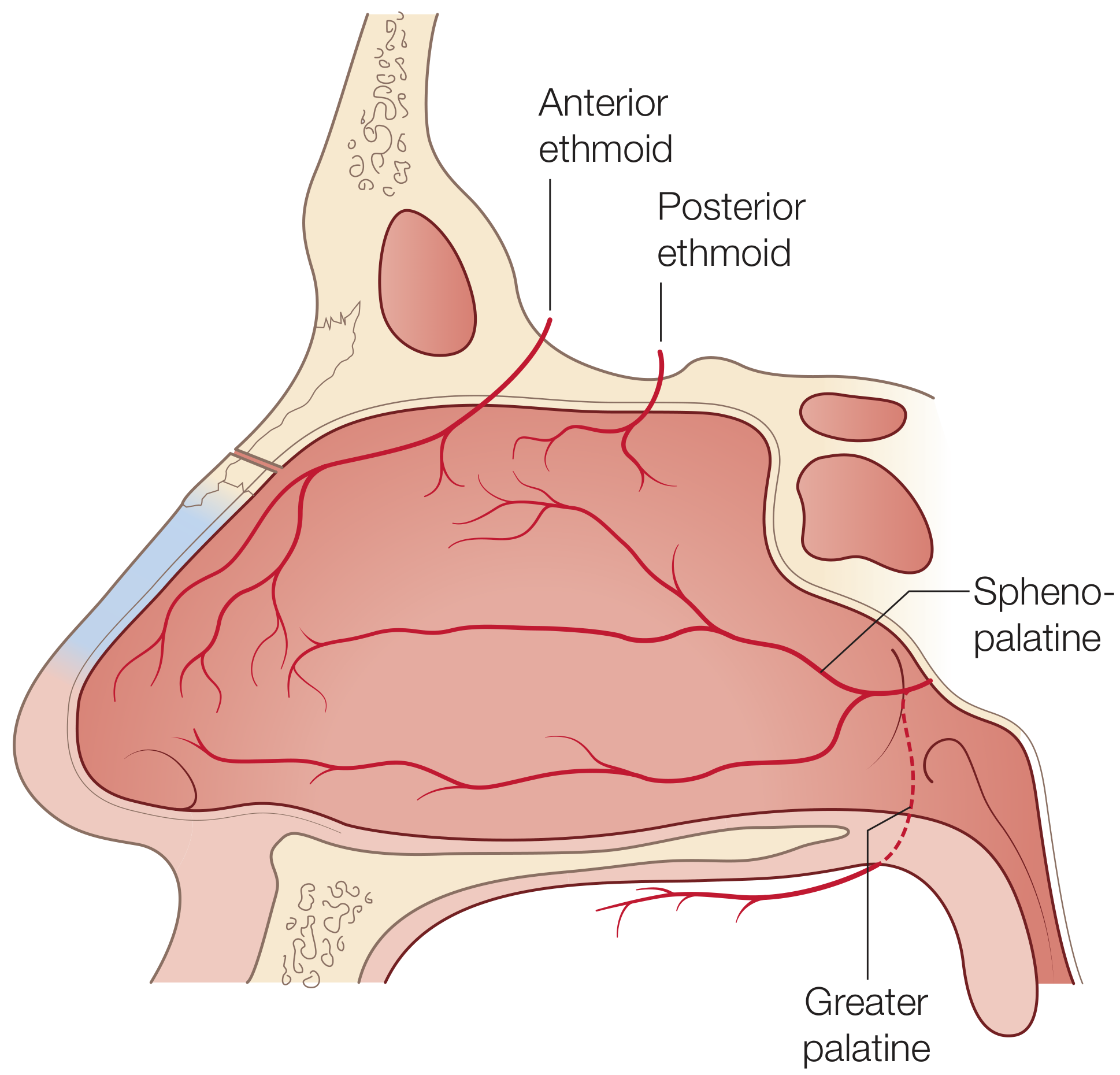
- Sphenopalatine artery (SPA) - the dominant supply, a terminal branch of the internal maxillary artery entering through the sphenopalatine foramen. Responsible for the vast majority of posterior epistaxis.
- Internal maxillary artery - the parent of the SPA, accessible in the pterygopalatine fossa.
- Anterior and posterior ethmoidal arteries - branches of the ophthalmic artery (internal carotid system), supplying the superior nasal cavity and septum. Important in trauma and skull base surgery.
- Kiesselbach's (Little's) plexus - anastomotic network on the anteroinferior septum where multiple vessels converge; the source of most anterior epistaxis.
- External carotid artery - ligation proximal to lingual artery is a last resort.
What Defines "Intractable"
Epistaxis becomes intractable when:
- Anterior nasal packing fails to control bleeding
- Posterior bleeding cannot be directly visualized or cauterized
- Bleeding recurs after packing removal
- Hemorrhage is life-threatening (requires blood transfusion)
Step-by-Step Escalating Management
Step 1 - Initial First-Line Measures (Not Intractable Yet)
- Firm compression of the lower third of the nose for at least 5 minutes
- Topical vasoconstrictors: 0.05% oxymetazoline spray or epinephrine 1:1,000 soaked cotton
- Anterior rhinoscopy to identify the bleeding point
- Silver nitrate cautery (chemical) at Kiesselbach's plexus - cauterize circumferentially first, then the active site
- Electrocautery for more severe active bleeding at 15W under endoscopic guidance
Topical hemostatic agents applied at the bleeding site have become increasingly used:
- Oxidized regenerated cellulose (Surgicel)
- Gelatin sponge (Gelfoam)
- Thrombin with gelatin matrix (Floseal) - particularly effective for both anterior and posterior bleeding
Step 2 - Anterior Nasal Packing
Indicated when direct cautery fails or no bleeding point can be identified.
- Absorbable packing (Nasopore, MeroGel, hyaluronic acid): better tolerated, dissolve within ~1 week, but may not provide sufficient pressure for arterial bleeding
- Non-absorbable packing (Vaseline-impregnated ribbon gauze, Merocel sponge): more pressure, but removed at 48-72 hours - carries risk of rebleeding on removal
- Pack must be directed along the nasal floor, not superiorly toward the skull base
- Cummings Otolaryngology, p. 940
Step 3 - Posterior Packing
Required when anterior packing fails to control posterior bleeding, particularly in elderly patients with hypertension. Scott-Brown's notes this should be viewed as largely obsolete but remains relevant where specialist rhinology expertise is unavailable.
Options:
- Belloc's (traditional) posterior pack: gauze pack positioned transorally via tapes passed from posterior choana to anterior nares. Secured anteriorly over padding to protect the columella from pressure necrosis. Requires opiate analgesia and antibiotics. Left in place minimum 48 hours.
- Foley catheter technique: size 12-14 Foley passed along the nasal floor, balloon inflated with 15 ml of water in the nasopharynx, pulled forward to occlude the posterior choana, then anterior packing added. Easier to insert but equally uncomfortable.
- Epistaxis balloon catheters (e.g., Rapid Rhino dual balloon): distal balloon inflated in nasopharynx, proximal sausage-shaped balloon inflated within the nasal fossa.
Complications of posterior packing: pain, hypoxia (soft palate edema), sinusitis, middle ear effusion, septal/columella necrosis. All patients with posterior packs require hospital admission and monitoring.
- Scott-Brown's Vol 1, p. 1224-1225
Surgical Management - When Packing Fails
Once packing fails or is insufficient, direct surgical or interventional radiology is required. The principle is to ligate as close to the bleeding point as possible.
Hierarchy of Ligation
| Priority | Vessel | Route |
|---|---|---|
| 1st | Sphenopalatine artery | Endoscopic (ESPAL) |
| 2nd | Internal maxillary artery | Transantral or endoscopic |
| 3rd | External carotid artery | Transcervical (last resort) |
| Adjuvant | Anterior/posterior ethmoidal artery | Open (Lynch/transcaruncular) or endoscopic |
1. Endoscopic Sphenopalatine Artery Ligation (ESPAL) - Procedure of Choice
ESPAL has now largely replaced all other ligation techniques as the procedure of choice, with success rates approaching 100% in some series.
Technique:
- Performed under general or local anaesthetic
- An incision is made approximately 8 mm anterior to and under cover of the posterior end of the middle turbinate
- Incision carried down to bone; mucosal flap elevated posteriorly
- The fibro-neurovascular sleeve emerging from the sphenopalatine foramen is identified - the crista ethmoidalis (a bony projection of the palatine bone) is the key landmark signalling the foramen's location
- The main vessel is ligated with haemostatic clips and divided, or coagulated with bipolar diathermy
- The ipsilateral facial artery branches may also be addressed
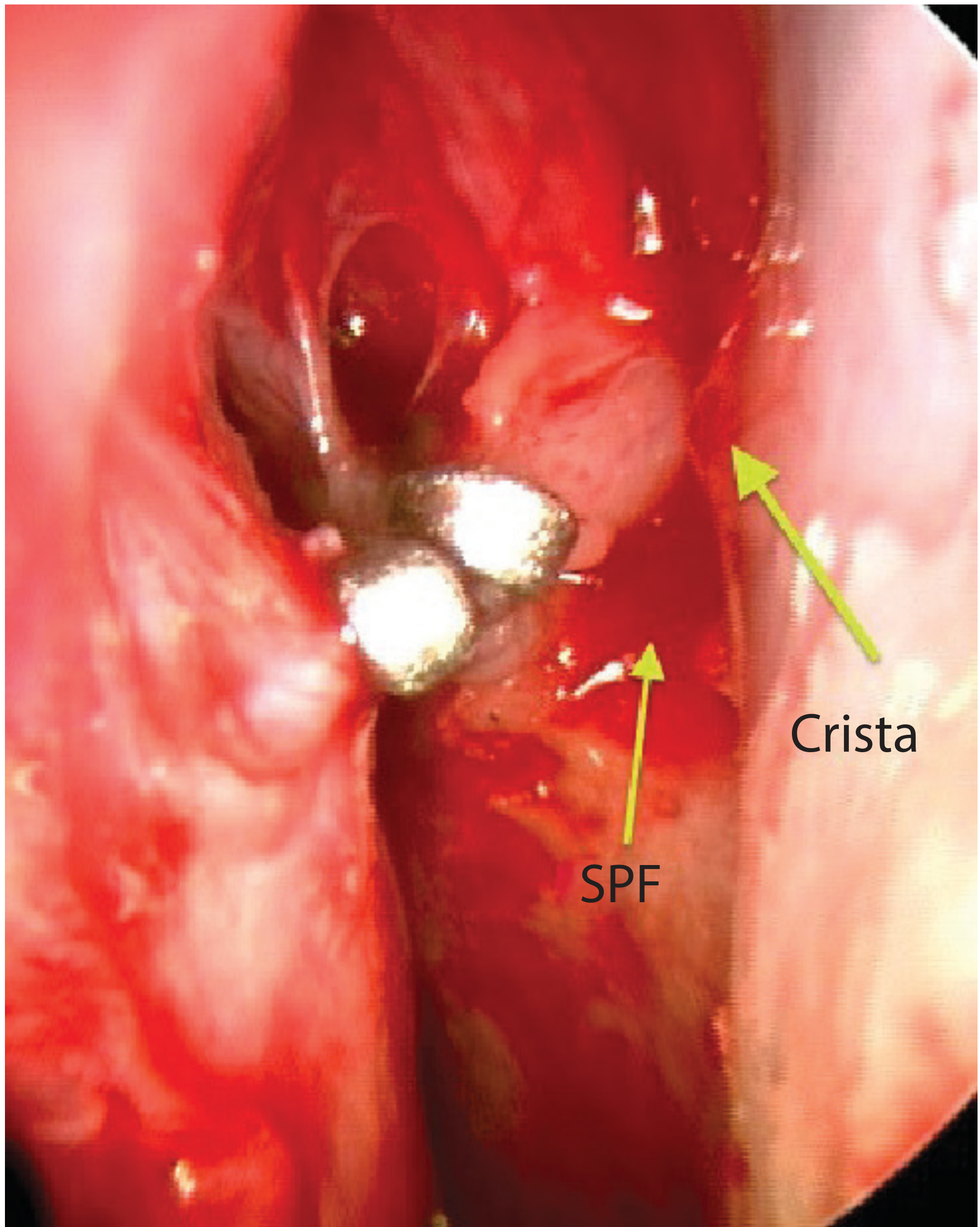
ESPAL: haemostatic clips on the sphenopalatine artery trunk. Crista ethmoidalis (Crista) marks the foramen (SPF). - Scott-Brown's Otorhinolaryngology, p. 1226
Complications: re-bleeding from anastomoses, nasal adhesions, infection - generally less common than other procedures.
- Scott-Brown's Otorhinolaryngology Vol 1, p. 1226
2. Internal Maxillary Artery Ligation (IMAL)
Used before ESPAL became widespread; now primarily performed during skull base procedures (transpterygoid approaches, juvenile angiofibroma resection).
- Traditional approach: transantral via sublabial Caldwell-Luc antrostomy - posterior maxillary sinus wall elevated, pterygopalatine fossa entered, branches of the internal maxillary artery (proximal, descending palatine, sphenopalatine) identified and clipped
- Endoscopic approach: middle meatal antrostomy with posterior antrostomy to access the ptergyopalatine fossa
Risks: vidian nerve injury (dry eyes), greater palatine nerve injury (palatal paresthesia), infraorbital nerve injury (cheek paresthesia).
- Cummings Otolaryngology, p. 941
3. Anterior Ethmoidal Artery Ligation
Indicated specifically for:
- Skull base trauma (naso-orbito-ethmoidal fractures)
- Iatrogenic injury during endoscopic sinus or skull base surgery
- Confirmed ethmoidal origin of bleeding
- Upper/superior nasal cavity bleeding not controlled by SPA ligation
Critical anatomy: The anterior ethmoidal artery is found between the 2nd and 3rd lamella. The traditional mnemonic for distances from the anterior lacrimal crest is 24-12-6 mm (anterior lacrimal crest → anterior ethmoidal foramen → posterior ethmoidal foramen → optic canal). However, the number of foramina is variable and multiple branches may be present.
Endoscopic approach: complete ethmoidectomy, define skull base, drill/curette bony canal to expose vessel, bipolar cautery or clips.
Open approaches:
- Lynch incision: straight medial canthal incision - excellent access but leaves a visible scar
- Transcaruncular/precaruncular approach: scarless, incision at or anterior to lacrimal caruncle, dissect to lamina papyracea, elevate periorbita posteriorly to reveal ethmoidal foramina
Warning: If the artery is transected laterally, the proximal stump retracts into the orbit, causing retrobulbar hematoma - a surgical emergency requiring immediate orbital decompression.
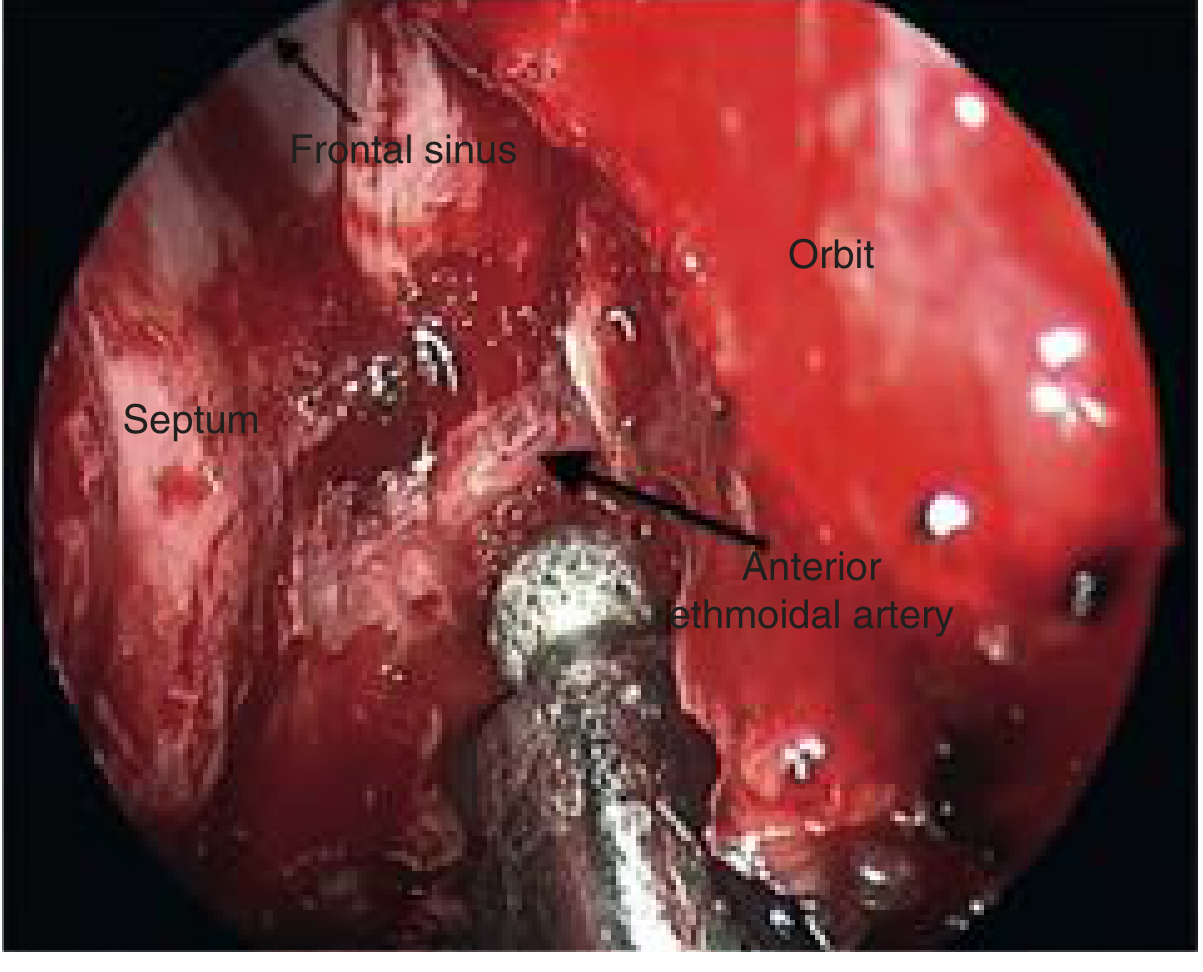
Endoscopic view of the anterior ethmoidal artery being drilled in preparation for bipolar cautery. - Cummings Otolaryngology, p. 941
- Cummings Otolaryngology, pp. 941-942
4. External Carotid Artery Ligation
A last resort only, via a transcervical approach. Due to the efficacy of ESPAL and embolization, this is rarely used and offers no proven additional benefit over less invasive options.
- Cummings Otolaryngology, p. 941
5. Septal Surgery
When epistaxis originates behind a septal deviation or vomerine spur, septoplasty or submucous resection (SMR) may be needed to gain access to the bleeding point. The rationale is that elevating the mucoperichondrial flap disrupts the septal blood supply and secures hemostasis. Historically used when packing failed, but largely superseded by ESPAL.
- Scott-Brown's Otorhinolaryngology Vol 1, p. 1227
Embolization (Interventional Radiology)
Efficacy: 75-97% success in controlling severe epistaxis.
Technique: Transfemoral Seldinger angiography under local anaesthetic. The nasal circulation is mapped to:
- Exclude AVMs, aneurysms, and fistulae before embolization
- Identify the bleeding vessel
- Pass a fine catheter into the internal maxillary artery (most common target) and embolize with polyvinyl alcohol particles, tungsten, or steel microcoils
- The ipsilateral facial artery is also embolized to prevent re-circulation via anastomoses
Advantages:
- Avoids general anaesthesia
- Suitable for poor surgical candidates
- Effective for tumour-related bleeding (nasopharyngeal carcinoma, sinonasal tumours)
- Useful for vascular tumours (juvenile angiofibroma) - preoperative embolization reduces intraoperative blood loss
- Preferred for craniofacial trauma with distorted anatomy
- Essential for carotid blowout (iatrogenic or traumatic) after local endoscopic control
Complications:
- Blindness (inadvertent ophthalmic artery embolization)
- Cerebrovascular accident / stroke (1.1-1.5%)
- Skin necrosis, facial paresthesia
- Groin haematoma at puncture site
- Acute kidney injury from iodinated contrast
Important: Embolization should not be used for the internal carotid system due to stroke and blindness risk. It is more costly than surgical management. Scott-Brown's recommends reserving it for failed ligations or where rhinological surgical expertise is unavailable.
- Cummings Otolaryngology, p. 942; Scott-Brown's Vol 1, p. 1227
Special Considerations
Hereditary Haemorrhagic Telangiectasia (HHT / Osler's Disease)
Patients with HHT have multiple mucosal telangiectasias and present with recurrent, bilateral, severe epistaxis. Standard packing and ligation give only temporary relief as telangiectasias reform. Management includes:
- Topical oestrogen, bevacizumab (anti-VEGF) nasal spray
- Laser photocoagulation of telangiectasias
- Septal dermoplasty (Young's procedure - surgical closure of the nasal cavity)
- Systemic anti-angiogenic therapy (bevacizumab IV)
Anticoagulated Patients
Reversal of anticoagulation (warfarin reversal with vitamin K/FFP, direct oral anticoagulant reversal agents) is a critical adjunct. Epistaxis in this setting will not resolve while coagulopathy persists. Resorbable packing is preferred to avoid rebleeding on removal.
Tumour-Related Epistaxis
Preoperative embolization is the preferred intervention for vascular tumours. For nasopharyngeal carcinoma, embolization avoids violating external surfaces while devascularizing tumour-feeding vessels.
Summary Algorithm
Epistaxis
↓
Compression + topical vasoconstrictor (≥5 min)
↓ fails
Endoscopy + direct cautery / topical haemostatic agent
↓ fails
Anterior nasal packing (48-72 h)
↓ fails
Posterior packing (48 h) + admit + monitoring
↓ fails
↙ ↘
ESPAL (1st choice) Embolization (poor surgical
candidate, tumour, trauma,
carotid blowout)
↓ fails
IMAL / Ethmoidal artery ligation (by source)
↓ absolute last resort
External carotid artery ligation
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1, pp. 1224-1228
- Cummings Otolaryngology Head and Neck Surgery, pp. 940-942
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 789
Anterior ethmoidal artery anatomy in nose and its ligation
Finding Sources
Finding Sources
Searching the Web
anterior ethmoidal artery anatomy nasal cavity skull base ligation surgical technique
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have everything needed - comprehensive anatomy from Scott-Brown's and Cummings, both images, and surgical technique details. Let me compile the full response.
Anterior Ethmoidal Artery: Anatomy in the Nose and Ligation
Origin and Overview
The anterior ethmoidal artery (AEA) is a branch of the ophthalmic artery, which itself is the first branch of the internal carotid artery. It therefore belongs to the internal carotid system - in contrast to the sphenopalatine and greater palatine arteries, which are external carotid territory. This dual blood supply to the nasal cavity creates important clinical implications for managing epistaxis.
Course - Three Compartments
The AEA traverses three anatomical compartments during its course:
1. Orbital Segment
- After branching from the ophthalmic artery in the medial orbit, the AEA passes between the superior oblique and medial rectus muscles
- It exits the orbit through the anterior ethmoidal foramen in the frontoethmoidal suture line
- This orbital segment is readily visible on pre-operative coronal CT imaging
2. Ethmoidal (Skull Base) Segment - Surgically Critical
- The artery enters the ethmoid cavity and travels obliquely in a posterior-to-anterior direction
- It runs either:
- Within the bone of the skull base (most common - ~75% of cases)
- Within a mucosal mesentery hanging below the skull base (in ~20-25% of cases)
- The artery can always be found between the 2nd and 3rd lamella endoscopically - a key surgical landmark
- It then traverses intracranially through the lateral lamella of the lamina cribrosa into the olfactory fossa
- Inside the cranial cavity, it gives off anterior meningeal branches
3. Nasal Cavity Segment
- Re-enters the nasal cavity through the cribroethmoidal foramen
- Divides into anterior and posterior nasal arteries
- Each nasal artery gives lateral branches to the superior lateral nasal wall and medial branches to the nasal septum
Key Anatomical Distances (The 24-12-6 Rule)
The classic mnemonic from the anterior lacrimal crest:
| Structure | Distance from Anterior Lacrimal Crest |
|---|---|
| Anterior ethmoidal foramen | 24 mm |
| Posterior ethmoidal foramen | 12 mm further (36 mm total) |
| Optic canal | 6 mm further (42 mm total) |
Important caveat: While these distances are relatively consistent, the number of foramina is variable - multiple accessory ethmoidal arteries exist, and the posterior ethmoidal artery may even be absent. Surgeons must be aware of this variability and should not assume a single foramen for each vessel.
- Cummings Otolaryngology, p. 942
Middle Ethmoidal Artery
In approximately 30% of patients, there is a middle ethmoidal artery located between the anterior and posterior ethmoidal arteries. It tends to be:
- Unilateral
- Positioned within the skull base
- Cummings Otolaryngology, p. 934
Surgically Important Variations: The "Low-Lying" or Dehiscent AEA
In up to 25% of cases, the anterior ethmoidal artery is "low-lying" - meaning it hangs below the skull base within a mucosal mesentery rather than being protected within a bony canal. This is a major risk factor for inadvertent intraoperative injury during endoscopic sinus surgery.
Risk factors for a low-lying/dehiscent AEA:
- Presence of a supraorbital ethmoid air cell (Onodi-type variant)
- High Keros classification (Keros type 3 = deep olfactory fossa, long lateral lamella, inherently lower skull base)
- Increased distance between the anterior wall of the frontal sinus and the skull base
When the AEA is dehiscent and hangs in a mesentery, it is visible endoscopically as a vascular pedicle crossing from the lateral orbital wall to the skull base - and is at risk of being avulsed during ethmoidectomy.
- Cummings Otolaryngology, p. 941
What Happens When the AEA is Injured
The consequence depends on where the artery is transected:
| Site of Transection | Consequence |
|---|---|
| Medially (within nasal cavity / near olfactory fossa) | Epistaxis - difficult to stop due to superior location |
| Laterally (orbital side of foramen) | Proximal stump retracts into the orbit → retrobulbar hematoma (surgical emergency - requires immediate orbital decompression) |
Indications for AEA Ligation
AEA ligation is specifically indicated in:
- Skull base trauma (naso-orbito-ethmoidal fractures) causing superior/ethmoidal epistaxis
- Iatrogenic injury during FESS or skull base surgery
- Confirmed ethmoidal origin of bleeding not controlled by SPA ligation
- Anterior skull base tumor resection (prophylactic ligation of both AEA and PEA to reduce intraoperative blood loss - e.g., anterior skull base meningiomas, olfactory groove tumors)
- Adjuvant to SPA ligation when superior nasal bleeding persists
The AEA contributes minimally to nasal blood supply compared to the SPA. Ligation of ethmoidal arteries as a primary treatment for epistaxis reflects the technical ease of the open procedure rather than a logical vascular rationale. It is best used as an adjuvant to SPA ligation or when ethmoidal origin is confirmed.
- Scott-Brown's Otorhinolaryngology Vol 1, p. 1225
Surgical Approaches to AEA Ligation
1. Endoscopic Transnasal Approach
The endoscopic approach is only feasible in ~20% of cases - specifically those where the AEA lies in a mucosal mesentery accessible from within the nasal cavity.
Steps:
- Perform a complete anterior ethmoidectomy and define the ethmoid skull base
- The AEA is identified at the junction of the 2nd and 3rd lamellae, running as a fibrovascular pedicle from the lateral wall (orbit side) to the skull base
- If the artery is within a bony canal, the canal is gently drilled with a diamond burr to expose the vessel; alternatively, a curette manipulates bone fragments off the vessel
- Bipolar electrocautery on low setting is applied - equally effective as clips
- Haemostatic clips may be applied if the vessel is well isolated
- The artery is NOT transected after cauterization - transection risks retraction of the proximal stump into the orbit with consequent retrobulbar hematoma
- Frontal sinus and orbital landmarks confirm position (frontal sinus anterosuperiorly, orbit laterally)

2. Open Transorbital Approach - Lynch Incision
The preferred method when endoscopic access is not possible (most cases - ~80% where artery is within bone).
Technique:
- A medial canthal (Lynch) incision - straight vertical incision at the medial canthus, carried down to the bone of the anterior lacrimal crest
- Periosteal elevators elevate the bulbar fascia and periorbita, retracting it laterally
- The anterior ethmoidal artery is seen as a fibro-neurovascular mesentery (a "pedicle") running from the bulbar fascia into the anterior ethmoidal foramen
- The vessel is clipped and divided
- Dissection continues 12 mm posteriorly to identify the posterior ethmoidal artery (between PEA and optic canal is only 6 mm - extreme care required not to confuse PEA with the optic nerve)
- Closed with fast-absorbing gut sutures, treated with erythromycin ophthalmic ointment
Disadvantage: Leaves a visible scar at the medial canthus.
3. Precaruncular / Transcaruncular Approach (Scarless)
A newer technique offering the same orbital access without a skin scar.
Technique:
- Incision at the lacrimal caruncle (transcaruncular) or anterior to it (precaruncular)
- Dissection through superior and inferior conjunctival folds
- Horner muscle identified and left undissected (to avoid epiphora)
- Periorbita posterior to its insertion is incised vertically to expose the lamina papyracea
- Blunt posterior elevation reveals the ethmoidal neurovascular foramina sequentially
- Vessels ligated and divided
- Closed with fast-absorbing gut sutures
Advantage: No visible external scar, excellent exposure identical to Lynch approach.
- Cummings Otolaryngology, pp. 941-942
Summary Comparison of Approaches
| Approach | Scar | Feasibility | Notes |
|---|---|---|---|
| Endoscopic transnasal | None | ~20% cases (mesentery only) | Do NOT transect - retraction risk |
| Lynch incision (open) | Medial canthal | All cases | Most widely used, reliable |
| Transcaruncular (open) | None | All cases | Preferred scarless alternative |
Critical Safety Points
- Never transect endoscopically without haemostatic control on both ends - the proximal orbital stump retracts and causes retrobulbar hematoma
- The 6 mm rule - only 6 mm separates the posterior ethmoidal foramen from the optic canal; do not clip what you cannot clearly identify
- Multiple foramina - additional accessory ethmoidal arteries exist and the posterior ethmoidal artery may be absent
- Both sides have overlapping supply - bilateral AEA supply means ligation may need to be bilateral in selected cases
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1, pp. 1015-1016, 1225-1226
- Cummings Otolaryngology Head and Neck Surgery, pp. 934, 941-942
Middle meatal antrostomy
Finding Sources
Finding Sources
Searching the Web
middle meatal antrostomy FESS technique uncinate process maxillary sinus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from Cummings and K.J. Lee's plus the key operative images. Let me now compile the full, detailed response.
Middle Meatal Antrostomy (MMA)
Middle meatal antrostomy is the surgical creation of an enlarged opening into the maxillary sinus via the middle meatus, performed by widening the natural maxillary ostium after uncinectomy. It is the central step of FESS for chronic maxillary sinusitis and forms the cornerstone of osteomeatal complex (OMC) surgery.
Relevant Anatomy
The Osteomeatal Complex (OMC)
The OMC is a functional concept rather than a single anatomic structure - it represents the final common drainage and ventilation pathway for the maxillary, anterior ethmoid, and frontal sinuses. Its components include:
- Uncinate process - sickle-shaped bone running anterosuperior to posteroinferior; the first structure encountered in the middle meatus on lateralizing the middle turbinate; forms the medial wall of the ethmoidal infundibulum
- Ethmoidal infundibulum - a funnel-shaped 3D space between the uncinate process medially and the lamina papyracea laterally, into which the anterior sinuses drain
- Hiatus semilunaris - a 2D slit (cleft) between the free (posterior) edge of the uncinate process and the ethmoid bulla; connects the middle meatus to the infundibulum; the entry point for surgical probes accessing the infundibulum
- Ethmoid bulla - the largest anterior ethmoidal air cell, posterior to the uncinate
- Maxillary sinus natural ostium - opens into the inferior aspect of the ethmoidal infundibulum at a 45-degree angle
- Anterior ethmoidal cells and ostia of maxillary and frontal sinuses
The OMC's exact boundaries are not defined, but it comprises structures between the medial orbital wall and the middle turbinate.
- Cummings Otolaryngology, p. 865
The Natural Maxillary Ostium
- Located in the floor of the infundibulum, lateral to the lower third of the uncinate process
- Opens at a 45-degree angle (inferolateral) - this is why angled endoscopes (30° or 45°) are mandatory for visualization
- Elliptical in shape (vs. accessory ostia which are more circular)
- Cannot be visualized without first removing the uncinate process
- Mucociliary clearance within the entire maxillary sinus is directed toward the natural ostium - this is a physiological principle with profound surgical implications
Accessory Ostia
- More circular than the natural ostium
- Commonly found in the posterior fontanelle (the membranous area of the lateral nasal wall posterior to the uncinate)
- Do not provide functional drainage - because mucociliary flow always goes toward the natural ostium
- Must be identified and incorporated into any antrostomy to prevent recirculation
Indications
- Chronic rhinosinusitis (CRS) with or without nasal polyps, refractory to medical therapy
- Acute recurrent sinusitis with OMC obstruction
- Maxillary sinus pathology requiring access (fungal ball, retention cyst, antrochoanal polyp, odontogenic sinusitis)
- Mucociliary dysfunction
- Postoperative drainage in revision surgery
Preoperative Planning
CT review is mandatory the day of surgery. Key landmarks to assess:
| Landmark | Surgical Relevance |
|---|---|
| Height and slope of skull base | Risk of intracranial penetration |
| Position of AEA relative to skull base | Injury risk during anterior ethmoidectomy |
| Shape/integrity of lamina papyracea | Orbital injury risk |
| Rotation/position of uncinate | Access to infundibulum |
| Presence of Haller cells (infraorbital ethmoid cells) | Can narrow/obstruct infundibulum |
| Presence of Onodi cells | Proximity to optic nerve |
| Frontal recess anatomy | Drainage pathway implications |
Anatomic variations predisposing to orbital or cranial complications include: lamina papyracea medial to maxillary ostium, maxillary sinus hypoplasia, fovea ethmoidalis abnormalities, lamina papyracea dehiscence, and sphenoid sinus wall variations.
- Cummings Otolaryngology, p. 878
Operative Setup
- Patient supine, head slightly elevated (reverse Trendelenburg) to reduce venous engorgement
- Topical vasoconstriction: oxymetazoline or epinephrine 1:1000 on pledgets
- Local anaesthetic infiltration (under endoscopic vision):
- Axilla of the middle turbinate (~1-1.5 mL 1% lidocaine with 1:100,000 epinephrine - until blanching)
- Anterior to the inferior uncinate process
- Optional: greater palatine block (transnasal or transoral) for posterior structures
- Eyes included in the surgical field and lubricated - must be visible at all times
- Image-guided navigation optional, but useful in revision cases or complex anatomy
- Endoscopes: 0°, 30°, 45°, 70° available
Step-by-Step Surgical Technique
Step 1 - Diagnostic Endoscopy and Middle Turbinate Medialization
- Begin with a 0° endoscope
- Identify the middle turbinate - the most important landmark
- Gently medialize the middle turbinate with a Freer elevator to expose the middle meatus
- Optional: a formal basal lamella relaxing incision at the junction of the oblique and vertical middle turbinate attachments to improve access
Step 2 - Uncinectomy (Prerequisite for MMA)
Uncinectomy is the first and most important step in FESS - the uncinate process must be completely removed before the natural ostium can be visualized.
Retrograde (preferred) technique:
- Identify the uncinate's posterior free margin (sickle-shaped; has a rolled/everted edge when polyps are present)
- Slide a ball-tipped probe into the infundibulum behind the posterior free edge to medialize the uncinate off the lamina papyracea (critical when the uncinate is atelectatic over the orbit - as in silent sinus syndrome)
- A pediatric backbiter punch is placed through the hiatus semilunaris and cuts the uncinate in an axial plane at the junction of the inferior one-third and superior two-thirds - this low incision location:
- Avoids inadvertent orbital penetration
- Corresponds to the natural maxillary ostium location
- Extend the incision anteriorly until the anterior maxillary line (junction with lacrimal bone) is reached - penetrating this bone damages the nasolacrimal duct
- Remove the middle third of the uncinate with cutting instruments or microdebrider
- The superior third may be preserved initially to protect the frontal recess from scarring
- Rotate the inferior third medially with a probe and remove with a downbiter + microdebrider
Alternative: Anterograde (sickle knife) technique
- Vertical incision on the anterior uncinate surface continued inferiorly and posteriorly along its crescent-shaped margin
Key safety point: Always verify the uncinate is being resected and not the lamina papyracea, which lies immediately lateral to it.
- Cummings Otolaryngology, p. 882; K.J. Lee's Essential Otolaryngology, p. 617
Step 3 - Identification of the Natural Maxillary Ostium
After uncinectomy, the infundibulum is exposed laterally:
- Switch to a 30° or 45° angled endoscope angled inferolaterally - this brings the maxillary ostium into optimal view
- The natural ostium is found in the floor of the infundibulum, lateral to the lower uncinate third
- It is elliptical - if only a circular opening is seen, suspect an accessory ostium in the posterior fontanelle
- If mucosal edema obscures the ostium:
- Follow the "mucus trail" with a small curved suction
- Use a double-ball (maxillary sinus seeker) probe directed inferolaterally - never laterally alone (orbital injury risk), never forced
- The inferior turbinate is a useful inferior landmark
Pitfall: Probing directly lateral risks orbital penetration. The probe must be directed inferolateral at 45°.
- K.J. Lee's Essential Otolaryngology, p. 617
Step 4 - Antrostomy Creation
- Gently dilate the natural ostium posteriorly with the seeker ball probe
- Avoid the sharp anterior aspect - this minimizes risk of circumferential scarring and stenosis
- Do not strip mucosa off the maxillary roof or medial wall - risks submucosal hematoma, delayed healing, and scarring
- Extend the ostium posteriorly with back-biting forceps or through-cutting instruments
- A straight punch can transect mucosa between medial and superior sinus walls (minimizes shearing/mucosal stripping)
- Extend inferiorly with a down-biting instrument, taking care not to injure the inferior turbinate
- Expand superiorly as needed with side-biting antrum punches
- The final result is a pear-shaped antrostomy verified with a 30° endoscope
Do NOT bite anteriorly into the natural ostium - this risks damage to the nasolacrimal duct.
- Cummings Otolaryngology, pp. 883-884; K.J. Lee's Essential Otolaryngology, p. 617
Step 5 - Incorporation of Accessory Ostia
Any accessory ostia found in the posterior fontanelle must be connected to the natural ostium to create a single confluent opening:
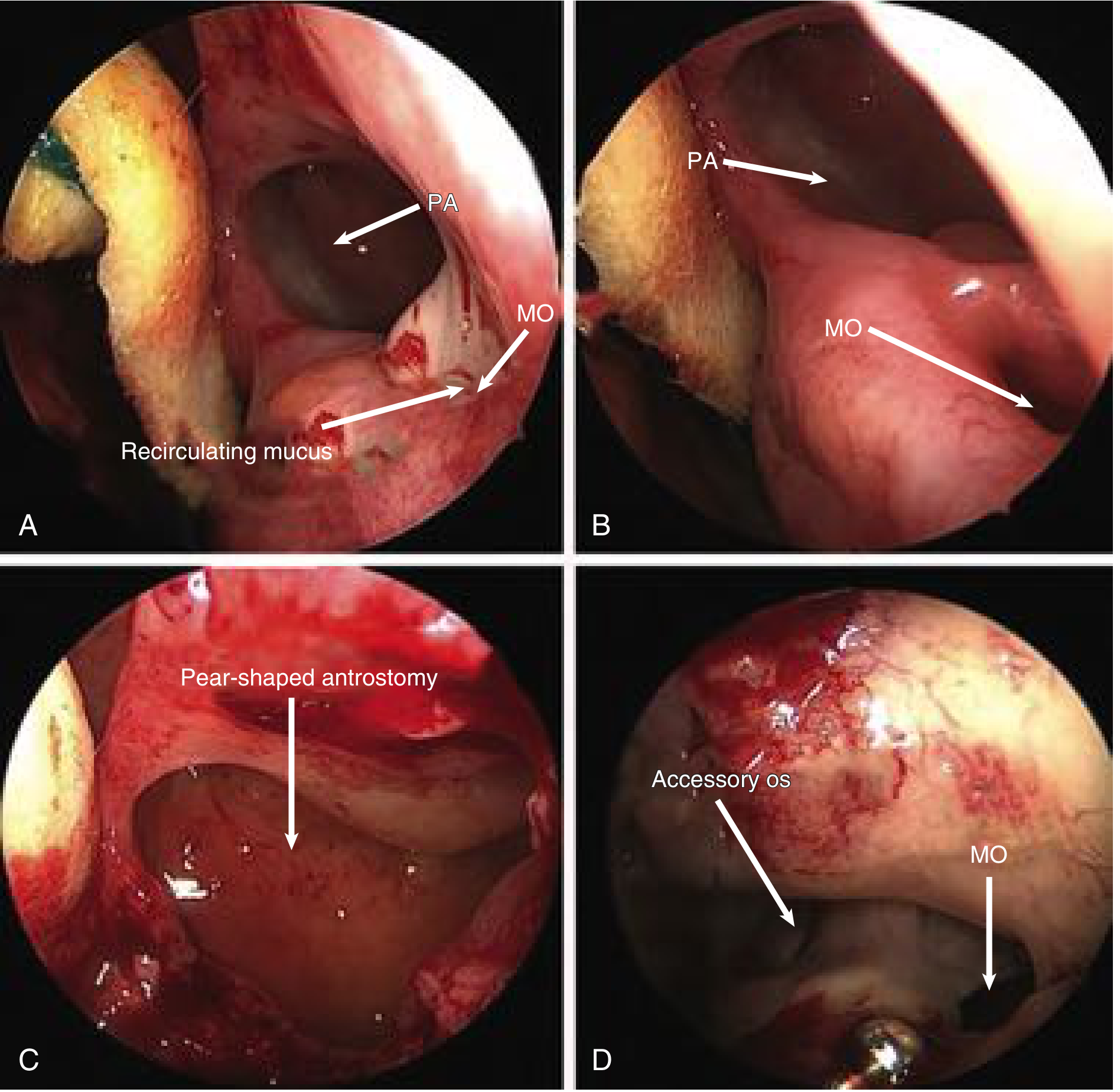
Recirculation phenomenon and correction. PA = posterior antrostomy, MO = natural maxillary ostium. - Cummings Otolaryngology, p. 883
Why this matters - the recirculation phenomenon:
If a posterior fontanelle antrostomy (or accessory ostium) is NOT connected to the natural ostium, mucus exiting the natural ostium re-enters the sinus via the posterior opening, and then exits again - an endless recirculation loop maintaining chronic infection.
Sizing the Antrostomy
The size of the antrostomy should be tailored to the extent of disease:
| Condition | Recommended Antrostomy |
|---|---|
| Mild/moderate CRS | Standard MMA - natural ostium widened posteriorly and inferiorly |
| Severe CRS, polyps, mucociliary dysfunction | Larger antrostomy |
| Mucociliary failure (e.g. cystic fibrosis, primary ciliary dyskinesia) | Mega-antrostomy (partial inferior turbinectomy + widening to nasal floor) |
| Benign sinonasal neoplasms | Modified medial maxillectomy (complete inferior turbinectomy + maximum widening) |
| Far lateral/anterior disease | Denker operation (extension beyond nasolacrimal duct to pyriform aperture) |
Inferior meatal antrostomy is rarely indicated and risks creating a separate drainage opening that bypasses mucociliary transport - it may cause recirculation and is reserved for mucociliary dysfunction conditions.
- K.J. Lee's Essential Otolaryngology, p. 618
Instruments Used
| Instrument | Purpose |
|---|---|
| 0° endoscope | Initial survey, uncinectomy |
| 30°, 45° endoscopes | Visualizing natural ostium (mandatory) |
| Pediatric backbiter punch | Retrograde uncinectomy |
| J-curette | Reflect superior uncinate medially |
| 90°-angled graspers | Remove vertical uncinate segment |
| Sidebiting instruments | Remove horizontal uncinate, expand antrostomy |
| Double-ball (maxillary seeker) probe | Locate and dilate natural ostium |
| Back-biting forceps | Posterior expansion of antrostomy |
| Down-biting instruments | Inferior expansion |
| Through-cutting instruments | Posterior expansion |
| Microdebrider | Soft tissue removal |
Common Causes of Failure
- Missed MMA - natural ostium not identified, only posterior fontanelle opened
- Maxillary ostium stenosis - circumferential scarring from mucosal stripping
- Recirculation - accessory ostium not connected to natural ostium
- Lateralized middle turbinate - adhesion to lateral wall post-operatively blocking access
- Residual ethmoidal cells - incomplete ethmoidectomy maintaining OMC obstruction
- Middle meatal adhesions
- Cummings Otolaryngology, p. 880
Key Complications
| Complication | Mechanism |
|---|---|
| Nasolacrimal duct injury | Biting anteriorly in the natural ostium, or penetrating the anterior maxillary line during uncinectomy |
| Orbital injury/fat herniation | Lateral penetration through lamina papyracea during uncinectomy or dissection |
| Epiphora/dacryocystitis | Nasolacrimal duct damage |
| Ostium stenosis | Circumferential mucosal stripping, biting anteriorly |
| Recirculation | Accessory ostium not incorporated |
| Bleeding | Sphenopalatine artery branches |
Summary of Key Principles
- The natural ostium must always be identified - opening only the posterior fontanelle does not provide functional drainage
- Mucociliary transport always heads toward the natural ostium - physiology cannot be redirected surgically
- Dilate posteriorly, never anteriorly - anterior biting risks nasolacrimal duct injury
- 30° or 45° endoscope is mandatory for ostium visualization - it opens at 45° into the infundibulum floor and cannot be seen on 0°
- Always incorporate accessory ostia - to prevent recirculation
- Preserve mucosa - stripping causes scarring and stenosis, not faster healing
- Tailor the size to disease extent and mucociliary function
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 865, 878, 882-884
- K.J. Lee's Essential Otolaryngology, pp. 617-618
Tympanostomy tubes
Finding Sources
Finding Sources
Searching the Web
tympanostomy tubes indications types complications technique otitis media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full, well-organized response.
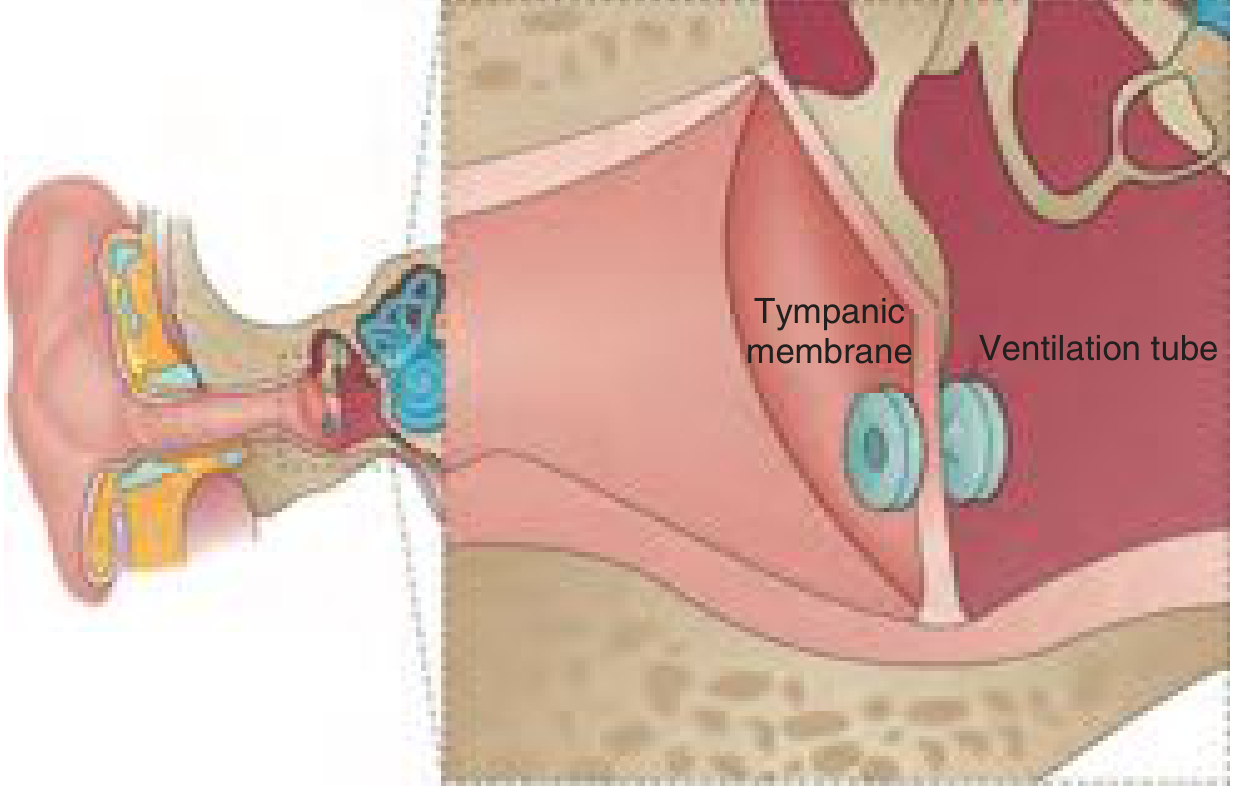
Tympanostomy Tubes (Ventilation Tubes / Grommets)
Tympanostomy tube insertion is the most commonly performed surgical procedure in children under general anaesthesia. Tubes act as a bypass for a dysfunctional Eustachian tube, ventilating the middle ear and reversing the cascade of negative pressure, effusion, and infection.
Rationale and Mechanism
Normal middle ear ventilation and pressure equilibration depends on periodic opening of the Eustachian tube. When this fails - due to inflammation, adenoid hypertrophy, anatomical abnormality (e.g. cleft palate), or Eustachian tube immaturity in young children - negative middle ear pressure develops, drawing fluid from the mucosa into the middle ear space (otitis media with effusion, OME). Persistent effusion provides a culture medium for bacteria, leading to recurrent acute otitis media (rAOM).
Tympanostomy tubes:
- Provide a surrogate pathway bypassing the under-functioning Eustachian tube
- Equalize middle ear pressure with atmospheric pressure
- Provide a drainage route for middle ear effusion (MEE) and purulent material
- Reverse OME and restore hearing
- Allow subsequent AOM episodes to present as otorrhoea rather than pain - treatable with topical antibiotics directly through the tube, avoiding systemic antibiotics
- Cummings Otolaryngology, p. 3773
Indications
1. Otitis Media with Effusion (OME / "Glue Ear")
Tympanostomy tubes are indicated when:
- Bilateral OME persisting ≥ 3 months with documented hearing loss ≥ 25 dB HL in both ears
- OME with type B (flat) tympanogram persisting ≥ 3 months in an at-risk child
- OME associated with vestibular/balance problems, behavioural problems, reduced quality of life, poor school performance
- OME in at-risk children (even if unilateral or without confirmed hearing loss): cleft palate, Down syndrome, autism, pervasive developmental disorder, craniofacial syndromes, pre-existing sensorineural hearing loss, visual impairment, speech-language delay
The effect of tubes on hearing is most marked in the first 6-9 months (mean 9.1 dB improvement at 1-3 months vs watchful waiting); the benefit diminishes thereafter as tubes extrude or as OME would have resolved spontaneously.
2. Recurrent Acute Otitis Media (rAOM)
- Defined as ≥3 AOM episodes in 6 months, or ≥4 in 12 months
- AAO-HNS guidelines recommend against tubes in rAOM when no MEE is present at time of assessment
- Recommended as an option for rAOM with MEE in one or both ears at assessment
- Modestly reduces AOM recurrences (~1 episode prevented by 6 months); effect diminishes at 12 months
- Benefit is greatest in children with MEE persisting between AOM episodes
3. Other Indications
- Eustachian tube dysfunction in adults causing chronic OME, barotrauma, or serous otitis
- Severe complications of AOM - mastoiditis, meningitis, intracranial abscess, facial nerve paralysis (as part of acute myringotomy + drainage)
- Persistent AOM despite ≥2 courses of different empiric antibiotics
- Adults with OME > 3 months with persistent aural fullness or hearing loss
- Cleft palate - high rate of Eustachian tube dysfunction; early tube insertion commonly performed
- Barotrauma - failed Valsalva in divers, aviation personnel
- Cholesteatoma retraction pockets - tubes can arrest progression by restoring middle ear pressure (though the causal relationship with cholesteatoma formation is debated)
- Cummings Otolaryngology, pp. 3773-3774; AAO-HNS 2013 guidelines
Types of Tympanostomy Tubes
All tympanostomy tubes are variations of two fundamental designs:
Short-term (Grommet) Tubes
- Small inner diameter, no lateral flange or small medial flange
- Self-extrude within 6-18 months as the TM migrates laterally
- Used for most routine cases in children
- Examples: Shepard (93% extruded by 2 years), Armstrong (~1 year clinical life; 50% extruded by 12 months, 75% by 18 months), Reuter-Bobbin (66% extruded by 2 years)
Long-term Tubes
- Larger medial flange (T-shape) or flanges on both ends that resist extrusion
- Remain in situ for years - require surgical removal when no longer needed
- Goode T-tube: only 31% extruded by 2 years
- Reserved for:
- Older children with atrophic TM
- Cleft palate (grommets extruded too quickly)
- Multiple previous sets of short-term tubes
- Conditions requiring prolonged ventilation (e.g. primary ciliary dyskinesia)
- Adults with irreversible Eustachian tube dysfunction
Material and Coating
- Fluoroplastic (Teflon) or silicone - silicone tubes were associated with longest time to first infection in a 400-patient RCT
- Long Armstrong tubes least prone to extrude among the short-term designs
- Antimicrobial coatings (silver oxide, etc.) proposed to reduce biofilm - data mixed
The time to extrusion is determined by: tube size, shape of the medial flange, presence or absence of a lateral flange, and material.
- Cummings Otolaryngology, p. 3774
Surgical Technique
Anaesthesia
- Children: general anaesthesia (inhalational), brief mask anaesthetic - no intubation required in most
- Selected children and adults: local anaesthesia (topical EMLA or lidocaine iontophoresis) in an office or clinic setting
Equipment
- Binocular operating microscope (mandatory)
- Ear speculum
- Myringotomy knife (curved radial blade) or tympanotomy lancet
- Fine suction (Frazier or Baron tip)
- Alligator forceps
- Tympanostomy tube of choice
Steps
- Remove cerumen and debris from the external canal under direct microscopic vision
- Inspect the entire tympanic membrane - identify the pars flaccida, pars tensa, handle of malleus, and light reflex; rule out pre-existing pathology
- Myringotomy incision: made in the anteroinferior quadrant of the pars tensa
- A radial incision directed toward the umbo
- Size: large enough for tube insertion with alligator forceps, but small enough to prevent premature extrusion
- The anteroinferior location avoids the ossicles (postero-superiorly), the facial nerve (posteriorly), and prevents tube migration onto the umbo
- Aspirate the MEE through the myringotomy with a fine Frazier suction
- If MEE is too thick to aspirate:
- Make a counterincision in the inferior TM, or
- Irrigate with sterile saline through the myringotomy to thin the fluid
- If MEE is too thick to aspirate:
- Insert the tube through the myringotomy incision using alligator forceps
- Advance the medial flange through the TM
- Ensure the tube sits flush and stable, with the lumen patent
Postoperative Care and Follow-Up
- First follow-up: 2-3 months post-insertion (otoscopy + hearing assessment)
- Subsequent reviews: every 6-12 months (or sooner if problems arise)
- At each visit: assess tube status (in situ, blocked, extruded), TM integrity, and hearing
- Water precautions: swimming and bathing water entry is a common parental concern. Evidence on mandatory use of ear plugs is mixed - many guidelines do not mandate plugs for surface swimming but do advise avoiding diving/submersion
- Topical antibiotic drops (e.g. ciprofloxacin/dexamethasone) at the time of insertion reduce early post-operative otorrhoea (NNTB 13 for single intraoperative dose)
- Middle ear saline washouts at surgery reduce early otorrhoea (NNTB 7)
- Cummings Otolaryngology, p. 3774
Complications and Sequelae
1. Acute Tympanostomy Tube Otorrhoea
- Most common complication: 25-75% of children develop ≥1 episode
- Results from AOM with middle ear fluid draining through the tube
- Risk factors: young age, rAOM as indication, recent recurrent URTIs, older siblings
- Management: topical antibiotic-corticosteroid drops (e.g. ciprofloxacin/dexamethasone) as first-line - these reach the middle ear directly through the tube
- If unresolved at 2 weeks: culture from tube lumen to guide therapy
- If yeast is predominant: topical clotrimazole
- Persistent or frequently recurring otorrhoea: remove the tube (foreign body reaction, biofilm)
2. Tube Blockage
- Incidence: ~6.9% (range 0-37%)
- Caused by dried blood/mucus, granulation tissue, or polyps
- Risk factors: serous effusion at surgery, delayed follow-up
- Management: suction, pick/Rosen needle, or ototopical drops for 10-14 days
- If cannot be unplugged: tube removal and reinsertion
3. Early (Premature) Extrusion
- ~3.9% of ears
- Causes: active middle ear infection pushing tube out; improper insertion into thickened TM; TM atrophy
- Requires tube reinsertion if indication persists
4. Tympanosclerosis
- ~32% after tube extrusion (range 7-64%)
- Calcification/hyalinisation of TM at insertion site - usually minimal functional significance
- No significant difference between short-term and long-term tubes
5. Focal Atrophy
- ~25% after extrusion (range 1.6-75%)
- Thin, healed TM patch at the tube site; usually functionally insignificant
6. Persistent Perforation
- Short-term tubes: 2.2% (range 0-12.3%)
- Long-term tubes: 16.6% (range 0-47%) - a major reason to avoid long-term tubes unless necessary
- Usually small; associated with only mild conductive hearing loss
- Management: myringoplasty (fat plug, paper patch, or formal fascia/perichondrium graft)
- Prerequisite: Eustachian tube function should have recovered; contralateral TM intact and infection-free for 1 year
7. Retraction Pockets
- ~3.1% after extrusion
- More relevant as a pre-existing complication of OME itself than of tubes per se
8. Cholesteatoma
- Reported incidence 0-6.5% - controversial; likely represents underlying middle ear pathology rather than a tube-specific complication
- Possible mechanism: ingrowth or transplantation of keratinised epithelium through the tube site
- Cummings Otolaryngology, pp. 3774-3775
Adjuvant Adenoidectomy
The adenoid pad acts as a nasopharyngeal reservoir for respiratory pathogens and may obstruct or impair Eustachian tube function when enlarged.
| Patient Group | Evidence |
|---|---|
| Children < 2 years with rAOM | Adenoidectomy ± tubes modestly beneficial |
| Children ≥ 4 years with OME | Adenoidectomy reduces need for tube reinsertion by ~10% |
| First set of tubes | Adenoidectomy not routinely added unless symptomatic nasal obstruction |
| Tube reinsertion | Adenoidectomy at time of second set is standard practice for ≥4-year-olds |
A meta-analysis of 10 RCTs confirmed adenoidectomy benefit is primarily in children ≥4 years for OME and <2 years for rAOM.
- Cummings Otolaryngology, p. 3773
Eustachian Tube Balloon Dilatation
Balloon dilatation of the Eustachian tube has been proposed as an adjunct or alternative for persistent OME, but current evidence does not support routine use in children.
- Cummings Otolaryngology, p. 3774
Summary Table
| Feature | Short-term (Grommet) | Long-term (T-tube) |
|---|---|---|
| Duration in situ | 6-18 months | Years |
| Persistent perforation risk | ~2.2% | ~16.6% |
| Main use | Routine OME/rAOM | Cleft palate, atrophic TM, multiple reinsertion |
| Requires surgical removal? | No (self-extrudes) | Usually yes |
| Examples | Shepard, Armstrong, Reuter-Bobbin | Goode T-tube |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 3773-3775
- AAO-HNS Clinical Practice Guideline: Tympanostomy Tubes in Children, 2013
This is a shared conversation. Sign in to Orris to start your own chat.