Incisions for neck dissection along with diagram and their advantage disadvantage according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the diagrams and textbook content needed. Let me compile a comprehensive answer.
Incisions for Neck Dissection
(Source: Cummings Otolaryngology Head and Neck Surgery, 7th ed., Chapter 118)
General Principles of Neck Incision Design
A well-planned neck incision must satisfy several requirements:
- Adequate exposure of all lymph node levels to be dissected
- Protection and coverage of the carotid artery
- Preservation of the blood supply to the neck skin (branches of the facial and occipital arteries superiorly; transverse cervical and suprascapular arteries inferiorly)
- Flaps that are broadly based (superiorly or inferiorly)
- Avoidance of trifurcations overlying the carotid sheath
- Allowance for excision of previously violated or irradiated skin when needed
- Subplatysmal flap elevation to preserve skin vascularity
Incisions that meet at right angles create skin flaps that best preserve blood supply. The ideal limbs should avoid any trifurcation directly over the carotid sheath.
Diagram 1 - Incisions for Radical and Modified Radical Neck Dissection (Fig. 118.4, Cummings)
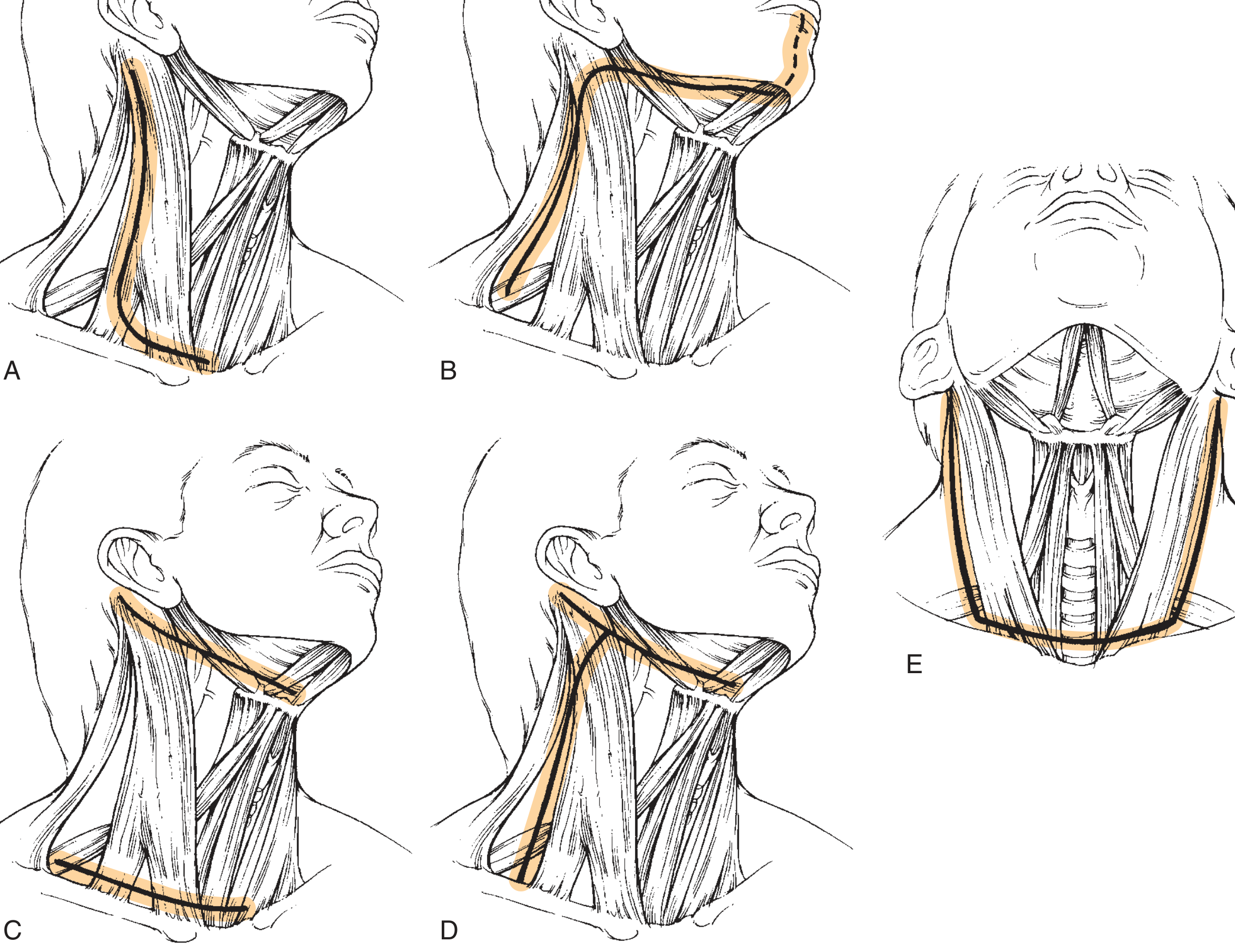
(A) Hockey Stick | (B) Boomerang | (C) McFee (two transverse) | (D) Modified Schobinger | (E) Apron (bilateral hockey stick)
Diagram 2 - Incisions for Selective Neck Dissection (SND Levels I-III) (Fig. 118.10, Cummings)
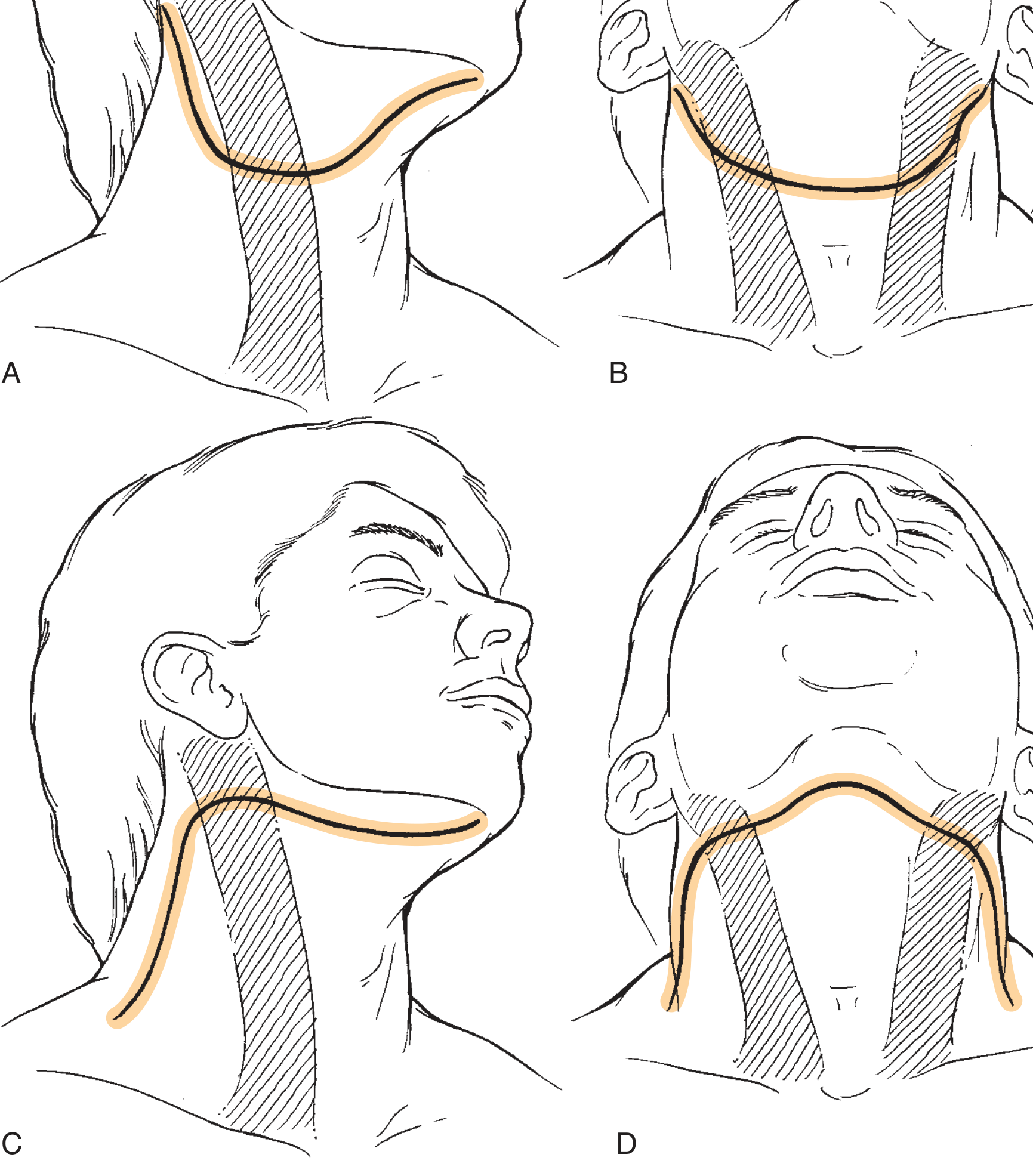
(A) Modified Apron | (B) Apron | (C) Boomerang | (D) Bilateral Boomerang
Individual Incisions: Description, Advantages, and Disadvantages
1. Hockey Stick Incision
Description: A vertical limb running along the anterior border of the sternocleidomastoid (SCM) from the mastoid tip to the clavicle, combined with a horizontal limb along a cervical skin crease. The "stick" curves posterosuperiorly behind the ear.
Advantages:
- Excellent exposure of all 5 lymph node levels (I-V)
- No trifurcation over the carotid artery - the junction is placed posteriorly
- Broadly based superior flap with good blood supply
- Can be extended across the midline as a bilateral (apron) incision
- Excellent for radical and modified radical neck dissection
- Can be extended for mandibulotomy or lip-split approaches
Disadvantages:
- Long scar that is visible along the SCM
- Less cosmetically acceptable than a transverse skin crease incision
- Not ideal in previously irradiated patients (risk of flap necrosis at angulation point)
2. Boomerang Incision
Description: A single curved transverse incision that follows the skin crease lines of the lower neck, sweeping from one side to the other in a gentle arc - shaped like a boomerang. Can be extended through the lip for mandibulotomy.
Advantages:
- Excellent exposure for all five lymph node levels
- No trifurcation over the carotid sheath
- Preferred companion to oral cavity and oropharyngeal tumor resections, especially when a mandibulotomy (lip-split) approach is required - the incision extends seamlessly through the lower lip
- Can be extended bilaterally for bilateral neck dissections (bilateral boomerang replaces the bilateral apron when lip-splitting is needed)
- Better cosmesis than hockey stick along the visible SCM region
Disadvantages:
- Somewhat less aesthetically pleasing compared to a purely transverse skin crease incision
- Not as cosmetically superior as the MacFee double-transverse incision
- Wider dissection required for adequate flap elevation
3. McFee (MacFee) Incision - Two Parallel Transverse Incisions
Description: Two separate parallel horizontal incisions placed in natural skin crease lines - one in the upper neck (below the mandible) and one in the lower neck (just above the clavicle). The central skin bridge between them is bipedicled, supplied from both ends.
Advantages:
- Excellent cosmesis - incisions fall in natural Langer's lines, scars are well concealed
- The bipedicled central skin bridge is surprisingly resistant to ischemia despite appearing to transect the dominant blood supply - studies confirm it is safe
- Preferred incision in previously irradiated patients - the bipedicled flap tolerates radiation-induced vascular compromise better than a raised single flap
- No trifurcation over the carotid
- Good carotid coverage
Disadvantages:
- Limited direct access to the midneck - the skin bridge between the two incisions limits lateral retraction and exposure in the central zone
- Technical difficulty - requires working through the tunnel created by the two incisions
- Extension of the incision to include the primary site is more difficult
- Not suitable when combined resection of the primary tumor (oral cavity, larynx) requires additional exposure - the limited access between incisions is a problem
- Wound dehiscence rate of 8% (vs. 0% for apron and 11% for triradiate incisions per one comparative study)
4. Schobinger Incision (Modified Schobinger / Conley-Modified)
Description: An H-shaped or tri-radiate incision that forms three limbs meeting at a central point. The Conley modification places the trifurcation more posteriorly and laterally (posterior to the carotid artery) rather than over it.
Advantages (Conley-modified Schobinger):
- Excellent wide exposure for comprehensive neck dissection
- Creates a large, robust anterior flap
- The modification places the trifurcation posterior to the carotid artery - reducing risk of carotid blowout if wound breaks down
- Good for bilateral neck dissections
Disadvantages:
- The original Crile single-Y and Martin double-Y designs placed the trifurcation directly over the carotid artery - a serious liability if wound breakdown occurs
- Tri-radiate incisions have the highest wound dehiscence rate (11%) in comparative studies, especially in irradiated necks
- Tenuous blood supply to posterior skin flaps
- Falls out of favor in previously irradiated patients due to highest rate of wound complications
5. Apron Incision (Bilateral Hockey Stick)
Description: Formed by extending the horizontal component of a hockey stick incision across the midline to the contralateral side, creating a wide U-shaped flap that elevates the entire anterior neck skin as one large superior flap.
Advantages:
- Lowest wound dehiscence rate (0%) in comparative studies - the widely based superior flap has excellent blood supply
- Ideal for bilateral neck dissection
- Well-suited when combined with laryngectomy (the apron flap is the standard companion incision for total laryngectomy + neck dissection)
- Excellent exposure of levels I-V bilaterally
- No trifurcation over the carotid
- Recommended for neck dissection in previously irradiated patients (superior flap vascularity)
- Good carotid protection
Disadvantages:
- Large incision - wider and more conspicuous than a unilateral approach
- The entire anterior neck skin is elevated as one flap - if devascularized, consequences are extensive
- Not needed for unilateral neck dissection where a single hockey stick suffices
6. Modified Apron Incision
Description: A smaller version of the apron incision extending only partway across the midline, providing access to levels I-III on one side.
Advantages:
- Adequate exposure for supraomohyoid selective neck dissection (levels I-III)
- Better cosmesis than full apron for unilateral procedures
- Can be extended across midline for bilateral dissection
Disadvantages:
- More limited exposure than a full apron - not suitable for level IV-V dissection
7. Attie Incision
Description: A single transverse incision used for neck dissection combined with thyroidectomy.
Advantages:
- Single incision serves both the thyroid exposure and neck dissection
- Good cosmesis - follows a skin crease line
- Eliminates need for a separate neck dissection incision
Disadvantages:
- Limited exposure compared to hockey stick or boomerang
- Use restricted to selected cases where neck dissection accompanies thyroid surgery
8. Early Historical Designs (Crile Single-Y and Martin Double-Y)
Description: The original Y-shaped incisions introduced in the early 20th century with the trifurcation placed centrally over the neck.
Advantages:
- Provided excellent exposure (the reason they were used historically)
Disadvantages:
- Trifurcation placed directly over the carotid artery - catastrophic if wound breakdown leads to carotid blowout
- Created tenuous posterior skin flaps
- Anterior flaps partially dependent on contralateral external carotid artery blood supply
- Now largely abandoned in favor of safer designs
Summary Comparison Table
| Incision | Best Used For | Key Advantage | Key Disadvantage |
|---|---|---|---|
| Hockey Stick | RND, MRND, SND (unilateral) | Excellent exposure, no trifurcation over carotid | Long visible scar |
| Boomerang | Oral cavity + oral access procedures | Extends into lip-split; no carotid trifurcation | Less aesthetic than McFee |
| MacFee (two transverse) | Previously irradiated neck | Best in irradiated patients; excellent cosmesis | Limited central access; cannot extend to primary |
| Conley-modified Schobinger | Comprehensive dissection | Large anterior flap; trifurcation placed posteriorly | Highest wound dehiscence (11%) |
| Apron (bilateral hockey stick) | Bilateral ND; ND + laryngectomy | 0% dehiscence; recommended post-RT | Large incision; wide exposure not always needed |
| Attie | ND + thyroidectomy | Single incision for both procedures | Limited to thyroid cases |
| Crile Y / Martin double-Y | Historical only | Good exposure (historical value) | Trifurcation over carotid; abandoned |
Reference: Cummings Otolaryngology Head and Neck Surgery, 7th Edition - Chapter 118 (Neck Dissection: Technique and Complications), pp. 2293-2316. Figs. 118.4 and 118.10.
This is a shared conversation. Sign in to Orris to start your own chat.