Discuss advantages disadvantages and relevance of different model in palliative care delivery Discuss different between pallitive care and hospice care when should each be introduced in care of pt with life limited disease Discuss Palliative prognosic index and palliative prognostic score ? Discuss the role of pallitive care team what are key member and how do they collaborate to improve outcomes Discuss various illness trajectory to chronic life limiting illness witnh appropriate examples of each Discuss role of patient reported outcome measure in continum of care Give the answers of DNB paper questions following standard book and pubmed and add the relevant images and flow chart
"palliative care" AND "models of care delivery"
"palliative care" AND "illness trajectory"
"palliative prognostic index" OR "palliative prognostic score"
"patient-reported outcomes" AND "palliative care" AND "quality of life"
"palliative care" AND "interdisciplinary team" AND outcomes
PMID: 37310019
"patient reported outcomes" AND "palliative care" AND continuity
Palliative Prognostic Index PPI score criteria table components palliative prognostic score PaP
models of palliative care delivery consultative integrative collaborative community based advantages disadvantages
https://www.mypcnow.org/fast-fact/palliative-prognostic-inde…
https://apm.amegroups.org/article/view/6316/html
DNB Palliative Medicine - Comprehensive Question Bank Answers
Sources: Harrison's Principles of Internal Medicine 22E, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Sleisenger & Fordtran's GI & Liver Disease, Brenner & Rector's The Kidney, Current Surgical Therapy 14E, Fuster & Hurst's The Heart 15E + PubMed (2021-2026) + PCNOW Fast Facts
QUESTION 1: Models of Palliative Care Delivery - Advantages, Disadvantages and Relevance
Background
MODEL CLASSIFICATION
A. By Provider Level
┌─────────────────────────────────────────────────────────────────────┐
│ THREE-TIER PALLIATIVE CARE PROVIDER MODEL │
├────────────────┬───────────────────────┬────────────────────────────┤
│ PRIMARY │ SECONDARY │ TERTIARY │
│ (Generalist) │ (Specialist │ (Academic/ │
│ │ Consultative) │ Research Centre) │
├────────────────┼───────────────────────┼────────────────────────────┤
│ All clinicians │ Palliative care team │ Palliative medicine units │
│ at point of │ consultation service │ affiliated with medical │
│ care │ inpatient/outpatient │ colleges; complex cases, │
│ │ │ training, research │
├────────────────┼───────────────────────┼────────────────────────────┤
│ Advantages: │ Advantages: │ Advantages: │
│ - Accessible │ - Specialist input │ - Research & training │
│ - Continuity │ - Complex symptom │ - Refractory cases │
│ - Low cost │ management │ - Protocol development │
├────────────────┼───────────────────────┼────────────────────────────┤
│ Disadvantages: │ Disadvantages: │ Disadvantages: │
│ - Skill gap │ - Limited reach │ - Highly specialized; │
│ - Burnout │ - May fragment care │ limited availability │
│ - Uneven QOL │ - Referral delays │ - High cost │
└────────────────┴───────────────────────┴────────────────────────────┘
B. By Setting / Service Model
1. CONSULTATIVE MODEL (Hospital-Based Inpatient Palliative Care Consultation)
| Aspect | Details |
|---|---|
| Setting | Inpatient hospital |
| Trigger | Request from treating team |
| Disciplines | Physician, nurse, social worker, chaplain |
- Provides expert symptom management and goals-of-care conversations for complex patients
- Reduces length of stay and ICU utilization
- Cost-effective - one study showed hospice saved 40% of healthcare costs in last month of life (Tintinalli's Emergency Medicine)
- Supports primary team without replacing them
- Standardizes access to specialist knowledge
- Reactive, not proactive; often consulted very late in illness
- Fragmented - not longitudinal; patient may not have pre-existing relationship with palliative team
- May create "hand-off" perception - patients fear abandonment by primary team
- Only 4-7% of hospitalized patients are referred to palliative care or hospice from the ED (Tintinalli's)
2. INTEGRATED / CONCURRENT CARE MODEL
- Earlier symptom control and goal-setting
- Normalizes palliative care - not synonymous with "giving up"
- Allows smooth transition to hospice without abrupt shift
- Improves quality of life and may modestly improve survival (less aggressive EOL care)
- Reduces emergency hospitalizations
- Resource intensive; requires dedicated palliative care capacity running parallel to oncology/cardiology teams
- Risk of role confusion between curative and palliative providers
- Requires training and culture change in curative teams
3. OUTPATIENT / AMBULATORY PALLIATIVE CARE CLINIC MODEL
- Longitudinal relationship with patients; serial assessment of goals
- Less stigmatizing than inpatient consultation
- Earlier introduction; patients attend while still functionally independent
- Cost-effective
- Limited in countries with sparse specialist workforce (major issue in India)
- Transportation barrier for patients with advanced disease
- After-hours coverage gaps
- Some patients too ill to travel
4. EMBEDDED INTEGRATION MODEL
- Face-to-face communication between oncologist and palliative specialist
- Rapid access; same-day consultation possible
- Referral rates increase; saves oncologist ~170 minutes per referral (Hui et al., Annals of Palliative Medicine)
- Minimizes stigma - palliative team is "part of the oncology team"
- Difficult to embed entire interdisciplinary team (space, logistics)
- Studies mostly involve single discipline (physician or nurse)
- Unclear whether superior to standalone palliative care clinic in outcomes
- High dependency on individual clinician relationships
5. HOME-BASED / COMMUNITY PALLIATIVE CARE MODEL
- Patient dies in preferred location (home); most patients prefer home death
- Reduces hospitalization and emergency department visits
- Caregiver empowerment, education and respite support
- Maintains patient dignity and autonomy in familiar surroundings
- Most cost-effective model in advanced illness
- Requires strong caregiver support at home
- Availability of 24-hour telephone support and crisis management
- Unequal access - rural and low-income populations disadvantaged
- Logistics of medication supply (injectable opioids, syringe drivers)
6. HOSPICE CARE MODEL (Residential / Inpatient Hospice)
7. DISEASE-FOCUSED / CONDITION-SPECIFIC PALLIATIVE CARE
Summary Comparison Table
| Model | Best for | Key Advantage | Key Limitation |
|---|---|---|---|
| Consultative (inpatient) | Complex hospital admissions | Specialist expertise | Late referrals, reactive |
| Integrated/concurrent | Early advanced illness | Improves survival + QoL | Resource intensive |
| Outpatient clinic | Ambulatory patients | Longitudinal, early | Access barriers |
| Embedded | Oncology/cardiology clinics | Rapid access, co-location | Partial team only |
| Home/community | Most advanced cancer, heart failure | Patient preference, cost | Caregiver dependent |
| Hospice | Dying (≤6 months) | Comfort-focused, holistic | Forfeits curative Rx |
| Disease-specific | CKD, HF, COPD | Disease pathway integration | Siloed care |
QUESTION 2: Palliative Care vs Hospice Care - Differences and When to Introduce Each
Definitions
Differences - Detailed Comparison
| Parameter | Palliative Care | Hospice Care |
|---|---|---|
| Eligibility | No specific criteria; any life-threatening illness at any stage | ≤6 months prognosis if disease follows its usual course |
| Concurrent disease treatment | YES - given alongside chemotherapy, dialysis, surgery | NO (in US Medicare model) - patient foregoes life-prolonging treatments |
| Stage/prognosis | Any stage, any prognosis | Terminal; prognosis ≤6 months |
| Setting | Hospital, ICU, outpatient, home, long-term care | Home (commonest), residential hospice, inpatient hospice |
| Goal | Relieve suffering + support curative/disease-modifying goals | Comfort, dignity, quality of death |
| Reimbursement | Via standard Medicare/Medicaid (specialty care billing) | Capitated (Medicare Hospice Benefit in USA = ~$190/day for all expenses) |
| Team | Consulting alongside primary team | Interdisciplinary team is primary care team |
| Duration | As long as needed | Until death; can be extended by recertification |
| All PC is hospice? | No | Yes - "All hospice care is palliative care, but not all palliative care is hospice" (Sleisenger & Fordtran) |
The Concept of Transition - Flowchart
DISEASE DIAGNOSIS
│
▼
┌───────────────────────────────────────────────────────────────────┐
│ CONCURRENT (INTEGRATED) PALLIATIVE CARE │
│ - Symptom management, goals of care, psychosocial support │
│ - Runs ALONGSIDE curative / disease-modifying treatment │
│ - Introduced at ANY stage of life-limiting illness │
└────────────────────────────────┬──────────────────────────────────┘
│
Disease progresses; prognosis ≤6 months
│
▼
┌───────────────────────────────────────────────────────────────────┐
│ HOSPICE CARE │
│ - Disease-modifying treatment stopped or not desired │
│ - Goal: comfort, dignity, peace │
│ - Interdisciplinary team as primary care team │
│ - Includes bereavement support for family post-death │
└───────────────────────────────────────────────────────────────────┘
│
▼
DEATH
│
▼
BEREAVEMENT SUPPORT (13 months)
When to Introduce Palliative Care in Life-Limiting Disease
- Length of stay ≥7 days with no pending discharge plan
- Admission from long-term care facility
- Patient/family requests for medically ineffective care
- DNR order conflicts
- Two or more hospitalizations for same illness within 3 months
- Stage IV cancer (any type) or Stage III lung/pancreatic cancer
- Uncontrolled symptoms: pain, dyspnea, delirium, nausea, psychological distress
- Uncertainty regarding prognosis
- Progressive incurable cancer (any stage IV)
- End-stage COPD/Heart failure with symptoms at rest despite therapy
- Advanced dementia with impaired mobility and communication
- Advanced CKD unwilling/unable to continue dialysis
- ALS/MND with bulbar symptoms or ventilator dependence
When to Introduce HOSPICE Care
- Physician certifies survival ≤6 months if disease follows normal course
- Goal of treatment is comfort (palliative), not curative
- Patient willing to forgo active disease-modifying treatment (US Medicare model)
- Declining functional status (PPS ≤40%)
- Weight loss >10% over 6 months
- Recurrent infections, progressive dysphagia
- Patient/family goal is comfort
QUESTION 3: Palliative Prognostic Index (PPI) and Palliative Prognostic Score (PaP)
Overview
A. PALLIATIVE PROGNOSTIC INDEX (PPI)
| Variable | Finding | Score |
|---|---|---|
| Palliative Performance Scale (PPS) | 10-20% | 4.0 |
| 30-50% | 2.5 | |
| ≥60% | 0 | |
| Oral Intake | Severely reduced (≤mouthfuls) | 2.5 |
| Moderately reduced (>mouthfuls but reduced) | 1.0 | |
| Normal | 0 | |
| Edema | Present | 1.0 |
| Absent | 0 | |
| Dyspnea at Rest | Present | 3.5 |
| Absent | 0 | |
| Delirium | Present | 4.0 |
| Absent | 0 | |
| TOTAL | Maximum | 15 |
| PPI Score | Predicted Survival | Sensitivity | Specificity |
|---|---|---|---|
| ≤2 | >6 weeks (median 155 days) | - | - |
| >2 to ≤4 | 6 weeks likely (median 89 days) | - | - |
| >4 to ≤6 | Shortened (18-21 days median) | 80% | 77% |
| >6 | <3 weeks (median 5 days) | 80% | 85% |
- PPI >6 = best for predicting <3-week survival (sensitivity 68%, specificity 80%)
- PPI >4 = best for predicting <6-week survival (sensitivity 72%, specificity 74%)
- PPI performs comparably to clinician predicted survival for <30-day mortality
- Major advantage: does NOT require blood tests (unlike PaP)
- Simple bedside tool; no lab work required
- Does not require invasive tests
- Easily implementable in multiple settings (home, hospice, acute care)
- Good sensitivity/specificity for short-term (3-6 week) prognosis
- Primarily validated in cancer patients
- May not reflect prognosis in organ failure or dementia trajectories
- Does not provide probability (only categorical groups)
- Less accurate for longer-term prognostication (>6 weeks)
B. PALLIATIVE PROGNOSTIC SCORE (PaP Score)
| Variable | Finding | Score |
|---|---|---|
| Dyspnea | No | 0 |
| Yes | 1.0 | |
| Anorexia | No | 0 |
| Yes | 1.5 | |
| Karnofsky Performance Score (KPS) | ≥30 | 0 |
| ≤20 | 2.5 | |
| Clinical Prediction of Survival (CPS) | >12 weeks | 0 |
| 11-12 weeks | 2.0 | |
| 9-10 weeks | 2.5 | |
| 7-8 weeks | 2.5 | |
| 5-6 weeks | 4.5 | |
| 3-4 weeks | 6.0 | |
| 1-2 weeks | 8.5 | |
| Total White Blood Count (WBC) | Normal (≤8,500) | 0 |
| High (8,501-11,000) | 0.5 | |
| Very high (>11,000) | 1.5 | |
| Lymphocyte % | Normal (20-40%) | 0 |
| Low (12-19.9%) | 1.0 | |
| Very low (<12%) | 2.5 | |
| TOTAL | Maximum | 17.5 |
| Group | PaP Score | 30-Day Survival Probability |
|---|---|---|
| A | 0-5.5 | >70% |
| B | 5.6-11 | 30-70% |
| C | >11 | <30% |
- Incorporates clinician's gestalt (CPS) which adds validated prognostic weight
- Provides 30-day survival probability - clinically actionable timeframe
- Validated in large prospective studies; validated in non-cancer diagnoses
- Includes inflammatory markers (WBC, lymphocyte%) reflecting systemic disease burden
- Can identify patients for hospice referral and goals-of-care planning
- Requires a full blood count - not always available in home/hospice setting
- CPS component introduces clinician subjectivity (though this is actually validated)
- More complex to calculate than PPI
- Only provides 30-day probability, not longer-term prognosis
- Primarily validated in cancer; less data in COPD, heart failure, dementia
Comparison: PPI vs PaP
| Feature | PPI | PaP |
|---|---|---|
| Variables | 5 (clinical only) | 6 (includes labs + CPS) |
| Lab tests required | No | Yes (CBC) |
| Clinician gestalt | No | Yes (CPS is core component) |
| Prognosis provided | Categorical (<3 wks, <6 wks) | 30-day probability (3 groups) |
| Max score | 15 | 17.5 (D-PaP: 19.5) |
| Setting feasibility | Home, inpatient, hospice | Inpatient, outpatient (needs CBC) |
| Validated population | Cancer | Cancer (+ limited non-cancer) |
| 2023 meta-analysis | PMID 37310019 (39 studies, n=19,714) | Validated in large prospective studies |
Clinical Application Flowchart
Patient with advanced life-limiting illness
│
▼
Need prognostic estimation?
│
┌────────┴────────┐
│ │
CBC available? CBC not available /
│ Home/Hospice setting
▼ │
PaP Score ▼
(30-day survival PPI Score
probability) (Weeks to live,
│ categorical)
▼ │
Groups A/B/C PPI ≤2 / 2-4 / 4-6 / >6
│ │
▼ ▼
Goals of care Hospice referral /
discussion, Goals of care /
hospice referral Family meeting
QUESTION 4: Role of the Palliative Care Team - Key Members and Collaboration
Team Philosophy
Key Team Members and Their Roles
┌─────────────────────────────────────────────────────────────────────┐
│ INTERDISCIPLINARY PALLIATIVE CARE TEAM │
│ │
│ ┌──────────────────┐ ┌──────────────────┐ │
│ │ PHYSICIAN │ │ NURSE/NP │ │
│ │ - Diagnosis │ │ - Symptom │ │
│ │ - Prognosis │ │ monitoring │ │
│ │ - Prescribing │ │ - Patient │ │
│ │ - Goals of care │ │ education │ │
│ │ conversations │ │ - Family support │ │
│ └──────────────────┘ └──────────────────┘ │
│ │
│ ┌──────────────────┐ ┌──────────────────┐ │
│ │ SOCIAL WORKER │ │ CHAPLAIN / │ │
│ │ - Psychosocial │ │ SPIRITUAL CARE │ │
│ │ assessment │ │ - Existential │ │
│ │ - Family │ │ distress │ │
│ │ counselling │ │ - Meaning-making │ │
│ │ - Resource │ │ - Rituals, faith │ │
│ │ coordination │ │ - Non-religious │ │
│ └──────────────────┘ │ patients │ │
│ └──────────────────┘ │
│ ┌──────────────────┐ ┌──────────────────┐ │
│ │ BEREAVEMENT │ │ ALLIED HEALTH │ │
│ │ COUNSELLOR │ │ (Physio, OT, │ │
│ │ - Post-death │ │ Dietitian, │ │
│ │ family support │ │ Pharmacist, │ │
│ │ - 13-month │ │ Psychologist) │ │
│ │ follow-up │ │ │ │
│ └──────────────────┘ └──────────────────┘ │
│ │
│ PRIMARY MEDICAL TEAM (Collaborating) │
└─────────────────────────────────────────────────────────────────────┘
Detailed Role of Each Member
1. Palliative Care Physician
- Comprehensive assessment across physical, psychological, social, and spiritual domains
- Prognostication and communication (using SPIKES, GUIDE, BREAKS frameworks)
- Prescribing: pain (opioids, co-analgesics), dyspnea, delirium, nausea
- Advance care planning and Advance Directives
- Leadership of interdisciplinary team meetings
- Tools used: Edmonton Symptom Assessment Scale (ESAS), Memorial Symptom Assessment Scale, PHQ-9, GAD-7 (Harrison's 22E)
2. Palliative Care Nurse / Nurse Practitioner
- Daily symptom assessment and titration of medications
- Wound care, syringe driver management
- Patient and family education - what to expect
- Night/weekend on-call - continuity of care
- Coordinate transition between settings
- In nurse-led models (CONNECT trial, PMID 34515737), an oncology nurse-led primary palliative care intervention significantly improved patient outcomes
3. Social Worker
- Financial assessment, insurance navigation
- Advance care planning support
- Family meeting facilitation
- Caregiver burden assessment and respite planning
- Community resource coordination (transport, meals)
4. Chaplain / Spiritual Care Provider
- Assess spiritual distress and unmet spiritual needs
- Support patients across religious and non-religious belief systems
- Support meaning, legacy, forgiveness, reconciliation
- Assist with rituals, religious rites
- Spiritual care is a distinct domain from psychological support
5. Bereavement Counsellor
- Starts family support BEFORE the death
- Provides structured bereavement follow-up post-death (typically 13 months)
- Identifies complicated grief requiring referral to psychiatry
6. Pharmacist
- Medication reconciliation and deprescribing (stopping futile medications)
- Opioid dose optimization and rotation
- Drug interaction checks in polypharmacy
7. Physiotherapist / Occupational Therapist
- Preserve function for as long as possible
- Assistive device provision
- Fatigue management
- Home environment adaptation for safety
How the Team Collaborates to Improve Outcomes
- All members discuss each patient; shared formulation of care plan
- In ICU settings: structured palliative care intervention + interdisciplinary family meeting within 72 hours improves outcomes (Miller's Anesthesia 10E)
- Single, unified care plan visible to all disciplines
- Prevents duplication and communication errors
- SPIKES: Set up - Perception - Invitation - Knowledge - Emotions - Summary
- Serious Illness Conversation Guide
- Used in family meetings with all team members present (Harrison's 22E)
- Ensure medical information is complete and understood
- Explore what patient/family hopes for; identify realistic goals
- Share all options
- Respond empathetically to emotions
- Make a recommendation based on goals
- Establish a concrete plan
- Follow up and reassess goals continuously
- Pain scores, symptom burden (ESAS)
- Days at home vs. hospital
- Patient satisfaction, family satisfaction
- Bereavement outcomes
- Temel et al. JAMA 2024 (PMID 38824442): Stepped palliative care for advanced lung cancer - showed equivalent outcomes with a tiered approach, reducing specialist burden
QUESTION 5: Illness Trajectories in Chronic Life-Limiting Illness
Trajectory 1: SUDDEN DEATH (~15% of deaths)
- Massive myocardial infarction (ventricular fibrillation)
- Massive pulmonary embolism
- Severe polytrauma (RTA)
- Spontaneous subarachnoid haemorrhage
- Sudden cardiac arrest (VF/VT)
- No opportunity for advance care planning in the terminal event
- Palliative care focuses on resuscitation decisions, ICU withdrawal protocols, family support post-death
- Preventive advance directives important
- Bereavement support for families crucial
Trajectory 2: TERMINAL ILLNESS (Cancer Trajectory) (~25-30%)
- Metastatic solid organ carcinomas (lung, colorectal, breast, pancreatic cancer)
- Haematological malignancies (multiple myeloma, AML)
- Stage IV cancer of any type
- Clear window for advance care planning while patient is still functional
- Palliative Performance Scale (PPS) most studied tool in this trajectory
- Integrated palliative care from cancer diagnosis; transition to hospice in final weeks
- ESAS, PPI and PaP most validated in this trajectory
- Early palliative care improves both QoL and survival (Temel, NEJM 2010)
Trajectory 3: ORGAN FAILURE TRAJECTORY (~25-30%)
- Chronic Heart Failure (HF) - repeated decompensations
- COPD with acute exacerbations requiring ICU admission
- Cirrhosis with repeated variceal bleeds, hepatic encephalopathy, SBP
- End-stage renal disease
- Advanced HIV
- Difficult timing - patient may appear to be doing well between exacerbations
- Clinicians hesitant to label as "dying" (each acute episode seems treatable)
- ICU admissions may be inappropriate in later stages
- Surprise question is particularly useful
- Parallel planning: treat acute exacerbation AND prepare for possibility of death
- Implanted devices (ICD, LVAD) - deactivation planning is necessary
- ESC 2021 and AHA/ACC/HFSA 2022 heart failure guidelines both recommend early palliative care in NYHA III-IV
Trajectory 4: FRAILTY / DEMENTIA TRAJECTORY (~25-30%)
- Advanced dementia (Alzheimer's disease, Lewy body dementia)
- Frailty syndrome in elderly
- Malnutrition and sarcopenia in the elderly
- Advanced Parkinson's disease
- Progressive neurodegenerative diseases (ALS, Huntington's)
- Advance directives essential - patient loses capacity progressively
- Feeding decisions (PEG tubes in dementia - evidence shows harm, not benefit)
- Surrogate decision-makers require extensive support
- Hospitalization is often not appropriate for terminal events (pneumonia in severe dementia)
- FAST scale for dementia staging
- In 2025, Chang et al. (JAMA Netw Open, PMID 40366652) defined referral criteria for specialist palliative care in dementia
Summary - Trajectory Comparison Table
| Trajectory | Pattern | Examples | Key Challenge | Palliative Care Timing |
|---|---|---|---|---|
| Sudden death | Abrupt | MI, Trauma | No warning | Advance directives, bereavement |
| Terminal illness (cancer) | Gradual decline | Solid tumours | Transition timing | From diagnosis; hospice in final weeks |
| Organ failure | Episodic | CHF, COPD, CKD | Unpredictable | Early; parallel planning |
| Frailty/Dementia | Prolonged low function | Dementia, frailty | Capacity, surrogate decisions | Early; surrogate engagement |
QUESTION 6: Role of Patient-Reported Outcome Measures (PROMs) in Continuum of Care
Definition
Why PROMs are Especially Important in Palliative Care
Key PROMs Used in Palliative Care
| PROM | Full Name | Domains | Use |
|---|---|---|---|
| ESAS-r | Revised Edmonton Symptom Assessment Scale | 10 symptoms: pain, fatigue, nausea, depression, anxiety, drowsiness, dyspnea, appetite, wellbeing, others | Daily/clinic symptom monitoring |
| MSAS (condensed) | Memorial Symptom Assessment Scale | Symptom frequency, severity, distress | Comprehensive symptom burden |
| PROMIS | Patient-Reported Outcomes Measurement Information System (NIH) | Physical function, fatigue, pain, social health, mental health | Research; cross-disease comparison |
| IPOS | Integrated Palliative care Outcome Scale | 10 physical + emotional + communication items | Validated across settings (cancer + non-cancer) |
| PaO | Palliative care Outcomes Scale | 10 items; symptom, family anxiety, practical concerns | Routine clinical use in PC |
| PHQ-9 | Patient Health Questionnaire-9 | Depression screening | Psychological domain |
| GAD-7 | Generalized Anxiety Disorder 7 | Anxiety | Psychological domain |
| FACT-G | Functional Assessment of Cancer Therapy - General | Physical, social/family, emotional, functional wellbeing | Oncology QoL |
| MD Anderson Brief Symptom Inventory | - | 4 core symptoms | Brief; feasible in sick patients |
Role of PROMs Across the Care Continuum
DISEASE DIAGNOSIS
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ EARLY PHASE: Baseline PROM Assessment │
│ - Establish pre-treatment symptom baseline (ESAS-r, PROMIS) │
│ - Identifies unmet needs early (depression, fatigue) │
│ - Triggers early palliative care referral if burden high │
└──────────────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ TREATMENT / DISEASE-MODIFYING PHASE: Serial PROM Monitoring │
│ - Detect treatment-related symptom burden (chemotoxicity) │
│ - Compare symptom burden with expected trajectory │
│ - Inform dose modifications and supportive care needs │
│ - CONNECT trial (PMID 34515737): nurse-led PROM-guided │
│ palliative care improved outcomes in advanced cancer │
└──────────────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ ADVANCED / PALLIATIVE PHASE: Goal-Directed PROM Use │
│ - Align PROMs with patient's personal goals of care │
│ - Daily ESAS to monitor symptom control; guide opioid titration │
│ - IPOS for holistic assessment (physical + emotional + │
│ communication domains) │
│ - Stepped palliative care (JAMA 2024, PMID 38824442): │
│ PRO-guided stepped interventions showed equivalent outcomes │
└──────────────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ END-OF-LIFE / HOSPICE PHASE: Comfort-Focused PROMs │
│ - Simplified instruments (2-3 item tools) due to cognitive │
│ decline and fatigue │
│ - Proxy PROMs (family-reported) when patient cannot respond │
│ - Measure: pain at rest, dyspnea, agitation, mouth care │
│ - After death: Family-reported satisfaction with care (QoD) │
└──────────────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────────────┐
│ BEREAVEMENT PHASE: Family/Caregiver PROMs │
│ - Caregiver burden assessment (ZBI - Zarit Burden Inventory) │
│ - PHQ-9/GAD-7 for family members at risk of complicated grief │
└─────────────────────────────────────────────────────────────────────┘
Benefits of PROMs in Palliative Care
- Improved symptom detection: Patients disclose symptoms in questionnaires they might not mention to clinicians (depression, sexual dysfunction, existential distress)
- Monitoring treatment response: Objective evidence of whether palliative interventions are working
- Facilitating communication: PRO data displayed in clinic creates structured opening for difficult conversations
- Research and quality improvement: Standardized comparison across institutions and interventions
- Regulatory and reimbursement: FDA increasingly requires PROMs as endpoints in palliative drug trials
- Electronic PROMs (ePROMs): Real-time symptom reporting between visits; triggers alerts to nursing team (systematic review PMID 38812853 confirms benefits but highlights implementation challenges)
- Empowering patients: Gives patients a voice; aligns care with patient priorities rather than clinician assumptions
Limitations of PROMs in Palliative Care
- Cognitive impairment/delirium limits self-reporting in final weeks
- Questionnaire burden in very ill patients (fatigue, dyspnea)
- Response shift - patients adapt expectations downwards, altering PROM scores
- Cultural and literacy barriers - especially in Indian context
- Proxy respondents (family members) may not accurately reflect patient experience
- Not all PROMs validated across languages and cultures
- Electronic systems require infrastructure; rural access barriers
ePROM / Electronic PROM Systems
- Advantages: Real-time data, remote monitoring between visits, alert systems for deteriorating symptoms, reduced paper burden
- Disadvantages: Digital divide (older/rural patients), alert fatigue for clinicians, integration challenges with EMR, data privacy
- Recommendation: ePROMs should supplement, not replace, clinical assessment
Summary Quick Reference
| Topic | Key Reference | Key Tool/Concept |
|---|---|---|
| PC vs Hospice difference | Sleisenger & Fordtran; Harrison's 22E | "All hospice is PC; not all PC is hospice" |
| Models of PC delivery | Hui et al. APM; NAM Perspectives | Solo > Congress > Integrated (recommended) |
| Illness trajectories | Lunney/Lynn/Hogan 2002 | 4 trajectories: sudden/cancer/organ failure/frailty |
| PPI | Morita 1999; PMID 37310019 (2023 meta) | Score >6 = <3 weeks survival |
| PaP | Pirovano 1999; PCNOW FF #124 | Groups A/B/C; 30-day survival probability |
| PROM in PC | Harrison's 22E; PMID 38812853 | ESAS-r, IPOS, PROMIS |
| Team collaboration | Sleisenger & Fordtran; Harrison's 22E | IDT meetings; SPIKES; 7-step goals process |
| When to refer | Current Surgical Therapy 14E | Surprise question + specific trigger criteria |
- 2023 Meta-analysis of PPI - 39 studies, 19,714 patients (PMID 37310019)
- CONNECT RCT - nurse-led PC - JAMA Intern Med 2021 (PMID 34515737)
- Stepped palliative care in lung cancer - JAMA 2024 (PMID 38824442)
- PC in dementia referral criteria - JAMA Netw Open 2025 (PMID 40366652)
- ePROM systems systematic review - Digit Health 2024 (PMID 38812853)
Give all 4
Convert it into pdf
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "created"
mkdir -p /tmp/workspace/palliative-care-pdf && python3 -c "from reportlab.lib import colors; print('reportlab ok')" && python3 -c "import requests; print('requests ok')" && python3 -c "from PIL import Image; print('PIL ok')"
~/palliative-care-pdf/generate_pdf.py
#!/usr/bin/env python3
"""
Generate a comprehensive DNB Palliative Medicine PDF
using ReportLab with professional formatting.
"""
import requests
import io
from PIL import Image as PILImage
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether, Image
)
from reportlab.platypus.flowables import Flowable
from reportlab.pdfgen import canvas
# ── Colours ────────────────────────────────────────────────────────────────
TEAL = colors.HexColor('#006D77')
TEAL_LIGHT = colors.HexColor('#E8F4F6')
TEAL_MID = colors.HexColor('#83C5BE')
GOLD = colors.HexColor('#B5870B')
GOLD_LIGHT = colors.HexColor('#FFF8E7')
DARK = colors.HexColor('#1A1A2E')
MID_GREY = colors.HexColor('#6B7280')
LIGHT_GREY = colors.HexColor('#F3F4F6')
RED_SOFT = colors.HexColor('#DC2626')
WHITE = colors.white
PAGE_W, PAGE_H = A4
# ── Page template with header/footer ───────────────────────────────────────
def make_page(c, doc):
c.saveState()
# Header bar
c.setFillColor(TEAL)
c.rect(0, PAGE_H - 1.2*cm, PAGE_W, 1.2*cm, fill=1, stroke=0)
c.setFillColor(WHITE)
c.setFont('Helvetica-Bold', 9)
c.drawString(1.5*cm, PAGE_H - 0.85*cm, 'DNB PALLIATIVE MEDICINE — Comprehensive Question Bank')
c.setFont('Helvetica', 8)
c.drawRightString(PAGE_W - 1.5*cm, PAGE_H - 0.85*cm, 'Based on Harrison\'s 22E · Tintinalli · Rosen\'s · Sleisenger & Fordtran · PubMed')
# Footer
c.setFillColor(TEAL)
c.rect(0, 0, PAGE_W, 0.8*cm, fill=1, stroke=0)
c.setFillColor(WHITE)
c.setFont('Helvetica', 8)
c.drawCentredString(PAGE_W/2, 0.25*cm, f'Page {doc.page}')
c.restoreState()
# ── Styles ──────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, **kw)
styles = {
'cover_title': S('cover_title', fontName='Helvetica-Bold', fontSize=28,
textColor=TEAL, alignment=TA_CENTER, spaceAfter=6),
'cover_sub': S('cover_sub', fontName='Helvetica', fontSize=14,
textColor=DARK, alignment=TA_CENTER, spaceAfter=4),
'cover_note': S('cover_note', fontName='Helvetica-Oblique', fontSize=10,
textColor=MID_GREY, alignment=TA_CENTER, spaceAfter=6),
'q_heading': S('q_heading', fontName='Helvetica-Bold', fontSize=14,
textColor=WHITE, backColor=TEAL,
leftIndent=8, rightIndent=8, spaceBefore=14, spaceAfter=6,
leading=20, borderPad=5),
'h2': S('h2', fontName='Helvetica-Bold', fontSize=12,
textColor=TEAL, spaceBefore=10, spaceAfter=4, leading=16),
'h3': S('h3', fontName='Helvetica-Bold', fontSize=11,
textColor=DARK, spaceBefore=8, spaceAfter=3, leading=14),
'h4': S('h4', fontName='Helvetica-Bold', fontSize=10,
textColor=GOLD, spaceBefore=6, spaceAfter=2),
'body': S('body', fontName='Helvetica', fontSize=9.5,
textColor=DARK, alignment=TA_JUSTIFY,
spaceAfter=4, leading=14),
'bullet': S('bullet', fontName='Helvetica', fontSize=9.5,
textColor=DARK, leftIndent=16, spaceAfter=2, leading=13,
bulletIndent=6),
'bullet2': S('bullet2', fontName='Helvetica', fontSize=9,
textColor=DARK, leftIndent=28, spaceAfter=2, leading=12,
bulletIndent=18),
'mono': S('mono', fontName='Courier', fontSize=8,
textColor=DARK, backColor=LIGHT_GREY,
leftIndent=8, rightIndent=8, spaceAfter=4, leading=11,
borderPad=4),
'ref': S('ref', fontName='Helvetica-Oblique', fontSize=8.5,
textColor=MID_GREY, spaceAfter=2, leading=12),
'highlight': S('highlight', fontName='Helvetica-Bold', fontSize=9.5,
textColor=DARK, backColor=GOLD_LIGHT,
leftIndent=8, rightIndent=8, spaceAfter=4, leading=14,
borderPad=4),
'caption': S('caption', fontName='Helvetica-Oblique', fontSize=8,
textColor=MID_GREY, alignment=TA_CENTER, spaceAfter=4),
}
def p(text, style='body'): return Paragraph(text, styles[style])
def sp(h=4): return Spacer(1, h)
def hr(): return HRFlowable(width='100%', thickness=0.5, color=TEAL_MID, spaceAfter=4, spaceBefore=4)
# ── Table helpers ────────────────────────────────────────────────────────────
def hdr_style():
return [
('BACKGROUND', (0,0), (-1,0), TEAL),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 8.5),
('FONTNAME', (1,0), (-1,-1), 'Helvetica'),
('FONTSIZE', (1,0), (-1,-1), 8.5),
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, LIGHT_GREY]),
('GRID', (0,0), (-1,-1), 0.3, TEAL_MID),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('WORDWRAP', (0,0), (-1,-1), 1),
]
def mk_table(data, col_widths, span_header=False):
ts = TableStyle(hdr_style())
if span_header:
ts.add('SPAN', (0,0), (-1,0))
ts.add('ALIGN', (0,0), (-1,0), 'CENTER')
t = Table(data, colWidths=col_widths, repeatRows=1)
t.setStyle(ts)
return t
def cell(text, bold=False, size=8.5):
style = 'Helvetica-Bold' if bold else 'Helvetica'
return Paragraph(f'<font name="{style}" size="{size}">{text}</font>', styles['body'])
# ── Image loader ─────────────────────────────────────────────────────────────
def load_image_from_url(url, width=14*cm):
try:
resp = requests.get(url, timeout=15)
resp.raise_for_status()
img_data = io.BytesIO(resp.content)
pil_img = PILImage.open(img_data)
w, h = pil_img.size
ratio = h / w
img_data.seek(0)
return Image(img_data, width=width, height=width*ratio)
except Exception as e:
return p(f'[Image could not be loaded: {e}]', 'ref')
# ════════════════════════════════════════════════════════════════════════════
# CONTENT
# ════════════════════════════════════════════════════════════════════════════
def build_story():
story = []
# ── COVER PAGE ──────────────────────────────────────────────────────────
story.append(Spacer(1, 3*cm))
story.append(p('DNB PALLIATIVE MEDICINE', 'cover_title'))
story.append(p('Comprehensive Question Bank Answers', 'cover_sub'))
story.append(sp(8))
story.append(HRFlowable(width='60%', thickness=2, color=TEAL, spaceAfter=8))
cover_items = [
'Q1 — Models of Palliative Care Delivery',
'Q2 — Palliative Care vs Hospice Care',
'Q3 — Palliative Prognostic Index (PPI) & Palliative Prognostic Score (PaP)',
'Q4 — Role of the Palliative Care Team',
'Q5 — Illness Trajectories in Chronic Life-Limiting Illness',
'Q6 — Patient-Reported Outcome Measures (PROMs)',
]
for item in cover_items:
story.append(p(f'• {item}', 'cover_sub'))
story.append(sp(16))
story.append(HRFlowable(width='60%', thickness=2, color=TEAL, spaceAfter=8))
story.append(p('Sources: Harrison\'s Principles of Internal Medicine 22E · Tintinalli\'s Emergency Medicine · Rosen\'s EM · Sleisenger & Fordtran\'s GI & Liver Disease · Brenner & Rector\'s The Kidney · Current Surgical Therapy 14E · Fuster & Hurst\'s The Heart 15E · PubMed 2021–2026', 'cover_note'))
story.append(p('July 2026', 'cover_note'))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q1 — MODELS OF PALLIATIVE CARE DELIVERY
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 1: Models of Palliative Care Delivery — Advantages, Disadvantages and Relevance', 'q_heading'))
story.append(sp(4))
story.append(p('<b>WHO Definition:</b> Palliative care is "an approach that improves quality of life of patients and their families facing problems associated with life-threatening illness, through prevention and relief of suffering by early identification and impeccable assessment and treatment of pain and other problems — physical, psychosocial and spiritual."', 'highlight'))
story.append(sp(4))
story.append(p('MODEL CLASSIFICATION', 'h2'))
story.append(p('A. By Provider Level: Three-Tier Model', 'h3'))
tier_data = [
[cell('Level', bold=True), cell('Provider', bold=True), cell('Advantages', bold=True), cell('Disadvantages', bold=True)],
[cell('PRIMARY\n(Generalist)'), cell('All clinicians at point of care\n(GPs, nurses, ward physicians)'),
cell('Accessible; continuity; low cost; universal availability'),
cell('Skill gap; burnout risk; uneven quality of care')],
[cell('SECONDARY\n(Specialist Consultative)'), cell('Dedicated palliative care team — inpatient/outpatient consultation'),
cell('Specialist symptom management; complex goal-setting; supports primary team'),
cell('Limited reach; reactive referrals; may fragment care')],
[cell('TERTIARY\n(Academic Centre)'), cell('Palliative medicine units at medical colleges/academic hospitals'),
cell('Research & training; refractory/complex cases; protocol development'),
cell('Highly specialised; limited geographic availability; high cost')],
]
story.append(mk_table(tier_data, [2.8*cm, 4.5*cm, 4.5*cm, 4.5*cm]))
story.append(sp(6))
story.append(p('B. Service/Setting Models (Detailed)', 'h3'))
models = [
('1. Consultative Model (Hospital-Based Inpatient)',
'A specialist palliative care team provides consultation on request from the primary team within a hospital setting.',
[
'<b>Advantages:</b> Expert symptom management for complex patients; reduces LOS and ICU utilization; cost-effective (hospice saves 40% of costs in last month of life — Tintinalli\'s); supports without replacing primary team.',
'<b>Disadvantages:</b> Reactive — often consulted very late; fragmented (not longitudinal); only 4–7% of hospitalised patients are referred from the ED (Tintinalli\'s); risk of "hand-off" perception.',
'<b>Relevance:</b> Best for acute care hospitals — trigger criteria: LOS ≥7 days, uncontrolled symptoms, DNR conflicts, Stage IV cancer.',
]),
('2. Integrated / Concurrent Care Model',
'Palliative care runs simultaneously alongside disease-modifying treatment from early in the illness trajectory.',
[
'<b>Key principle (Harrison\'s 22E):</b> "Beginning palliative care many months before death... patients will often receive palliative interventions long before they are formally diagnosed as terminally ill."',
'<b>Advantages:</b> Earlier symptom control and goal-setting; normalises palliative care (not "giving up"); smooth transition to hospice; improves QoL and may modestly improve survival.',
'<b>Disadvantages:</b> Resource intensive; risk of role confusion; requires culture change in curative teams.',
'<b>Relevance:</b> Strongly supported by ASCO, ESMO, AHA/ACC. Recommended for Stage IV cancer, HF NYHA III–IV, COPD GOLD 3–4, advanced CKD.',
]),
('3. Outpatient / Ambulatory Clinic Model',
'Dedicated palliative care clinic operating alongside oncology or subspecialty outpatient services.',
[
'<b>Advantages:</b> Longitudinal relationship; less stigmatising than inpatient consultation; earlier introduction; patients are still functionally independent; cost-effective.',
'<b>Disadvantages:</b> Limited by sparse specialist workforce (major issue in India); transportation barrier for advanced disease; after-hours coverage gaps.',
]),
('4. Embedded Integration Model',
'Palliative care clinician co-located within the oncology/cardiology department (Hui et al., Annals of Palliative Medicine).',
[
'<b>Advantages:</b> Face-to-face communication; rapid/same-day access; referral rates increase; saves oncologist ~170 min per referral; reduces stigma.',
'<b>Disadvantages:</b> Difficult to embed entire IDT (space/logistics); studies mostly single discipline; unclear superiority over standalone clinic.',
]),
('5. Home-Based / Community Palliative Care Model',
'Palliative care delivered in patients\' homes by community nurses, GPs, and specialist teams with home visits.',
[
'<b>Advantages:</b> Patient dies in preferred location (home); reduces ED visits and hospitalisation; caregiver empowerment; maintains dignity in familiar surroundings; most cost-effective.',
'<b>Disadvantages:</b> Requires strong caregiver support; 24-hour coverage logistics; rural/low-income populations disadvantaged; medication supply challenges.',
]),
('6. Disease-Focused / Condition-Specific Model',
'Integrated into disease-specific pathways — e.g., kidney supportive care, heart failure palliative care, neuropalliative care.',
[
'<b>Key concept (Brenner & Rector\'s Kidney):</b> The term "kidney supportive care" has replaced "kidney palliative care" because many CKD patients have high palliative needs for years before death.',
'<b>Advantages:</b> Disease pathway integration; familiar team; reduces transition anxiety.',
'<b>Disadvantages:</b> Siloed care; may miss psychosocial/spiritual domains; variable expertise.',
]),
]
for title, desc, bullets in models:
story.append(p(title, 'h3'))
story.append(p(desc, 'body'))
for b in bullets:
story.append(p(f'• {b}', 'bullet'))
story.append(sp(4))
story.append(p('Summary Comparison Table', 'h3'))
summary_data = [
[cell('Model', bold=True), cell('Best For', bold=True), cell('Key Advantage', bold=True), cell('Key Limitation', bold=True)],
[cell('Consultative (inpatient)'), cell('Complex hospital admissions'), cell('Specialist expertise'), cell('Late referrals, reactive')],
[cell('Integrated/concurrent'), cell('Early advanced illness'), cell('Improves survival + QoL'), cell('Resource intensive')],
[cell('Outpatient clinic'), cell('Ambulatory patients'), cell('Longitudinal, early'), cell('Access barriers')],
[cell('Embedded'), cell('Oncology/cardiology clinics'), cell('Rapid access, co-location'), cell('Partial team only')],
[cell('Home/community'), cell('Most advanced cancer, HF'), cell('Patient preference, cost-effective'), cell('Caregiver dependent')],
[cell('Hospice'), cell('Dying (≤6 months)'), cell('Comfort-focused, holistic'), cell('Forfeits curative treatment')],
[cell('Disease-specific'), cell('CKD, HF, COPD'), cell('Disease pathway integration'), cell('Siloed care')],
]
story.append(mk_table(summary_data, [3.5*cm, 4*cm, 4.2*cm, 4.5*cm]))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q2 — PALLIATIVE CARE vs HOSPICE CARE
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 2: Palliative Care vs Hospice Care — Differences and When to Introduce Each', 'q_heading'))
story.append(sp(4))
story.append(p('Definitions', 'h2'))
story.append(p('<b>Palliative Care:</b> An approach that improves quality of life of patients AND their families facing problems associated with life-threatening illness — applicable at any stage, any prognosis, concurrent with curative treatment. (WHO definition, Brenner & Rector\'s The Kidney)', 'highlight'))
story.append(sp(4))
story.append(p('<b>Hospice Care:</b> Palliative care provided specifically to patients with an anticipated lifespan of ≤6 months, where the goal of care is entirely comfort-focused and disease-directed life-prolonging therapies are discontinued. "Hospice care recognises that dying is a normal life cycle event and seeks to neither unnecessarily hasten nor postpone death." (Sleisenger & Fordtran)', 'highlight'))
story.append(sp(6))
story.append(p('Detailed Differences', 'h2'))
diff_data = [
[cell('Parameter', bold=True), cell('Palliative Care', bold=True), cell('Hospice Care', bold=True)],
[cell('Eligibility'), cell('No specific criteria; any life-threatening illness at any stage'), cell('≤6 months prognosis if disease follows usual course')],
[cell('Concurrent disease treatment'), cell('YES — alongside chemotherapy, dialysis, surgery'), cell('NO (Medicare model) — patient foregoes life-prolonging treatments')],
[cell('Stage/prognosis'), cell('Any stage, any prognosis'), cell('Terminal; prognosis ≤6 months')],
[cell('Setting'), cell('Hospital, ICU, outpatient, home, long-term care'), cell('Home (commonest), residential hospice, inpatient hospice')],
[cell('Goal'), cell('Relieve suffering + support curative/disease-modifying goals'), cell('Comfort, dignity, quality of death')],
[cell('Reimbursement'), cell('Via standard Medicare/Medicaid (specialty care billing)'), cell('Capitated (Medicare Hospice Benefit ~$190/day for all expenses)')],
[cell('Team role'), cell('Consulting alongside primary team'), cell('IDT is the primary care team')],
[cell('Duration'), cell('As long as needed'), cell('Until death; extended by recertification')],
[cell('Key principle'), cell('Not all palliative care is hospice'), cell('All hospice care IS palliative care')],
]
story.append(mk_table(diff_data, [4*cm, 6.5*cm, 6*cm]))
story.append(sp(6))
story.append(p('Care Transition Flowchart', 'h2'))
flow_data = [
['DISEASE DIAGNOSIS'],
['↓'],
['CONCURRENT (INTEGRATED) PALLIATIVE CARE\nSymptom management · Goals of care · Psychosocial support\nRuns ALONGSIDE curative / disease-modifying treatment\nIntroduced at ANY stage of life-limiting illness'],
['↓ Disease progresses; prognosis ≤6 months ↓'],
['HOSPICE CARE\nDisease-modifying treatment stopped or not desired\nGoal: comfort, dignity, peace\nIDT team as primary care team\nIncludes bereavement support for family post-death'],
['↓'],
['DEATH → BEREAVEMENT SUPPORT (13 months)'],
]
ts = TableStyle([
('BACKGROUND', (0,0), (-1,0), TEAL),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('BACKGROUND', (0,2), (-1,2), TEAL_LIGHT),
('BACKGROUND', (0,4), (-1,4), colors.HexColor('#FFE4E4')),
('BACKGROUND', (0,6), (-1,6), LIGHT_GREY),
('FONTNAME', (0,0), (-1,-1), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
('BOX', (0,0), (-1,-1), 1, TEAL),
('INNERGRID', (0,0), (-1,-1), 0.5, TEAL_MID),
])
ft = Table([[Paragraph(row[0], ParagraphStyle('fc', fontName='Helvetica-Bold', fontSize=9, alignment=TA_CENTER, leading=13))] for row in flow_data],
colWidths=[15*cm])
ft.setStyle(ts)
story.append(ft)
story.append(sp(8))
story.append(p('When to Introduce Palliative Care', 'h2'))
story.append(p('<b>The Surprise Question:</b> "Would I be surprised if this patient died within 12 months?" — If NO, a palliative care consult is beneficial. Positive predictive value = 93% for identifying patients who will live longer than a year. (Current Surgical Therapy 14E)', 'highlight'))
story.append(sp(4))
story.append(p('Inpatient Referral Criteria (Current Surgical Therapy 14E — Table 1):', 'h3'))
ip_criteria = [
'Length of stay ≥7 days with no pending discharge plan',
'Admission from long-term care facility',
'Patient/family requests for medically ineffective (futile) care',
'DNR order conflicts',
'Two or more hospitalisations for same illness within 3 months',
'Stage IV cancer (any type) or Stage III lung/pancreatic cancer',
'Uncontrolled symptoms: pain, dyspnea, delirium, nausea, psychological distress',
'Uncertainty regarding prognosis (patient, family, or physician)',
]
for c_ in ip_criteria:
story.append(p(f'• {c_}', 'bullet'))
story.append(p('Outpatient Referral Criteria:', 'h3'))
op_criteria = [
'Progressive incurable cancer (any Stage IV)',
'End-stage COPD/Heart failure with symptoms at rest despite maximal therapy',
'Advanced dementia with impaired mobility and inability to communicate',
'Advanced CKD unwilling/unable to continue dialysis',
'ALS/MND with bulbar symptoms or ventilator dependence',
]
for c_ in op_criteria:
story.append(p(f'• {c_}', 'bullet'))
story.append(p('When to Introduce HOSPICE Care:', 'h3'))
story.append(p('• Physician certifies survival ≤6 months if disease follows its normal course', 'bullet'))
story.append(p('• Goal of treatment is comfort (palliative), not curative', 'bullet'))
story.append(p('• Patient/family willing to forgo active disease-modifying treatment', 'bullet'))
story.append(p('• Practical indicators: PPS ≤40%; weight loss >10% over 6 months; recurrent infections; progressive dysphagia; patient goal is comfort', 'bullet'))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q3 — PPI & PaP
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 3: Palliative Prognostic Index (PPI) and Palliative Prognostic Score (PaP)', 'q_heading'))
story.append(sp(4))
story.append(p('Prognosis is one of the three pillar tasks in clinical medicine alongside diagnosis and treatment. Accurate prognostication enables appropriate clinical decision-making, anticipatory guidance, resource utilisation, symptom management, and goals-of-care planning. (PCNOW Fast Facts #124, #444)', 'body'))
story.append(sp(4))
# PPI
story.append(p('A. PALLIATIVE PROGNOSTIC INDEX (PPI)', 'h2'))
story.append(p('<b>Development:</b> Morita et al., 1999 (Japan) — terminally ill cancer patients in a palliative care unit.', 'body'))
story.append(p('<b>Key feature:</b> Uses 5 clinically observable variables; requires NO laboratory tests — ideal for home, hospice, and resource-limited settings.', 'body'))
story.append(sp(4))
story.append(p('PPI Scoring Table', 'h3'))
ppi_data = [
[cell('Variable', bold=True), cell('Finding', bold=True), cell('Score', bold=True)],
[cell('Palliative Performance Scale (PPS)', bold=True), cell('10–20%'), cell('4.0')],
[cell(''), cell('30–50%'), cell('2.5')],
[cell(''), cell('≥60%'), cell('0')],
[cell('Oral Intake', bold=True), cell('Severely reduced (≤mouthfuls)'), cell('2.5')],
[cell(''), cell('Moderately reduced (>mouthfuls, reduced)'), cell('1.0')],
[cell(''), cell('Normal'), cell('0')],
[cell('Oedema', bold=True), cell('Present'), cell('1.0')],
[cell(''), cell('Absent'), cell('0')],
[cell('Dyspnoea at Rest', bold=True), cell('Present'), cell('3.5')],
[cell(''), cell('Absent'), cell('0')],
[cell('Delirium', bold=True), cell('Present'), cell('4.0')],
[cell(''), cell('Absent'), cell('0')],
[cell('TOTAL', bold=True), cell('Maximum'), cell('15')],
]
ppi_t = Table(ppi_data, colWidths=[5.5*cm, 8*cm, 2.5*cm])
ppi_ts = TableStyle([
('BACKGROUND', (0,0), (-1,0), TEAL),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8.5),
('ROWBACKGROUNDS', (0,1), (-1,-2), [WHITE, LIGHT_GREY]),
('BACKGROUND', (0,-1), (-1,-1), TEAL_LIGHT),
('FONTNAME', (0,-1), (-1,-1), 'Helvetica-Bold'),
('GRID', (0,0), (-1,-1), 0.3, TEAL_MID),
('ALIGN', (2,0), (2,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
])
ppi_t.setStyle(ppi_ts)
story.append(ppi_t)
story.append(sp(6))
story.append(p('PPI Interpretation', 'h3'))
interp_data = [
[cell('PPI Score', bold=True), cell('Predicted Survival', bold=True), cell('Sensitivity', bold=True), cell('Specificity', bold=True)],
[cell('≤2'), cell('Median 155 days (>6 weeks)'), cell('—'), cell('—')],
[cell('>2 to ≤4'), cell('Median 89 days (~6 weeks)'), cell('—'), cell('—')],
[cell('>4 to ≤6'), cell('Median 18–21 days (<6 weeks)'), cell('80%'), cell('77%')],
[cell('>6 ★', bold=True), cell('Median 5 days (<3 weeks)', bold=True), cell('80%'), cell('85%')],
]
story.append(mk_table(interp_data, [3*cm, 6*cm, 3*cm, 3*cm]))
story.append(p('★ PPI >6 is the most clinically useful threshold for hospice admission and goals-of-care decisions.', 'ref'))
story.append(sp(4))
story.append(p('<b>2023 Meta-Analysis (PMID 37310019, Palliat Med):</b> 39 studies, n=19,714 patients. PPI >6 best for <3-week prediction (sensitivity 68%, specificity 80%). PPI >4 best for <6-week prediction. PPI performs comparably to clinician gestalt for <30-day survival. Does NOT require blood tests — advantage over PaP.', 'highlight'))
story.append(sp(8))
# PaP
story.append(p('B. PALLIATIVE PROGNOSTIC SCORE (PaP Score)', 'h2'))
story.append(p('<b>Development:</b> Pirovano et al., 1999 (Italy) — multi-centre prospective study in cancer patients.', 'body'))
story.append(p('<b>Key feature:</b> Uniquely incorporates the clinician\'s subjective Clinical Prediction of Survival (CPS) as a major weighted component. Requires full blood count (CBC).', 'body'))
story.append(sp(4))
story.append(p('PaP Scoring Table', 'h3'))
pap_data = [
[cell('Variable', bold=True), cell('Finding', bold=True), cell('Score', bold=True)],
[cell('Dyspnoea', bold=True), cell('No'), cell('0')],
[cell(''), cell('Yes'), cell('1.0')],
[cell('Anorexia', bold=True), cell('No'), cell('0')],
[cell(''), cell('Yes'), cell('1.5')],
[cell('Karnofsky Performance Score', bold=True), cell('≥30'), cell('0')],
[cell(''), cell('≤20'), cell('2.5')],
[cell('Clinical Prediction of Survival (CPS)', bold=True), cell('>12 weeks'), cell('0')],
[cell(''), cell('11–12 weeks'), cell('2.0')],
[cell(''), cell('9–10 weeks'), cell('2.5')],
[cell(''), cell('7–8 weeks'), cell('2.5')],
[cell(''), cell('5–6 weeks'), cell('4.5')],
[cell(''), cell('3–4 weeks'), cell('6.0')],
[cell(''), cell('1–2 weeks'), cell('8.5')],
[cell('Total White Blood Count', bold=True), cell('Normal (≤8,500/mm³)'), cell('0')],
[cell(''), cell('High (8,501–11,000)'), cell('0.5')],
[cell(''), cell('Very high (>11,000)'), cell('1.5')],
[cell('Lymphocyte %', bold=True), cell('Normal (20–40%)'), cell('0')],
[cell(''), cell('Low (12–19.9%)'), cell('1.0')],
[cell(''), cell('Very low (<12%)'), cell('2.5')],
[cell('TOTAL', bold=True), cell('Maximum (D-PaP = 19.5 if delirium present)'), cell('17.5')],
]
pap_t = Table(pap_data, colWidths=[5.5*cm, 8*cm, 2.5*cm])
pap_t.setStyle(ppi_ts)
story.append(pap_t)
story.append(sp(6))
story.append(p('PaP Interpretation — 30-Day Survival Probability Groups', 'h3'))
pap_grp = [
[cell('Group', bold=True), cell('PaP Score', bold=True), cell('30-Day Survival Probability', bold=True)],
[cell('A (Good)'), cell('0 – 5.5'), cell('>70%')],
[cell('B (Intermediate)'), cell('5.6 – 11'), cell('30 – 70%')],
[cell('C (Poor)'), cell('>11'), cell('<30% → Consider hospice')],
]
story.append(mk_table(pap_grp, [3*cm, 4*cm, 9.2*cm]))
story.append(sp(6))
story.append(p('PPI vs PaP — Comparison Table', 'h2'))
comp_data = [
[cell('Feature', bold=True), cell('PPI', bold=True), cell('PaP', bold=True)],
[cell('Variables'), cell('5 (clinical only)'), cell('6 (includes labs + clinician CPS)')],
[cell('Lab tests required'), cell('No ✓'), cell('Yes (CBC required)')],
[cell('Clinician gestalt (CPS)'), cell('No'), cell('Yes — core weighted component')],
[cell('Prognosis provided'), cell('Categorical (<3 wks, <6 wks)'), cell('30-day probability (3 groups A/B/C)')],
[cell('Maximum score'), cell('15'), cell('17.5 (D-PaP: 19.5 with delirium)')],
[cell('Setting feasibility'), cell('Home, inpatient, hospice'), cell('Inpatient, outpatient (needs CBC)')],
[cell('Validated population'), cell('Cancer (primary)'), cell('Cancer + limited non-cancer data')],
[cell('Key study'), cell('PMID 37310019 (2023 meta, 39 studies, n=19,714)'), cell('Large prospective validation (Pirovano 1999 + subsequent studies)')],
]
story.append(mk_table(comp_data, [4.5*cm, 5.5*cm, 6.2*cm]))
story.append(sp(6))
story.append(p('Clinical Application Flowchart', 'h3'))
prog_flow = [
['Patient with advanced life-limiting illness — Need prognostic estimation?'],
['CBC available? / Inpatient / Outpatient CBC NOT available / Home / Hospice'],
[' PaP Score PPI Score'],
[' (30-day survival probability) (Categorical: weeks to live)'],
[' Groups A / B / C PPI ≤2 / 2–4 / 4–6 / >6'],
['Goals of care discussion · Hospice referral · Family meeting · Advance care planning'],
]
pf = Table(
[[Paragraph(r[0], ParagraphStyle('pf', fontName='Helvetica', fontSize=9, alignment=TA_CENTER, leading=13))] for r in prog_flow],
colWidths=[16*cm]
)
pf.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), TEAL),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('BACKGROUND', (0,-1), (-1,-1), TEAL_LIGHT),
('FONTNAME', (0,-1), (-1,-1), 'Helvetica-Bold'),
('ROWBACKGROUNDS', (0,1), (-1,-2), [WHITE, LIGHT_GREY]),
('GRID', (0,0), (-1,-1), 0.5, TEAL_MID),
('TOPPADDING', (0,0), (-1,-1), 7),
('BOTTOMPADDING', (0,0), (-1,-1), 7),
]))
story.append(pf)
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q4 — PALLIATIVE CARE TEAM
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 4: Role of the Palliative Care Team — Key Members and Collaboration', 'q_heading'))
story.append(sp(4))
story.append(p('"Quality care near the end of life for complex physical and psychological problems cannot be provided by a single clinician. Care is ideally provided by an interdisciplinary team that includes physicians, nurses, social workers, chaplains, and bereavement counsellors. The interdisciplinary palliative care team works in concert with, and does not seek to replace, the primary medical team." — Sleisenger & Fordtran\'s GI & Liver Disease', 'highlight'))
story.append(sp(6))
story.append(p('Key Team Members and Their Roles', 'h2'))
team_data = [
[cell('Team Member', bold=True), cell('Core Responsibilities', bold=True), cell('Key Tools / Assessments', bold=True)],
[cell('Palliative Care\nPhysician', bold=True),
cell('Diagnosis, prognosis, prescribing (opioids, co-analgesics, anti-emetics, anxiolytics); goals-of-care conversations; advance care planning; IDT meeting leadership'),
cell('ESAS-r, MSAS, PHQ-9, GAD-7, PPI/PaP, SPIKES, Serious Illness Conversation Guide')],
[cell('Palliative Care\nNurse / NP', bold=True),
cell('Daily symptom assessment; titration of medications; syringe driver management; wound care; patient and family education; night/weekend on-call; care transitions. In CONNECT trial (PMID 34515737), nurse-led primary PC significantly improved outcomes.'),
cell('Edmonton Symptom Assessment Scale (ESAS-r); functional assessment; medication administration records')],
[cell('Social Worker', bold=True),
cell('Psychosocial assessment; financial navigation; family meeting facilitation; caregiver burden assessment; respite planning; community resource coordination (transport, meals, housing)'),
cell('Zarit Burden Interview (ZBI); PHQ-9 for carers; social history; genogram')],
[cell('Chaplain /\nSpiritual Care\nProvider', bold=True),
cell('Assess spiritual distress; support meaning-making, legacy, reconciliation, forgiveness; rituals across religious and non-religious backgrounds; distinct from psychological support'),
cell('FICA spiritual assessment; HOPE questions; faith history')],
[cell('Bereavement\nCounsellor', bold=True),
cell('Structured bereavement follow-up post-death (typically 13 months); identifies complicated grief requiring psychiatric referral; family support begins before death'),
cell('Texas Revised Inventory of Grief; PHQ-9/GAD-7 for bereaved family')],
[cell('Pharmacist', bold=True),
cell('Medication reconciliation and deprescribing (stopping futile medications); opioid dose optimisation and rotation; drug interaction checks; palliative sedation protocols'),
cell('Opioid equivalence tables; Beers criteria; polypharmacy review')],
[cell('Physiotherapist /\nOT', bold=True),
cell('Preserve function as long as possible; fatigue management; assistive devices; home environment adaptation for safety; breathlessness management techniques'),
cell('Barthel Index; IADL assessment; home visit checklist')],
]
story.append(mk_table(team_data, [3.5*cm, 7.5*cm, 5.2*cm]))
story.append(sp(8))
story.append(p('How the Team Collaborates to Improve Outcomes', 'h2'))
collab_items = [
('1. Regular Interdisciplinary Team (IDT) Meetings',
'All members discuss each patient; shared formulation of care plan. In ICU settings: structured palliative care intervention + interdisciplinary family meeting within 72 hours improves outcomes (Miller\'s Anesthesia 10E). Meeting typically weekly; more frequent for complex/rapidly changing cases.'),
('2. Shared Documentation',
'Single, unified care plan visible to all disciplines. Prevents duplication and communication errors. Allows any team member to update goals and symptom burden in real time.'),
('3. Communication Frameworks',
'SPIKES: Set up - Perception - Invitation - Knowledge - Emotions - Summary. Serious Illness Conversation Guide. GUIDE, BREAKS, SHARE frameworks. Used in family meetings with all relevant team members present (Harrison\'s 22E).'),
('4. Goals of Care Process (7-step protocol — Harrison\'s 22E)',
'(1) Ensure medical information is complete and understood; (2) Explore what patient/family hopes for; (3) Share all options; (4) Respond empathetically to emotions; (5) Make a recommendation based on goals; (6) Establish a concrete plan; (7) Follow up and reassess goals continuously.'),
('5. Outcome Metrics for Team Performance',
'Pain and symptom scores (ESAS-r); days at home vs. hospital; patient satisfaction scores; family satisfaction scores; bereavement outcomes; PPS trajectory over time. Stepped palliative care (JAMA 2024, PMID 38824442): tiered IDT intervention showed equivalent outcomes with reduced specialist burden.'),
]
for title, desc in collab_items:
story.append(p(title, 'h3'))
story.append(p(desc, 'body'))
story.append(sp(4))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q5 — ILLNESS TRAJECTORIES
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 5: Illness Trajectories in Chronic Life-Limiting Illness', 'q_heading'))
story.append(sp(4))
story.append(p('The concept of illness trajectories was described by Lunney, Lynn, and Hogan (J Am Geriatr Soc, 2002) and is central to prognostication and palliative care planning in all chronic life-limiting illnesses.', 'body'))
story.append(sp(4))
# Insert the trajectory image
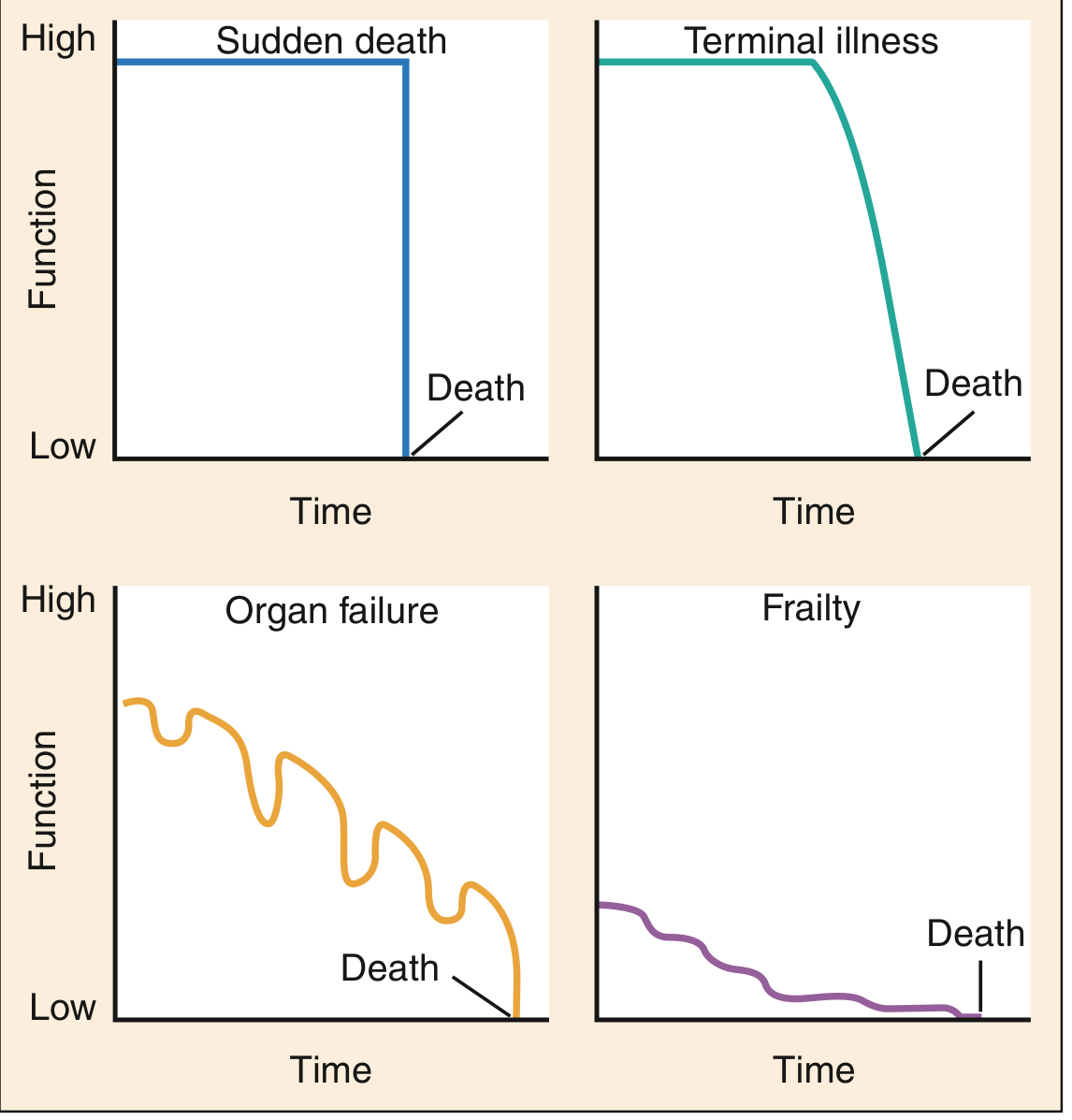
story.append(p('Fig. 1 — Four Theoretic Trajectories of Dying (Lunney JR, Lynn J, Hogan C, 2002)', 'h3'))
trajectory_img = load_image_from_url(
'https://cdn.orris.care/cdss_images/fb161cff38ca843df17f5e35777c0298081e9ddf52862be1753306cc0840d5c2.png',
width=14*cm
)
story.append(trajectory_img)
story.append(p('Source: Rosen\'s Emergency Medicine — Concepts and Clinical Practice. From: Lunney JR, Lynn J, Hogan C. Profiles of older Medicare decedents. J Am Geriatr Soc. 2002;50:1108–1112.', 'caption'))
story.append(sp(8))
trajectories = [
{
'num': '1', 'name': 'SUDDEN DEATH (~15% of deaths)',
'pattern': 'High function maintained until abrupt catastrophic event, then immediate death. No preceding decline.',
'colour': TEAL,
'examples': ['Massive myocardial infarction (VF/VT arrest)', 'Massive pulmonary embolism', 'Severe polytrauma (road traffic accident)', 'Spontaneous subarachnoid haemorrhage', 'Sudden cardiac arrest'],
'pc_implications': [
'No opportunity for advance care planning at the terminal event itself',
'Palliative care focuses on resuscitation decisions, ICU withdrawal protocols, family support post-death',
'Preventive advance directives (DNAR, living will) are critically important for high-risk patients',
'Bereavement support for families — sudden loss = high complicated grief risk',
'Palliative care may play a role in ICU if patient survives initial event but has non-survivable injury',
]
},
{
'num': '2', 'name': 'TERMINAL ILLNESS / CANCER TRAJECTORY (~25–30%)',
'pattern': 'Reasonably good function maintained for months to years, followed by a relatively brief period of accelerating decline close to death. "Patients with cancer may remain independent and functional for some time but often experience a significant decline in overall health as death nears." (Rosen\'s EM)',
'colour': colors.HexColor('#0D7377'),
'examples': ['Metastatic solid organ carcinomas (lung, colorectal, breast, pancreatic)', 'Haematological malignancies (multiple myeloma, AML)', 'Stage IV cancer of any type', 'Advanced hepatocellular carcinoma'],
'pc_implications': [
'Clear window for advance care planning while patient is still functional and has decision-making capacity',
'Palliative Performance Scale (PPS) most studied prognostic tool in this trajectory',
'Integrated palliative care from time of cancer diagnosis; transition to hospice in final weeks',
'PPI and PaP most validated in this trajectory',
'Early palliative care improves QoL AND modestly improves survival (Temel, NEJM 2010; PMID 38824442)',
'WHO analgesic ladder most applicable — step up pain management as disease progresses',
]
},
{
'num': '3', 'name': 'ORGAN FAILURE TRAJECTORY (~25–30%)',
'pattern': 'Background of declining function punctuated by acute exacerbations (some requiring hospitalisation), partial recovery with each episode, but each peak lower than the last. Prognosis unpredictable; death may occur during any exacerbation.',
'colour': colors.HexColor('#B45309'),
'examples': ['Chronic Heart Failure (HF) — repeated decompensations (Fuster & Hurst: "palliative care can be initiated at any point in the illness trajectory")', 'COPD with acute exacerbations requiring ICU admission', 'Cirrhosis with repeated variceal bleeds, HE, SBP', 'End-stage renal disease (CKD 5D)', 'Advanced HIV/AIDS'],
'pc_implications': [
'DIFFICULT timing — patient may appear well between exacerbations; clinicians hesitant to label as "dying"',
'Each acute episode seems treatable — leads to over-aggressive, under-palliative care',
'Surprise question is particularly useful in this trajectory',
'Parallel planning: treat acute exacerbation AND prepare for possibility of death in same admission',
'Implanted devices (ICD, LVAD) — deactivation planning MUST be part of advance care planning',
'ESC 2021 and AHA/ACC/HFSA 2022 HF guidelines both recommend early palliative care in NYHA III–IV',
'For CKD: "Kidney supportive care" provided throughout illness trajectory, not only terminally (Brenner & Rector)',
]
},
{
'num': '4', 'name': 'FRAILTY / DEMENTIA TRAJECTORY (~25–30%)',
'pattern': 'Prolonged period of low but relatively stable function, with very slow gradual decline over months to years. Each intercurrent illness causes a small but often irreversible drop in function. No single dramatic decline; death appears almost imperceptible.',
'colour': colors.HexColor('#6B21A8'),
'examples': ['Advanced dementia (Alzheimer\'s disease, Lewy body dementia)', 'Frailty syndrome in the elderly (polypharmacy, sarcopenia, recurrent falls)', 'Advanced Parkinson\'s disease', 'Progressive neurodegenerative diseases (ALS/MND, Huntington\'s)', 'Severe malnutrition/cachexia in the elderly'],
'pc_implications': [
'Advance directives ESSENTIAL — patient loses decision-making capacity progressively over time',
'Feeding decisions: PEG tube insertion in advanced dementia is NOT beneficial (evidence shows increased aspiration and no survival benefit)',
'Surrogate decision-makers (family) require extensive support, education, and regular family meetings',
'Hospitalisation is often inappropriate for terminal events (pneumonia in severe dementia) — goals: comfort at home/care home',
'FAST scale (Functional Assessment Staging Test) for dementia staging and hospice eligibility',
'Chang et al. 2025 (JAMA Netw Open, PMID 40366652): defined referral criteria for specialist palliative care in dementia',
'"Advanced dementia — Impaired mobility and inability to communicate health needs" = indication for palliative care (Tintinalli\'s)',
]
},
]
for traj in trajectories:
story.append(p(f"Trajectory {traj['num']}: {traj['name']}", 'h2'))
story.append(p(f"<b>Pattern:</b> {traj['pattern']}", 'body'))
story.append(p('<b>Clinical Examples:</b>', 'h4'))
for ex in traj['examples']:
story.append(p(f'• {ex}', 'bullet'))
story.append(p('<b>Palliative Care Implications:</b>', 'h4'))
for imp in traj['pc_implications']:
story.append(p(f'• {imp}', 'bullet'))
story.append(sp(6))
story.append(p('Trajectory Summary Comparison Table', 'h2'))
traj_sum = [
[cell('Trajectory', bold=True), cell('Pattern', bold=True), cell('Examples', bold=True), cell('Key Challenge', bold=True), cell('PC Timing', bold=True)],
[cell('Sudden death'), cell('Abrupt — no warning'), cell('MI, Trauma, PE'), cell('No advance warning'), cell('Advance directives; bereavement support')],
[cell('Terminal illness\n(Cancer)'), cell('Good function then rapid decline'), cell('Solid tumours, haematologic malignancy'), cell('Transition timing'), cell('From diagnosis; hospice in final weeks')],
[cell('Organ failure'), cell('Episodic; partial recovery; each peak lower'), cell('CHF, COPD, CKD, Cirrhosis'), cell('Unpredictable; clinician hesitance'), cell('Early; parallel planning')],
[cell('Frailty/Dementia'), cell('Prolonged low function; slow decline'), cell('Dementia, Frailty, ALS'), cell('Capacity loss; surrogate decisions'), cell('Early; surrogate engagement; ADs')],
]
story.append(mk_table(traj_sum, [3*cm, 4*cm, 3.8*cm, 3.5*cm, 4*cm]))
story.append(PageBreak())
# ════════════════════════════════════════════════════════════════════════
# Q6 — PROMs
# ════════════════════════════════════════════════════════════════════════
story.append(p('QUESTION 6: Role of Patient-Reported Outcome Measures (PROMs) in Continuum of Care', 'q_heading'))
story.append(sp(4))
story.append(p('<b>Definition:</b> A Patient-Reported Outcome Measure (PROM) is "any report of the status of a patient\'s health condition that comes directly from the patient, without interpretation of the patient\'s response by a clinician or anyone else." (FDA Guidance for Industry)', 'highlight'))
story.append(p('<b>Key principle:</b> PROMs capture outcomes important to <i>patients</i> rather than to healthcare providers. In palliative care, where the goal is symptom relief and quality of life — not tumour response or biomarker normalisation — PROMs are the most clinically relevant measures available. (Bailey & Love\'s Short Practice of Surgery 28E; Harrison\'s 22E)', 'body'))
story.append(sp(6))
story.append(p('Key PROMs Used in Palliative Care', 'h2'))
prom_data = [
[cell('PROM', bold=True), cell('Full Name', bold=True), cell('Domains', bold=True), cell('Use', bold=True)],
[cell('ESAS-r'), cell('Revised Edmonton Symptom Assessment Scale'), cell('10 symptoms: pain, fatigue, nausea, depression, anxiety, drowsiness, dyspnoea, appetite, wellbeing, others'), cell('Daily / clinic symptom monitoring; serial tracking')],
[cell('MSAS (condensed)'), cell('Memorial Symptom Assessment Scale'), cell('Symptom frequency, severity, distress'), cell('Comprehensive symptom burden assessment')],
[cell('PROMIS'), cell('Patient-Reported Outcomes Measurement Information System (NIH)'), cell('Physical function, fatigue, pain, social health, mental health'), cell('Research; cross-disease comparison')],
[cell('IPOS'), cell('Integrated Palliative care Outcome Scale'), cell('10 physical + emotional + communication items'), cell('Validated across settings — cancer and non-cancer')],
[cell('PaO / POS'), cell('Palliative care Outcomes Scale'), cell('10 items: symptoms, family anxiety, practical concerns'), cell('Routine clinical use in palliative care')],
[cell('PHQ-9'), cell('Patient Health Questionnaire-9'), cell('Depression screening (9 items)'), cell('Psychological domain assessment')],
[cell('GAD-7'), cell('Generalised Anxiety Disorder 7'), cell('Anxiety (7 items)'), cell('Psychological domain assessment')],
[cell('FACT-G'), cell('Functional Assessment of Cancer Therapy — General'), cell('Physical, social/family, emotional, functional wellbeing'), cell('Oncology quality of life')],
[cell('ZBI'), cell('Zarit Burden Inventory'), cell('Caregiver burden (22 items)'), cell('Family/caregiver assessment; bereavement risk')],
]
story.append(mk_table(prom_data, [2.5*cm, 4*cm, 5*cm, 4.7*cm]))
story.append(p('Harrison\'s 22E (2025) explicitly lists ESAS-r, MSAS, PROMIS, Rotterdam Symptom Checklist, Symptom Distress Scale, MD Anderson Brief Symptom Inventory, and ISAAC tool as validated instruments for palliative care assessment.', 'ref'))
story.append(sp(6))
story.append(p('Role of PROMs Across the Care Continuum', 'h2'))
prom_phases = [
('EARLY PHASE — Baseline PROM Assessment', TEAL_LIGHT,
['Establish pre-treatment symptom baseline (ESAS-r, PROMIS)',
'Identifies unmet needs early: depression, fatigue, anxiety before treatment starts',
'Triggers early palliative care referral when symptom burden is high',
'Establishes patient\'s personal goals and values while patient is fully competent']),
('TREATMENT / DISEASE-MODIFYING PHASE — Serial PROM Monitoring', LIGHT_GREY,
['Detect treatment-related symptom burden (chemotoxicity, radiotherapy mucositis)',
'Compare symptom burden with expected trajectory; identify outliers',
'Inform dose modifications and supportive care needs',
'CONNECT RCT (PMID 34515737, JAMA Intern Med 2021): nurse-led PROM-guided palliative care improved outcomes in advanced cancer patients']),
('ADVANCED / PALLIATIVE PHASE — Goal-Directed PROM Use', TEAL_LIGHT,
['Align PROMs with patient\'s personal goals of care (not clinician-defined endpoints)',
'Daily ESAS-r to monitor symptom control; guide opioid titration and anti-emetic choice',
'IPOS for holistic assessment covering physical, emotional, and communication domains',
'Stepped palliative care (JAMA 2024, PMID 38824442): PROM-guided stepped interventions showed equivalent outcomes with reduced specialist burden']),
('END-OF-LIFE / HOSPICE PHASE — Comfort-Focused PROMs', LIGHT_GREY,
['Simplified instruments (2–3 item tools) due to cognitive decline and fatigue',
'Proxy PROMs (family-reported) when patient cannot self-report',
'Measure: pain at rest, dyspnoea, agitation, mouth care adequacy',
'After death: Family-reported satisfaction with quality of dying and care']),
('BEREAVEMENT PHASE — Family/Caregiver PROMs', TEAL_LIGHT,
['Caregiver burden (ZBI) assessed during illness AND post-death',
'PHQ-9/GAD-7 for family members at risk of complicated grief',
'Structured bereavement follow-up at 1, 3, 6, and 13 months',
'Identifies need for specialist psychiatric referral for complicated grief disorder']),
]
for phase_title, bg_colour, items in prom_phases:
phase_rows = [[Paragraph(phase_title, ParagraphStyle('ph', fontName='Helvetica-Bold', fontSize=9.5, textColor=DARK, leading=13))]]
for item in items:
phase_rows.append([Paragraph(f'• {item}', ParagraphStyle('pi', fontName='Helvetica', fontSize=9, textColor=DARK, leading=12, leftIndent=12))])
pt = Table(phase_rows, colWidths=[16*cm])
pt.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), bg_colour if bg_colour != LIGHT_GREY else TEAL),
('TEXTCOLOR', (0,0), (-1,0), DARK if bg_colour != TEAL else WHITE),
('TEXTCOLOR', (0,0), (-1,0), WHITE if bg_colour == TEAL else DARK),
('BACKGROUND', (0,1), (-1,-1), bg_colour),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 8),
('BOX', (0,0), (-1,-1), 0.5, TEAL_MID),
('INNERGRID', (0,0), (-1,-1), 0.3, TEAL_MID),
]))
story.append(pt)
story.append(sp(4))
story.append(sp(4))
story.append(p('Benefits and Limitations of PROMs in Palliative Care', 'h2'))
ben_lim = [
[cell('Benefits', bold=True), cell('Limitations', bold=True)],
[cell('Improved symptom detection — patients disclose in questionnaires what they might not mention verbally (depression, existential distress, sexual concerns)'),
cell('Cognitive impairment/delirium limits self-reporting in final weeks of life')],
[cell('Objective monitoring of whether palliative interventions are working'),
cell('Questionnaire burden in very ill patients with fatigue or dyspnoea')],
[cell('Facilitates communication — PRO data displayed in clinic creates structured opening for difficult conversations'),
cell('Response shift — patients adapt expectations downwards, altering PROM scores over time')],
[cell('Enables research and quality improvement — standardised comparison across institutions'),
cell('Cultural and literacy barriers — especially significant in Indian context (multiple languages, low literacy)')],
[cell('FDA increasingly requires PROMs as primary endpoints in palliative drug trials (regulatory role)'),
cell('Proxy respondents (family) may not accurately reflect patient experience')],
[cell('ePROMs: real-time symptom reporting between visits; triggers nurse alerts for deteriorating symptoms (PMID 38812853)'),
cell('Digital divide: older/rural patients cannot access electronic systems; EMR integration challenges')],
[cell('Empowers patients — gives patients a voice; aligns care with patient priorities'),
cell('Not all PROMs validated across cultures and translated into regional languages')],
]
t = Table(ben_lim, colWidths=[8*cm, 8.2*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), TEAL),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8.5),
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, LIGHT_GREY]),
('GRID', (0,0), (-1,-1), 0.3, TEAL_MID),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('LEFTPADDING', (0,0), (-1,-1), 5),
]))
story.append(t)
story.append(sp(8))
# ── References page ──────────────────────────────────────────────────────
story.append(PageBreak())
story.append(p('KEY REFERENCES AND EVIDENCE BASE', 'q_heading'))
story.append(sp(6))
refs = [
('Harrison\'s Principles of Internal Medicine 22E (2025, McGraw Hill)', 'End-of-Life and Palliative Care, Assessment and Care Planning, Communication Frameworks, PROM instruments'),
('Tintinalli\'s Emergency Medicine — A Comprehensive Study', 'Palliative Care in the ED; Functional Decline; Prognosis; Palliative Prognostic Score; Identifying patients for PC'),
('Rosen\'s Emergency Medicine — Concepts and Clinical Practice', 'End-of-Life Trajectories and Prognostication; Illness Trajectory Figure (Lunney/Lynn/Hogan 2002)'),
('Sleisenger & Fordtran\'s GI & Liver Disease', 'Hospice vs Palliative Care; IDT team definition; Goals of Care; Exploring Patient Goals'),
('Brenner & Rector\'s The Kidney, 2-Volume Set', 'Kidney Supportive Care; Illness trajectory in CKD; Conservative kidney management'),
('Current Surgical Therapy 14E', 'Differences between PC and hospice; Specialist PC measures; Referral criteria; Surprise question'),
('Fuster & Hurst\'s The Heart 15E', 'Palliative Care in Advanced Heart Failure; illness trajectory for organ failure'),
('Miller\'s Anesthesia 10E', 'Palliative care in ICU; interdisciplinary family meeting evidence; Pediatric palliative care'),
('PMID 37310019 (2023)', 'Yoong et al. — PPI systematic review and meta-analysis (39 studies, n=19,714). Palliat Med 2023.'),
('PMID 34515737 (2021)', 'Schenker et al. — CONNECT RCT: nurse-led primary palliative care in advanced cancer. JAMA Intern Med 2021.'),
('PMID 38824442 (2024)', 'Temel et al. — Stepped Palliative Care for Advanced Lung Cancer. JAMA 2024.'),
('PMID 40366652 (2025)', 'Chang et al. — Referral criteria for specialist palliative care in dementia. JAMA Netw Open 2025.'),
('PMID 38812853 (2024)', 'Salmani et al. — Advantages/disadvantages of ePROM systems in cancer. Digit Health 2024.'),
('PMID 33096217 (2021)', 'Yoon et al. — Accuracy of PaP score with/without clinician prediction. J Pain Symptom Manage 2021.'),
('PCNOW Fast Facts #124, #444', 'Palliative Prognostic Score (PaP) and Palliative Prognostic Index (PPI). Palliative Care Network of Wisconsin.'),
('Lunney JR, Lynn J, Hogan C. 2002', 'Profiles of older Medicare decedents — 4 illness trajectories. J Am Geriatr Soc 2002;50:1108–1112.'),
('Hui et al. Ann Palliat Med', 'Models of integration of oncology and palliative care — solo, congress, integrated, embedded models.'),
]
ref_data = [[cell('Source', bold=True), cell('Topic Covered', bold=True)]]
for source, topic in refs:
ref_data.append([cell(source), cell(topic)])
story.append(mk_table(ref_data, [7.5*cm, 8.7*cm]))
return story
# ── Build PDF ─────────────────────────────────────────────────────────────────
output_path = '/tmp/workspace/palliative-care-pdf/DNB_Palliative_Medicine_QBank.pdf'
doc = SimpleDocTemplate(
output_path,
pagesize=A4,
leftMargin=1.8*cm,
rightMargin=1.8*cm,
topMargin=2*cm,
bottomMargin=1.8*cm,
title='DNB Palliative Medicine — Comprehensive Question Bank',
author='Orris Medical AI',
subject='Palliative Medicine — Models, Trajectories, PPI, PaP, PROMs',
)
story = build_story()
doc.build(story, onFirstPage=make_page, onLaterPages=make_page)
print(f'PDF generated: {output_path}')
cd /tmp/workspace/palliative-care-pdf && python3 generate_pdf.py 2>&1
ls -lh /tmp/workspace/palliative-care-pdf/DNB_Palliative_Medicine_QBank.pdf && python3 -c " from pypdf import PdfReader r = PdfReader('/tmp/workspace/palliative-care-pdf/DNB_Palliative_Medicine_QBank.pdf') print(f'Pages: {len(r.pages)}') print(f'Title: {r.metadata.title}') "
DNB Palliative Medicine QBank
PDF Document · PDF
| Pages | Content |
|---|---|
| 1 | Cover page with topic index and sources |
| 2–3 | Q1 — Models of palliative care delivery (3-tier table + 7 setting models + summary comparison table) |
| 4–5 | Q2 — Palliative care vs hospice care (differences table + care transition flowchart + referral criteria) |
| 6–8 | Q3 — PPI scoring table + interpretation + PaP scoring table + 30-day survival groups + PPI vs PaP comparison + clinical application flowchart |
| 9–10 | Q4 — IDT team member roles table + collaboration methods + 7-step goals-of-care protocol |
| 11–14 | Q5 — All 4 illness trajectories with the Lunney/Lynn/Hogan figure, clinical examples, and PC implications for each; trajectory comparison table |
| 15–16 | Q6 — PROM instruments table + continuum of care phases + benefits vs limitations table |
| 17 | Full reference list (textbooks + 6 PubMed citations) |