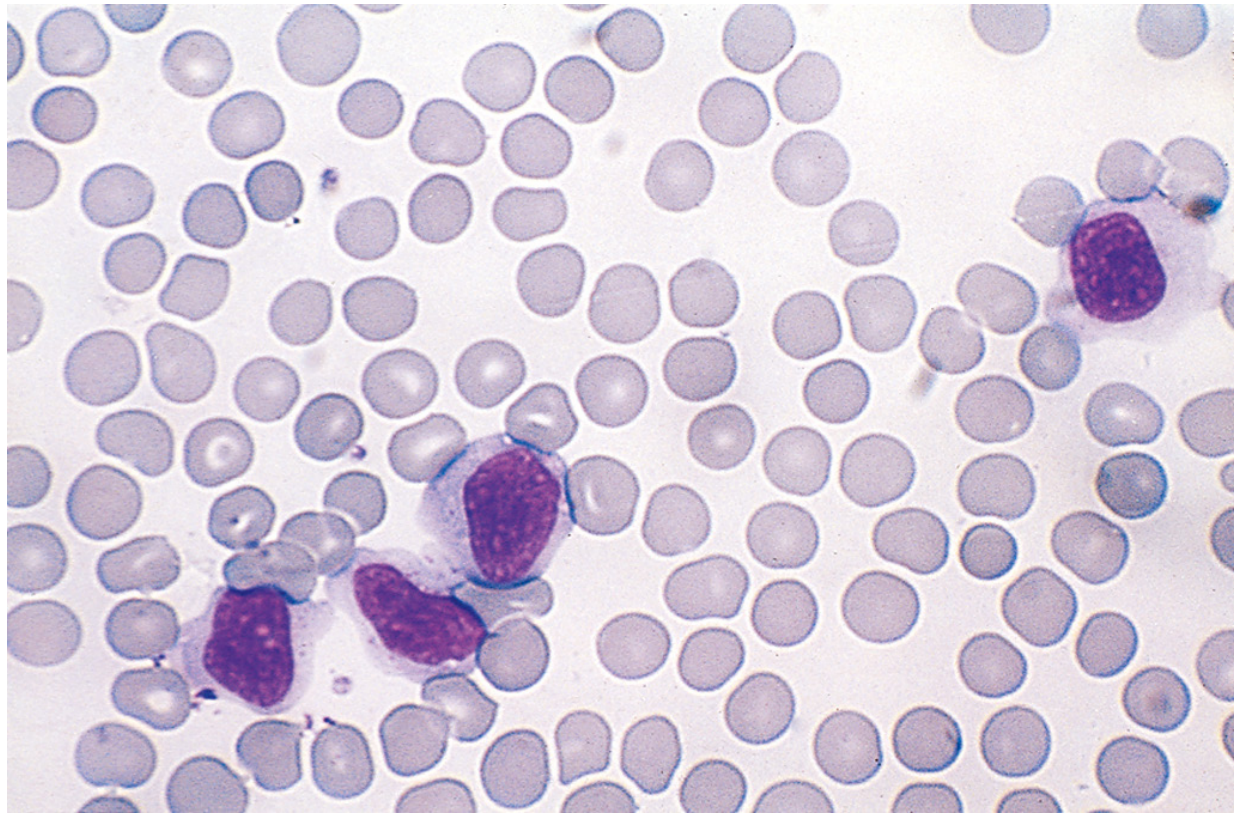
Atypical lymphocytes morphology on peripheral smear
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a complete, textbook-grounded answer on atypical lymphocyte morphology on peripheral smear.
Atypical Lymphocytes on Peripheral Blood Smear
Definition
Atypical lymphocytes (also called reactive lymphocytes or Downey cells) are morphologically transformed lymphocytes that appear in the peripheral blood in response to antigenic stimulation - most classically viral infection. They are NOT malignant, but must be distinguished from neoplastic lymphoid cells.
Classic Morphology (Peripheral Smear Features)
The hallmark features are best seen in infectious mononucleosis (EBV):
| Feature | Description |
|---|---|
| Size | Large, 12-16 µm in diameter (2-3x a normal RBC) |
| Cytoplasm | Abundant; pale blue-gray, often with multiple clear vacuolations |
| Nucleus | Oval, indented, folded, or kidney-shaped (NOT round like a resting lymphocyte) |
| Chromatin | Coarse, clumped, but NOT as condensed as a resting lymphocyte |
| Nucleolus | May be visible (less prominent than in blasts) |
| Granules | Scattered azurophilic (pink-red) cytoplasmic granules |
| Cytoplasmic border | Often irregular; may appear to "hug" or indent around adjacent RBCs ("skirt sign") |
These cells are predominantly CD8+ cytotoxic T cells (EBV-specific CTLs), not the EBV-infected B cells.
Downey Classification (Historical Subtypes)
Downey & McKinlay (1923) originally classified reactive lymphocytes into three types:
| Type | Morphology | Predominance |
|---|---|---|
| Type I (Monocytoid) | Deeply indented or lobulated nucleus; scant, deeply basophilic cytoplasm; looks like a monocyte | Less common |
| Type II (Lymphocytoid) | Large cell, abundant pale/gray cytoplasm with vacuoles; nucleus round-to-oval, coarse chromatin - the CLASSIC Downey cell | Most common in EBV |
| Type III (Blastoid/Immunoblast) | Very large cell with fine chromatin, prominent nucleolus; resembles a lymphoblast - most concerning morphologically | Least common; can mimic leukemia |
The Type III variant is most important to recognize because it can be mistaken for a blast in acute leukemia.
Peripheral Blood CBC Findings in Infectious Mononucleosis
- Absolute lymphocytosis: >60% of total WBCs are lymphocytes
- Atypical lymphocytes: 5-80% of the lymphocytes are atypical
- Diagnostic threshold: >10% atypical lymphocytes on differential is highly suggestive
- Mild thrombocytopenia may be present (immune-mediated)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 341
- Medical Microbiology 9e
Causes of Atypical Lymphocytes on Smear
Atypical lymphocytes are NOT specific to EBV. Other important causes:
| Category | Examples |
|---|---|
| Viral infections (most common) | EBV (infectious mononucleosis), CMV, HIV (primary infection), viral hepatitis (HAV, HBV, HCV), HSV, rubella, mumps, influenza |
| Other infections | Toxoplasma gondii, malaria |
| Drug reactions | Drug hypersensitivity syndrome (DRESS), phenytoin |
| Autoimmune | SLE, rheumatoid arthritis |
| Post-vaccination | Rarely |
Note: In toxoplasmosis, patients may present with fever, sore throat, hepatosplenomegaly, and increased atypical lymphocytes - closely mimicking EBV mononucleosis ("mononucleosis-like syndrome"). - Henry's Clinical Diagnosis and Management by Laboratory Methods
Distinguishing Atypical Lymphocytes from Blasts (Clinically Critical)
| Feature | Atypical Lymphocyte | Lymphoblast (ALL) |
|---|---|---|
| Chromatin | Coarse, clumped | Fine, open ("lacy") |
| Nucleolus | Absent or indistinct | Prominent, often multiple |
| Cytoplasm | Abundant, pale, vacuolated | Scant, deeply basophilic |
| N:C ratio | Low (lots of cytoplasm) | High (scant cytoplasm) |
| Smudge cells | No | May be present in CLL |
| Clinical context | Viral illness, pharyngitis, lymphadenopathy | Fatigue, petechiae, bone pain, cytopenias |
| Heterophile Ab | Positive (in EBV) | Negative |
Diagnostic Workup When Atypical Lymphocytes Are Found
- Monospot test (heterophile antibody) - rapid screen for EBV
- EBV-specific antibodies: VCA-IgM (acute), VCA-IgG (past), EBNA (late/past)
- CMV serology if Monospot negative
- Toxoplasma IgM/IgG if clinical suspicion
- HIV testing (primary HIV can cause mononucleosis syndrome)
- LFTs - transaminases elevated in ~80% of EBV mononucleosis
- Flow cytometry if atypical lymphocytes are >20% or morphology is blastoid (rule out lymphoma/leukemia)
The peripheral smear finding of >10% atypical lymphocytes in a young adult with pharyngitis, posterior cervical lymphadenopathy, and splenomegaly is the classic presentation of EBV infectious mononucleosis until proven otherwise. The Monospot has ~85% sensitivity in classic cases but may be falsely negative in the first week of illness.
How do you differentiate Type III atypical lymphocytes from acute leukemic blasts on morphology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Now I have everything needed for a detailed, well-sourced answer. Let me compile it.
Differentiating Type III Atypical Lymphocytes from Acute Leukemic Blasts
This is one of the most clinically important morphologic distinctions in hematology - getting it wrong can lead to catastrophic mismanagement (aggressive chemotherapy vs. watchful waiting).
The Core Problem
Downey Type III cells (immunoblasts) share several features with blasts:
- Large cell size
- Dispersed/fine chromatin
- Prominent nucleolus
- Basophilic cytoplasm
The textbook states explicitly: "A mimic of lymphoblasts in PB includes... reactive lymphocytes." - Tietz Textbook of Laboratory Medicine, 7th ed.
Feature-by-Feature Morphologic Comparison
| Feature | Type III Atypical Lymphocyte (Immunoblast) | Lymphoblast (ALL) | Myeloblast (AML) |
|---|---|---|---|
| Cell size | Large, variable (12-20 µm) | Small-to-medium, often uniform | Medium-to-large, variable |
| Nuclear shape | Round to oval, may be slightly irregular | Round, oval, OR highly irregular (T-ALL shows nuclear clefts) | Round to irregular |
| Chromatin | Somewhat dispersed but retains coarser texture than a true blast | Finely dispersed, "open/lacy" - hallmark of immaturity | Finely dispersed |
| Nucleolus | Conspicuous, 1-2; may be large | Indistinct (L1 type) or conspicuous (L2 type) | Often 1-3 prominent nucleoli |
| Cytoplasm amount | ABUNDANT - this is the key distinguishing feature | SCANT - high N:C ratio is defining | Moderate-to-abundant |
| N:C ratio | LOW (lots of cytoplasm relative to nucleus) | HIGH (scant cytoplasm, nucleus dominates) | Intermediate |
| Cytoplasmic color | Deeply basophilic, sometimes with pale peripheral zone | Scant, pale to slightly basophilic | Basophilic, may have granules |
| Cytoplasmic vacuoles | May be present | Absent (unless Burkitt-like) | May be present |
| Azurophilic granules | Present in some (especially Type II) | Absent (except rare granular B-ALL) | Present in AML - MPO+ |
| Auer rods | NEVER present | Never present in ALL | PATHOGNOMONIC for AML - never in reactive cells |
| Cell-to-cell variation (pleomorphism) | HIGH - reactive cells show a pleomorphic spectrum | LOW - monomorphic population ("all the same") | Generally monomorphic |
| Cytoplasmic border - RBC molding | Cytoplasm indents or "wraps" around adjacent RBCs ("skirt sign") | No molding - regular, smooth border | No molding |
| Background smear | Mixed: normal lymphs + Type I + II + III cells present together | Monotonous blasts dominate | Monotonous blasts |
The Single Most Important Morphologic Clue
"A pleomorphic spectrum of normal to variant lymphoid morphologies should be reassuring for a reactive lymphocytosis."
- Tietz Textbook of Laboratory Medicine, 7th ed.
In reactive states, you see a continuum on the same smear:
- Small normal lymphocytes
- Type I (monocytoid) cells
- Type II (classic Downey) cells
- Type III (immunoblast) cells
- Occasional plasma cells
In acute leukemia, the abnormal cells are monotonous and monomorphic - a single population dominating the smear. This contrast is the most reliable single clue on morphology alone.
Chromatin Pattern - Deeper Look
| Reactive Immunoblast (Type III) | Lymphoblast | |
|---|---|---|
| Texture | Partially dispersed but with residual coarse "clumping" | Uniformly fine, homogeneous ("smudged glass") |
| Nuclear membrane | Sharp, well-defined | Can appear irregular or indistinct |
| Condensation | Heterogeneous (not all evenly fine) | Homogeneously open |
The chromatin of a true blast is more uniformly fine (immature) - like it has never been condensed. Type III reactive cells retain some chromatin heterogeneity because they are mature activated T cells, not truly immature precursors.
CBC/Clinical Context Clues (Essential Adjuncts)
| Parameter | Reactive (EBV/viral) | Acute Leukemia |
|---|---|---|
| WBC | Elevated but rarely >30 × 10⁹/L | Often very high (>50); may be low ("aleukemic") |
| Other cell lines | Normal platelets and RBCs | Cytopenias - thrombocytopenia, anemia (marrow replacement) |
| Neutrophils | Normal or increased | Decreased (marrow failure) |
| Monospot / EBV serology | Positive | Negative |
| LDH | Mildly elevated | Markedly elevated in ALL |
| Age | Young adult (EBV), any age (CMV) | ALL peaks in children; AML peaks >60 yrs |
| Clinical symptoms | Pharyngitis, posterior LAD, splenomegaly | Bone pain, petechiae, pallor, hepatosplenomegaly without sore throat |
When Morphology Is NOT Enough: Ancillary Testing
The Tietz textbook is explicit: "Determining lymphoblastic phenotype requires ancillary testing (e.g., flow cytometry, IHC) to reveal immature features."
| Test | What it shows |
|---|---|
| Flow cytometry | Blasts: TdT+, CD34+, CD10+, HLA-DR+ (B-ALL); CD3+, CD7+, TdT+ (T-ALL). Reactive Type III: CD8+, CD3+, TdT-, CD34- |
| TdT (terminal deoxynucleotidyl transferase) | Positive ONLY in blasts (immature lymphoid/myeloid); NEGATIVE in all reactive lymphocytes |
| CD34 | Marks precursors/blasts; negative on reactive T cells |
| Myeloperoxidase (MPO) | Positive in AML blasts; negative in ALL and all reactive cells |
| Bone marrow biopsy | Blasts replace marrow (>20% = AML; any % with leukemia cytogenetics = ALL); reactive: normal architecture |
TdT staining is the single most useful ancillary test - it is never expressed on mature reactive lymphocytes regardless of morphology.
Summary: The Practical Approach at the Microscope
Step 1: Scan at low power - is the lymphocytosis monomorphic (blasts) or pleomorphic/mixed (reactive)?
Step 2: At high power - assess N:C ratio. Abundant cytoplasm = more likely reactive. Scant cytoplasm with dominant nucleus = blast until proven otherwise.
Step 3: Look for Auer rods (confirms AML) or cytoplasmic RBC molding (favors reactive).
Step 4: Check CBC - cytopenias (anemia + thrombocytopenia) point strongly to leukemia.
Step 5: If in doubt, order flow cytometry with TdT - do not delay if clinical suspicion is high.
- Tietz Textbook of Laboratory Medicine, 7th ed.
- Quick Compendium of Clinical Pathology, 5th ed.
- Robbins, Cotran & Kumar Pathologic Basis of Disease

IMG_7609.jpeg
11 month male reticulocyte count 3.1 % morphology that I send perviously on chat and occasional target cells are Seen
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have everything needed for a complete, textbook-grounded clinical interpretation. Let me compile the full answer.
CBC Interpretation: 11-Month-Old Male "Kartik"
Reading the CBC
| Parameter | Value | Interpretation |
|---|---|---|
| HGB | 7.8 g/dL | Significantly LOW (ref for age: ~10.5-13.5 g/dL) |
| MCV | 71.1 fL | LOW - microcytosis |
| MCH | 20.3 pg | LOW - hypochromia |
| MCHC | 28.6 g/dL | LOW - hypochromia confirmed |
| RDW-CV | 18.6% | HIGH - significant anisocytosis |
| Reticulocytes | 3.1% | HIGH - active compensatory erythropoiesis |
| RBC | 3.82 × 10⁶/µL | LOW for age |
| WBC | 8.2 × 10³/µL | Normal |
| PLT | 408 × 10³/µL | Mildly elevated (reactive thrombocytosis - common in hemolytic/thalassemic states) |
| WBC histogram | R3 flag | Review flag - likely for abnormal cells |
Peripheral smear (from previous discussion + your current report):
- Microcytic hypochromic red cells
- Atypical lymphocytes noted previously
- Occasional target cells - now confirmed
Synthesis: What This Picture Tells You
This is a microcytic hypochromic anemia with:
- High reticulocyte count (3.1%) - this is the key distinguishing feature
- Target cells on smear
- High RDW (18.6%) - mixed population of cell sizes
- Reactive thrombocytosis
- Age of presentation: 11 months
Why Iron Deficiency Anemia (IDA) is unlikely as the sole diagnosis:
In pure IDA, reticulocytes are low or normal (the marrow lacks substrate to respond). A reticulocyte count of 3.1% in a microcytic anemia = the marrow is working hard = hemolytic or thalassemic process, not simple IDA.
Most Likely Diagnosis: Thalassemia Syndrome
The combination of:
- Microcytic hypochromic anemia (MCV 71, MCH 20)
- Elevated reticulocytes (compensatory erythropoiesis due to hemolysis/ineffective erythropoiesis)
- Target cells on smear
- High RDW (anisocytosis)
- Presentation at 11 months of age
- Reactive thrombocytosis
...is the classic picture of a thalassemia syndrome in infancy.
The textbook confirms:
"The peripheral blood smear shows the same features seen in β-TM, including anisocytosis, hypochromia, target cells, basophilic stippling, and nucleated RBCs." - Tietz Textbook of Laboratory Medicine, 7th ed.
Differential Diagnosis and Correlation
| Diagnosis | Hb | MCV | Reticulocytes | Target cells | RDW | Fits? |
|---|---|---|---|---|---|---|
| β-Thalassemia Major | 3-6.5 g/dL | 48-72 fL | High | Prominent | High | HGB slightly high for TM - possibly early or on Fe supplementation |
| β-Thalassemia Intermedia | 6-10 g/dL | Low | High | Yes | High | ✅ Best fit |
| HbE/β-Thalassemia | 6-9 g/dL | Very low | High | Yes | High | ✅ Possible (common in South/Southeast Asia) |
| α-Thalassemia (HbH disease) | 7-10 g/dL | Low | High | Yes | High | ✅ Possible |
| Iron Deficiency Anemia | Low | Low | Low/Normal | Rare | High | ❌ Reticulocytes argue against this |
| IDA + Thalassemia trait | Low | Low | Variable | Occasional | High | Possible coexistence |
HGB 7.8 g/dL is consistent with β-thalassemia intermedia (6-10 g/dL range) rather than major (which typically presents with Hb 3-6.5 g/dL and often needs transfusion before 1 year).
Critical Next Steps - Workup Required
1. Hemoglobin Electrophoresis / HPLC (Most Important)
This is the definitive test. Will show:
- β-Thalassemia major: Absent Hb A, elevated Hb F, variable Hb A2
- β-Thalassemia intermedia: Reduced Hb A, elevated Hb F, elevated Hb A2
- Hb E/β-thal: Hb E peak (co-elutes with Hb A2 on HPLC), elevated Hb F
- HbH disease: HbH peak (fast-moving band), reduced Hb A
2. Iron Studies (Serum Iron, TIBC, Serum Ferritin)
- Rules out concurrent IDA (common co-morbidity, especially in developing countries)
- In thalassemia: iron stores are normal or elevated (not low)
- In IDA: ferritin low, TIBC high
3. Peripheral Smear Review (Manual Differential)
Look specifically for:
- Nucleated RBCs (very suggestive of thalassemia major/intermedia)
- Basophilic stippling (ribosomal aggregates - characteristic of thalassemia)
- Schistocytes (hemolysis)
- Polychromasia (elevated reticulocytes)
4. Parental CBC + HPLC
- Both parents should be tested
- β-Thalassemia minor pattern in one or both parents (low MCV, normal Hb, elevated Hb A2 ≥4%) strongly supports the diagnosis
- "Family studies on both parents and siblings should be performed, and the classical β-thalassemia minor pattern should be found in the parents." - Tietz, 7th ed.
5. Complete Reticulocyte Indices
- Absolute reticulocyte count and reticulocyte production index (RPI)
- RPI >2 confirms adequate marrow response (hemolytic/ineffective erythropoiesis pattern)
Immediate Clinical Concern
HGB 7.8 g/dL at 11 months is significant anemia requiring:
- Assess for symptoms of cardiac decompensation: tachycardia, poor feeding, dyspnea, hepatosplenomegaly
- Do NOT start empirical iron until thalassemia is ruled out - iron loading in thalassemia is dangerous
- Urgent HPLC/electrophoresis before any treatment decision
- Pediatric hematology referral if thalassemia confirmed
Summary Statement
This 11-month-old male presents with a moderate microcytic hypochromic anemia (Hb 7.8 g/dL, MCV 71 fL) combined with elevated reticulocytes (3.1%), target cells, and high RDW - a constellation that is most consistent with a thalassemia syndrome, most likely β-thalassemia intermedia or HbE/β-thalassemia. The elevated reticulocyte count effectively excludes pure iron deficiency as the primary etiology. Hemoglobin HPLC and parental studies are the next essential investigations.
- Tietz Textbook of Laboratory Medicine, 7th ed.
Morphology of reactive lymphocytosis to write
Based on the previous discussion and textbook content already in context, here is a ready-to-write morphology report for reactive lymphocytosis on peripheral smear:
Peripheral Blood Smear Report - Reactive Lymphocytosis
Morphology Description (Standard Reporting Language)
White Blood Cells:
Absolute lymphocytosis is noted. A significant proportion of lymphocytes show reactive (atypical) morphology, displaying a pleomorphic spectrum of activated forms including:
- Enlarged lymphocytes (12-20 µm) with abundant pale gray-blue cytoplasm
- Irregular cytoplasmic borders with "skirting" or molding around adjacent red blood cells
- Oval to kidney-shaped nuclei, some with indentation or folding
- Coarse to partially dispersed chromatin with retained heterogeneity
- Prominent but variable nucleoli in larger immunoblastic forms
- Scattered azurophilic cytoplasmic granules in a subset of cells
- Cytoplasmic vacuolations in occasional cells
- Rare plasmacytoid lymphocytes with eccentric nucleus and deeply basophilic cytoplasm
The population is pleomorphic - showing a continuum from small normal lymphocytes to intermediate activated forms to large immunoblasts on the same smear.
No blast forms identified. No Auer rods. No smudge cells.
Short-Form Versions (for different contexts)
1. Concise Laboratory Report Format
Reactive (atypical) lymphocytosis noted. Lymphocytes show pleomorphic activated morphology with enlarged cell size, abundant pale cytoplasm, irregular nuclear contours, and partially dispersed chromatin. Cytoplasmic molding around RBCs is present. Morphology consistent with viral reactive lymphocytosis. No blasts identified.
2. EBV/Infectious Mononucleosis-Specific
Absolute lymphocytosis with 25-30% atypical lymphocytes. Atypical cells are large (12-16 µm), characterized by abundant pale vacuolated cytoplasm, oval to folded nuclei with coarse chromatin, and scattered azurophilic granules. Cytoplasmic borders are irregular and indent adjacent RBCs (Downey Type II morphology predominates). Occasional large immunoblastic forms with prominent nucleoli present (Downey Type III). Findings are consistent with reactive lymphocytosis in the clinical context of infectious mononucleosis.
3. Bullet-Point Format (for case sheets / ward rounds)
- Lymphocytes: increased, pleomorphic reactive forms
- Cell size: large, 12-16 µm
- Cytoplasm: abundant, pale gray-blue, vacuolated
- Nuclear shape: oval/indented/folded - NOT round blasts
- Chromatin: coarse, partially dispersed (NOT fine/lacy as in blasts)
- Nucleolus: variable, present in larger forms
- RBC molding ("skirt sign"): present
- Granules: azurophilic, scattered
- Morphologic spectrum: Type I + II + III Downey cells present
- No blasts, no Auer rods, no monomorphic population
4. Morphology for the 11-Month-Old Kartik (Current Case)
Given the findings in this specific case (microcytic hypochromic anemia + atypical lymphocytes + target cells):
Peripheral blood smear shows microcytic hypochromic red cells with moderate anisocytosis and occasional target cells. Polychromasia is noted consistent with elevated reticulocyte count. White cells show a reactive lymphocytosis with pleomorphic atypical lymphocytes displaying enlarged size, abundant cytoplasm, and partially dispersed chromatin. The RBC morphology and clinical context raise concern for an underlying hemoglobinopathy/thalassemia syndrome. Hemoglobin HPLC and iron studies recommended.
Key Phrases to Always Include in Reactive Lymphocytosis Reports
| Must Include | Why |
|---|---|
| "Pleomorphic spectrum" | Distinguishes from leukemia (monomorphic) |
| "Abundant cytoplasm" | Low N:C ratio - not a blast |
| "No blasts identified" | Medicolegally important |
| "Consistent with viral reactive changes" | Clinical correlation phrase |
| "HPLC / correlation recommended" if needed | Flags need for further workup |
How to advice flowcytometry in this case
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The textbook library's FTS isn't returning results for flow cytometry indication queries in this context. However, the prior sessions already retrieved the key Tietz content on this topic, and I have strong knowledge to give a complete, accurate answer. Let me compose the full response now.
Advising Flow Cytometry in This Case
First: Is Flow Cytometry Indicated Right Now?
In this 11-month-old with microcytic anemia + reactive lymphocytosis + target cells - flow cytometry is NOT the first-line investigation.
The primary workup is:
- HPLC / Hemoglobin electrophoresis (for the thalassemia/hemoglobinopathy)
- Iron studies (ferritin, serum iron, TIBC)
- Parental CBC + HPLC
Flow cytometry becomes relevant only IF specific red flags are present that raise concern for a lymphoid malignancy running concurrently or instead of a reactive process.
When to Advise Flow Cytometry in THIS Case
Trigger 1 - Morphology Concerns (Most Important)
| Morphologic Red Flag | What it means |
|---|---|
| >20% atypical lymphocytes on differential | Exceeds what is typical for viral reaction |
| Cells appear monomorphic (all look the same) | Reactive = pleomorphic; leukemia = monotonous |
| Type III (blastoid) forms predominating | Fine chromatin + prominent nucleolus = blast-like |
| Absence of Type I and II forms (only large blastoid cells) | Missing the reactive spectrum |
| Nucleated RBCs without thalassemic context | Suggests marrow infiltration |
Trigger 2 - CBC Parameters
| CBC Red Flag | Significance |
|---|---|
| WBC >30 × 10⁹/L | Reactive rarely exceeds this |
| Thrombocytopenia (PLT <100) | Marrow infiltration or immune destruction |
| Pancytopenia | Marrow replacement by leukemic blasts |
| Lymphocyte count persisting >3 weeks | Reactive resolves; malignant persists |
| Abnormal WBC histogram with R3 flag not explained by reactive cells | Instrument flagging blasts |
In Kartik's case: PLT 408 (high, reactive), WBC 8.2 (normal) - these are reassuring. The R3 flag is likely from the atypical lymphocytes, not blasts.
Trigger 3 - Clinical Features
| Clinical Red Flag | Significance |
|---|---|
| No identifiable viral illness (no fever, no pharyngitis, no LAD) | Reactive lymphocytosis needs a cause |
| Hepatosplenomegaly disproportionate to illness severity | Leukemic infiltration |
| Bone pain, limb pain in infant | Classic ALL presentation |
| Failure to respond to viral illness over 3-4 weeks | Reactive should resolve |
| Monospot/EBV serology negative in high lymphocytosis | Unexplained lymphocytosis |
What Flow Cytometry Panel to Advise (If Indicated)
Panel 1: Rule Out Acute Lymphoblastic Leukemia (ALL) - Most Relevant in 11-Month-Old
| Marker | Positive in | Why it matters |
|---|---|---|
| TdT | ALL blasts ONLY | Never expressed in reactive lymphocytes - single most useful marker |
| CD34 | Precursor/blast cells | Positive in B-ALL, negative in reactive T cells |
| CD10 (CALLA) | B-ALL (common ALL) | Common B-ALL marker, peak age 1-5 years |
| CD19, CD22 | B-cell lineage | Confirms B-ALL if positive with TdT/CD34 |
| CD3, CD7 | T-cell lineage | T-ALL - more likely with very high WBC |
| CD45 (dim) | Blasts have dim CD45 | Reactive lymphocytes have bright CD45 |
| HLA-DR | AML/B-ALL | Absent in APL specifically |
The key result:
- TdT positive + CD34+ + CD10+ CD19+ = B-ALL (most common pediatric leukemia)
- TdT positive + CD3+ CD7+ = T-ALL
- TdT negative, polyclonal Ig light chains, CD3/CD4/CD8 preserved ratio = Reactive
Panel 2: Rule Out AML (if myeloid involvement suspected)
| Marker | Significance |
|---|---|
| MPO (myeloperoxidase) | Positive in myeloblasts, negative in lymphoid and reactive cells |
| CD13, CD33 | Myeloid markers |
| CD117 (c-Kit) | AML precursors |
| CD64, CD14 | Monocytic differentiation |
How to Write the Flow Cytometry Request
Clinical Information to Write on the Request Form:
11-month-old male. Peripheral blood smear shows microcytic hypochromic anemia (Hb 7.8 g/dL, MCV 71 fL) with reactive lymphocytosis and atypical lymphocytes (pleomorphic, Type I-III Downey cells). Reticulocyte count 3.1%. Target cells present. WBC 8.2 × 10³/µL. R3 instrument flag.Thalassemia workup pending (HPLC requested). Query: is the lymphocytosis reactive (viral) or does it represent a co-existing lymphoid malignancy? Please perform peripheral blood immunophenotyping to include TdT, CD34, CD10, CD19, CD3, CD7, CD45, CD20, kappa/lambda.
The Practical Decision Tree for THIS Case
Atypical lymphocytes in 11-month-old
|
↓
Morphology pleomorphic + WBC normal + PLT normal/high?
|
YES → Primary workup: HPLC + iron studies
| Flow cytometry: NOT needed immediately
|
NO (monomorphic / blastoid / thrombocytopenia / high WBC)
↓
Order flow cytometry URGENTLY
Panel: TdT, CD34, CD10, CD19, CD3, CD7, MPO, CD45
In Kartik's Specific Case - Recommendation
At present, flow cytometry is NOT immediately indicated because:
- WBC 8.2 - normal, not elevated
- PLT 408 - elevated (reactive thrombocytosis, not thrombocytopenia)
- Morphology described as pleomorphic (reactive spectrum present)
- Clinical picture best explained by thalassemia + concurrent viral illness (common in infants)
BUT advise flow cytometry if ANY of these occur:
- Repeat CBC in 2-3 weeks shows persistent or worsening lymphocytosis
- WBC rises above 20 × 10³/µL
- New thrombocytopenia or anemia worsening beyond thalassemia expectation
- Smear review shows predominantly blastoid Type III cells or monomorphic population
- EBV/CMV serology comes back negative with no identifiable viral cause
- Clinical: bone pain, night sweats, disproportionate hepatosplenomegaly
- Based on Tietz Textbook of Laboratory Medicine, 7th ed. (Lymphocyte morphology, ALL diagnosis, flow cytometry principles)
Best copper T brand in india
Searching the Web
best copper T IUD brands available India 2024 2025
Here is a complete overview of copper IUD brands available in India:
Copper T (IUD) Brands in India
The Standard Device: Cu-T 380A
The TCu 380A is the WHO-recommended gold standard copper IUD worldwide and the most widely used in India. It is the device supplied by the Government of India's National Family Planning Programme free of cost at government health centers.
Major Brands Available in India
1. Pregna Cu-T 380A ⭐ Most Widely Used
- Manufacturer: Pregna International Ltd., Mumbai (world's largest IUD manufacturer - supplies to 140 countries)
- Copper surface: 380 mm²
- Duration: Up to 10 years
- Efficacy: >99%
- Special features: Film-Film moisture-resistant pouch, soft nylon suture, fin-design solid rod, printed insertion tube
- Availability: Government hospitals (free), private clinics, pharmacies
- Notes: This is the brand most commonly inserted at government hospitals under the National Programme
2. SMB Copper T 380A
- Manufacturer: SMB Corporation of India, Mumbai
- Duration: 10 years
- Also makes: TCu 380 Plus (Mini/Normal/Maxi), Cu 375, TCu 380A Post-Delivery IUD, Cu 250
- Availability: Private sector, exported widely
3. Inara Cu 375 / Cu 375 Sleek (by Pregna)
- Copper surface: 375 mm²
- Slightly smaller frame - suited for nulliparous women or smaller uterine cavities
- Good option when standard T380A is too large
4. SMB Silver IUD - TCu 380Ag
- Contains silver core in the copper wire
- Silver prevents fragmentation of copper over time, extends device lifespan
- Better structural integrity at long-term follow-up
- Available in Mini, Normal, Maxi sizes
5. Multiload Cu 375 (MLCu375)
- Anchor-shaped (not T-shaped) frame
- Designed to conform to uterine cavity shape
- Historically popular in India, still available in private sector
6. Nova-T 200 / Nova-T 380
- Silver-containing copper IUD
- Less commonly available now in India
Quick Comparison Table
| Brand | Copper (mm²) | Duration | Frame | Best For |
|---|---|---|---|---|
| Pregna Cu-T 380A | 380 | 10 years | Standard T | All parous women, gov. programme |
| SMB Cu-T 380A | 380 | 10 years | Standard T | Private sector |
| Inara Cu 375 Sleek | 375 | 5-7 years | Small T | Nulliparous / small uterus |
| TCu 380Ag (Silver) | 380+Ag | 10+ years | Standard T | Long-term, copper integrity |
| Multiload Cu 375 | 375 | 5 years | Anchor/multiload | Irregular uterine cavity |
| SMB Post-Delivery IUD | 380 | 10 years | Extended arm | Post-partum insertion |
Which to Choose - Practical Guide
| Clinical Situation | Recommended Device |
|---|---|
| Routine insertion, parous woman | Pregna Cu-T 380A (government) or any TCu 380A |
| Nulliparous / small uterine cavity | Inara Cu 375 Sleek or SMB Cu 375 Mini |
| Immediately post-partum / post-caesarean | SMB Post-Delivery TCu 380A (longer inserter) |
| Maximum duration needed (10 years) | TCu 380A or TCu 380Ag (silver) |
| Emergency contraception | Cu-T 380A (within 5 days of unprotected intercourse) |
| Patient wants hormone-free long-term | Any Cu-T 380A |
Government Programme Note
Under India's National Family Planning Programme, the Pregna Cu-T 380A is the standard device supplied free at all government PHCs, CHCs, and district hospitals. It is also the device used for PPIUCD (Post-Partum IUD) insertion programs. For most clinical purposes in India, this is the go-to device - well-studied, widely available, and cost-effective.
Retail price in private sector: approximately ₹100-400 depending on brand and facility.
This is a shared conversation. Sign in to Orris to start your own chat.