Military cns tb granulomas
Reading File
Finding Sources
Finding Sources
Searching PubMed
"miliary tuberculosis" AND "CNS" AND "granuloma"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
miliary tuberculosis CNS granuloma histology brain
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of military (miliary) CNS tuberculosis and granulomas:
Miliary CNS Tuberculosis & Granulomas
Pathogenesis — How Granulomas Form
TB does not reach the CNS via direct hematogenous seeding of the meninges. Instead, the sequence is:
- Primary or post-primary pulmonary TB → bacteremia → hematogenous dissemination
- Millet seed–sized (miliary) tubercles form in the brain parenchyma and subependymal regions during this dissemination
- Tubercles enlarge and typically undergo caseous necrosis
- A subependymal or subpial tubercle ruptures → discharges bacilli and TB antigens into the subarachnoid space (SAS)
- This triggers a severe inflammatory response → thick, gelatinous basilar exudate
The propensity of a caseous lesion to cause meningitis depends on its proximity to the SAS and the rate of fibrous encapsulation. — Adams and Victor's Principles of Neurology, 12th Ed.
Gross & Microscopic Pathology
Meningoencephalitis pattern (most common):
- Small discrete white tubercles scattered over base of cerebral hemispheres and, to lesser extent, convexities
- Thick, gelatinous exudate fills the basilar cisterns — pontine and interpeduncular cisterns obliterated; extends to optic chiasm, floor of third ventricle, undersurfaces of temporal lobes, medulla
- Cranial nerves and major vessels at the base become encased
- Obliterative endarteritis with marked intimal thickening → lacunar infarction
- Ependyma and choroid plexus studded with minute glistening tubercles
- Arachnoid fibrosis develops in long-standing cases → obstructive hydrocephalus
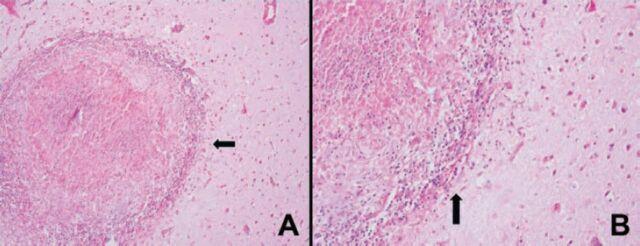
Microscopic structure of the tubercle/granuloma:
- Central zone of caseous necrosis (pale, acellular, eosinophilic on H&E)
- Surrounded by epithelioid macrophages and Langhans giant cells
- Peripheral rim of lymphocytes, plasma cells, and connective tissue
- Organisms visible on acid-fast stain but often sparse, requiring a careful search
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Adams and Victor's
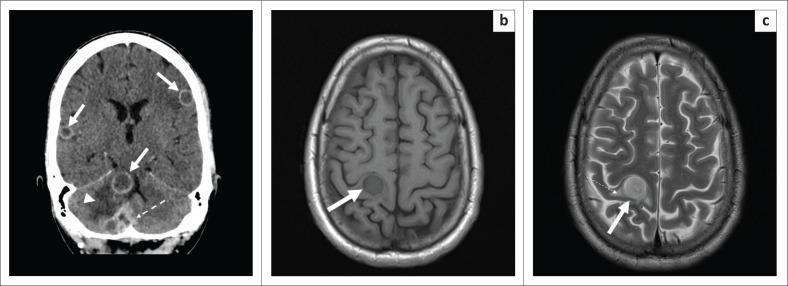
Tuberculoma (Focal Granuloma Mass)
A tuberculoma is a well-circumscribed intraparenchymal granuloma — an uncommon but important distinct form:
- May be several centimeters in diameter with significant mass effect
- Usually has central caseous necrosis; calcification in inactive/healed lesions
- Presents with seizures and focal neurological signs rather than meningitis
- On CT/MRI: contrast-enhanced ring-enhancing lesion (ring of enhancement around hypodense/hypointense center)
- Biopsy is required for definitive diagnosis
- Remains a major cause of focal CNS mass lesions in India and East Asia
— Harrison's Principles of Internal Medicine 22E; Robbins Basic Pathology
MRI Appearance of Basal Meningeal Involvement (TB Meningitis)
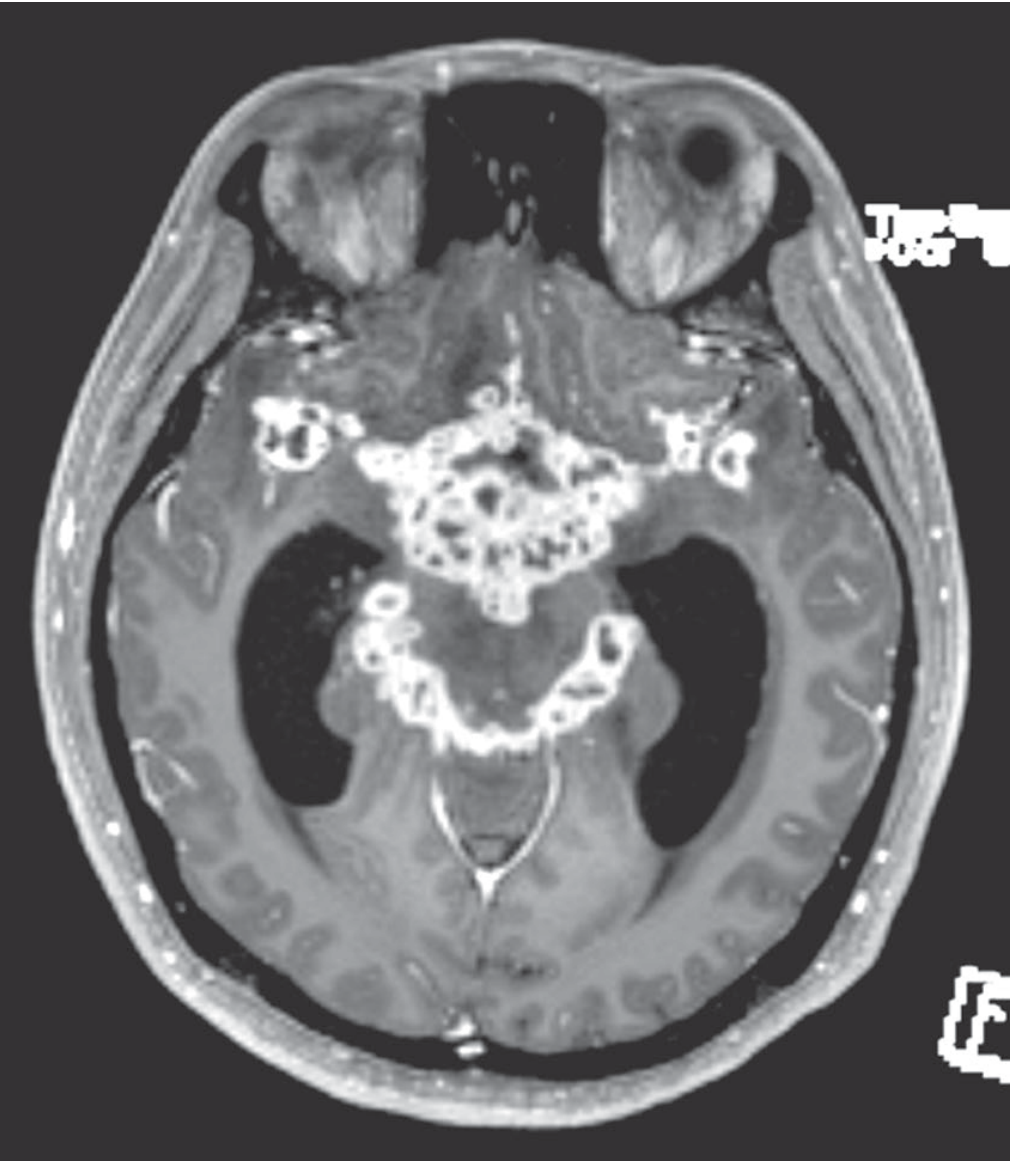
Axial T1+Gd: intense basal meningeal enhancement outlining the basilar cisterns, consistent with tuberculous meningitis with multiple small abscesses and developing hydrocephalus.
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Subacute — 1–2 weeks of prodrome (low-grade fever, malaise, headache, anorexia) |
| Meningeal signs | Headache, neck rigidity, photophobia |
| Cranial nerve palsies | Common — especially CN III, IV, VI (ocular nerves) from basal exudate |
| Focal ischemia | From obliterative endarteritis of vessels in subarachnoid space |
| Hydrocephalus | From arachnoid fibrosis and cisternal obstruction |
| Evolution | Coma, herniation if untreated — uniformly fatal if unrecognized |
| HIV co-infection | Increased incidence; less host reaction (fewer/poorly formed granulomas); higher mortality (~21%) |
CSF Findings
| Parameter | Typical Value |
|---|---|
| Opening pressure | Elevated |
| Leukocytes | 10–1000/μL; lymphocytic predominance (neutrophils early) |
| Protein | 1–8 g/L (often strikingly elevated) |
| Glucose | Low (1.1–2.2 mmol/L; 20–40 mg/dL) |
| AFB smear | Positive only 10–40% of cases |
| Culture | Gold standard; positive in up to 80% |
| Xpert MTB/RIF | Preferred initial test; sensitivity up to 80% |
A pellicle or cobweb clot on the CSF surface — smear of this clot yields the highest AFB smear positivity.
Treatment
- Four-drug regimen (HRZE) for 2 months, then HR continuation phase (total 9–12 months for CNS TB)
- Adjunctive dexamethasone (or prednisolone) tapered over 6–8 weeks:
- Reduces mortality and CSF pressure
- Does not reduce neurological sequelae
- Benefit seen in immunocompetent patients >14 years; no benefit demonstrated in PLWH in a recent RCT
- WHO now recommends glucocorticoids for all CNS TB
Response to Treatment on Imaging
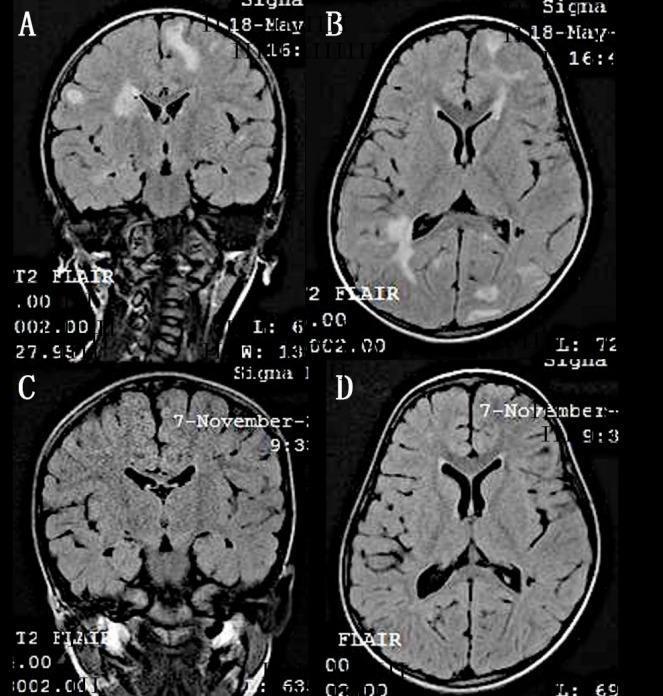
Miliary hyperintense parenchymal lesions on T2-FLAIR completely resolved after 6 months of anti-tubercular therapy.
Prognosis
- Mortality ~10% overall in immunocompetent patients; ~21% in HIV co-infected
- If diagnosis delayed until coma: mortality approaches 50%
- 20–30% of survivors have residual neurological sequelae: cognitive impairment, seizures, visual/oculomotor deficits, deafness, hemiparesis
Key distinction: Miliary CNS TB refers to hematogenous seeding producing millet seed–sized parenchymal tubercles — the precursor to tuberculous meningitis. A tuberculoma is a consolidated, enlarging granulomatous mass that behaves as a space-occupying lesion. Both involve the same granulomatous pathology (caseating necrosis + epithelioid/giant cells) but differ in location, size, and clinical presentation.
This is a shared conversation. Sign in to Orris to start your own chat.