Why do they say to reduce salt intake in hypertensive patients? What’s the physiological explanation
Reading File
Finding Sources
Searching PubMed
sodium reduction hypertension mechanism
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have very rich, authoritative content from Guyton, Brenner & Rector, and Comprehensive Clinical Nephrology. Here is the full, well-sourced answer:
Why Salt Restriction Lowers Blood Pressure: The Physiology
1. Sodium and Osmolality - The Starting Point
Sodium is the dominant extracellular cation. When you eat salt (NaCl), serum osmolality rises. The hypothalamic osmoreceptors detect this and trigger two responses simultaneously:
- ADH (vasopressin) release from the posterior pituitary - causes the kidneys to retain water
- Thirst - drives additional water intake
Both responses dilute the sodium back toward normal, but the net result is that more water is held in the circulation, expanding plasma volume and extracellular fluid (ECF).
2. Volume Expansion Raises Cardiac Output
The expanded ECF volume increases venous return to the heart (preload). By Starling's law, the heart stretches more and ejects more with each beat, raising cardiac output (CO). Since:
MAP = CO × Total Peripheral Resistance (TPR)
an acute rise in CO directly raises blood pressure.
3. The Kidney's Normal Escape Mechanism - Pressure Natriuresis
In healthy individuals, the kidney has a powerful feedback loop called pressure natriuresis/diuresis. As arterial pressure rises, the kidney excretes more sodium and water until the volume overload is corrected and blood pressure returns to near-normal. This is why normal people can eat a wide range of salt without dramatic BP changes - the kidney's renal output curve is very steep.
As Guyton explains, if the kidneys and hormonal systems are functioning normally, chronic increases in salt intake to as high as six times normal cause only small changes in arterial pressure, because the renal output curve shifts sharply upward to maintain balance. - Guyton and Hall Textbook of Medical Physiology
4. Why Hypertensive Patients Can't Escape Normally - "Salt Sensitivity"
The critical difference in hypertension is that the pressure natriuresis curve is reset or blunted. The kidney requires a higher blood pressure than normal to excrete the same sodium load. This can happen through several overlapping mechanisms:
a) Reduced functional nephron mass
Loss of nephrons (from aging, diabetes, CKD, or chronic hypertension itself) reduces the total filtration capacity. With fewer nephrons contributing, the remaining ones must operate at higher pressures to handle the same sodium load. - Guyton and Hall, Table 19.1
b) RAAS (Renin-Angiotensin-Aldosterone System) overactivation
- Angiotensin II directly constricts efferent arterioles and stimulates proximal tubule Na⁺ reabsorption via NHE3 (Na⁺/H⁺ exchanger)
- Aldosterone upregulates ENaC (epithelial sodium channels) in the distal tubule and collecting duct, further promoting Na⁺ and water retention
- When these systems fail to appropriately suppress in response to a sodium load, salt sensitivity is amplified. - Guyton and Hall
c) Sympathetic nervous system activation
Increased sympathetic tone causes renal vasoconstriction (reducing GFR and natriuresis) and directly stimulates tubular sodium reabsorption. The baroreceptor reflex normally damps this during BP rises, but with sustained hypertension the baroreflex can be reset upward, allowing SNS activity to persist even at elevated pressures.
d) Autoregulation and structural vascular changes
Over time, chronically elevated cardiac output causes autoregulatory vasoconstriction - blood vessels constrict to protect downstream tissues from excess flow. TPR rises, and now both CO and TPR are elevated, maintaining high blood pressure even if volume partly normalizes. The vascular wall also undergoes structural remodeling (hypertrophy), making this harder to reverse.
e) Genetic factors
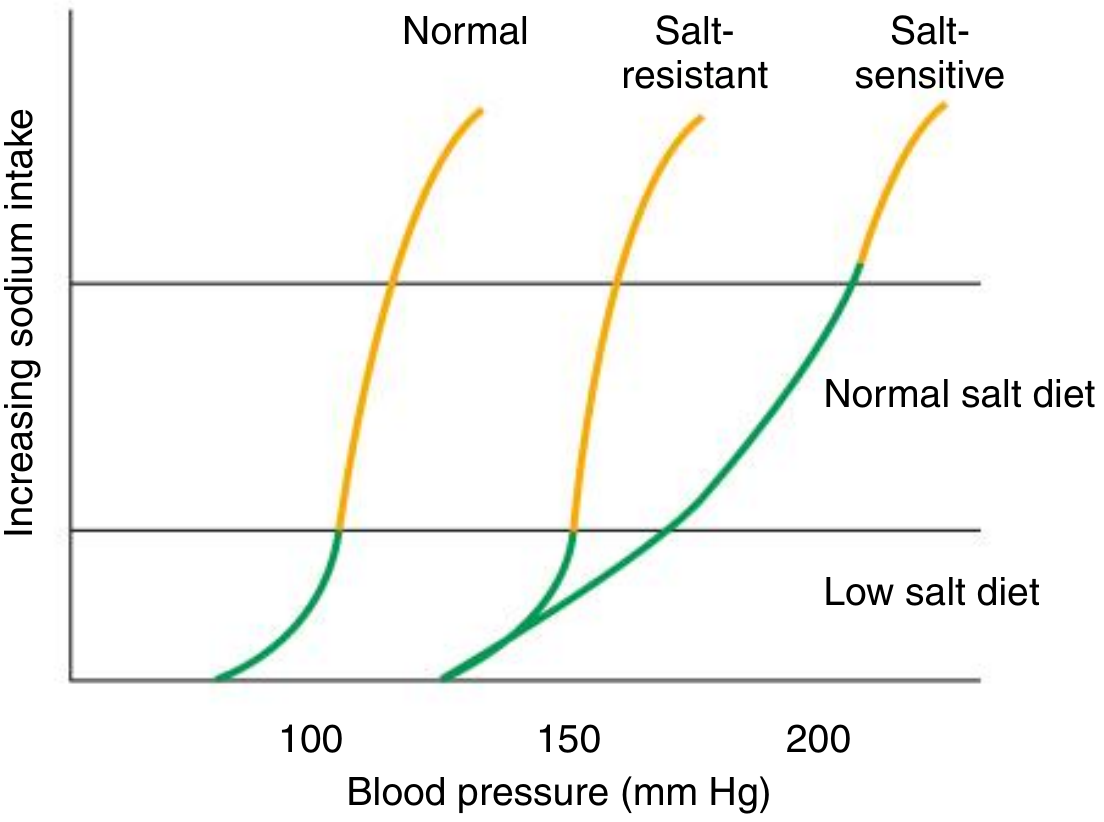
Polymorphisms in renal sodium transporters (e.g., gain-of-function mutations in ENaC causing Liddle syndrome; variants in Na-Cl cotransporter SLC12A3 or Na-K-2Cl cotransporter SLC12A1) can tip the balance toward sodium retention in hypertensive subjects. The Comprehensive Clinical Nephrology textbook notes that in salt-sensitive hypertension, increasing salt intake produces an exaggerated rightward-shifted BP response curve compared to normal subjects.
5. Why Reducing Salt Intake Helps
By cutting sodium intake, you shift the equilibrium point leftward:
| Effect of Salt Reduction | Mechanism |
|---|---|
| Plasma volume falls | Less osmotic water retention |
| Venous return decreases | Lower preload → lower CO |
| Arterial pressure drops | Direct MAP = CO × TPR effect |
| RAAS partially suppresses | Lower Ang II → less tubular Na⁺ reabsorption |
| SNS tone decreases | Baroreceptor reflex responds to lower filling pressures |
The quantitative effect is meaningful: a meta-analysis of RCTs (≥4 weeks duration) found that reducing salt by 3 g/day lowers SBP by 3.6-5.6 mmHg and DBP by 1.9-3.2 mmHg in hypertensive patients - and estimates suggest a 9 g/day reduction could cut stroke risk by ~33% and ischemic heart disease by ~25%. In the TONE trial, reducing sodium to 80 mEq/day allowed ~40% of elderly hypertensive patients to discontinue antihypertensive medications. - Brenner and Rector's The Kidney, 2-Volume Set
6. The Potassium-Sodium Interaction
Potassium competes with sodium at the aldosterone-sensitive distal nephron. Higher potassium intake suppresses aldosterone secretion and enhances natriuresis (the Na-K-ATPase pump exports Na⁺ in exchange for K⁺). This is why the DASH diet - which adds fruits, vegetables, and low-fat dairy (high K⁺, low Na⁺) - has additive BP-lowering effects beyond sodium restriction alone. Salt substitutes that replace some NaCl with KCl exploit this same mechanism. - Katzung's Basic and Clinical Pharmacology, 16th Ed.
Summary
The chain from salt to hypertension is:
High salt intake → osmolality ↑ → ADH/thirst → water retention → plasma volume ↑ → CO ↑ → BP ↑
In healthy kidneys, pressure natriuresis corrects this quickly. In hypertensive patients, the natriuresis curve is reset - the kidney needs a higher BP to excrete the same sodium load (due to nephron loss, RAAS excess, SNS activation, or genetic variants). Salt restriction reduces the sodium burden the kidney must handle, allows the system to operate at a lower equilibrium BP, and potentiates the effects of antihypertensive drugs - especially ACE inhibitors, ARBs, and diuretics - which all work partly through the same RAAS/renal axis.
Really helpful thanks
Glad it helped! Feel free to ask if you want to go deeper on any part of it - like the RAAS pathway in more detail, specific drug mechanisms that target this system, or anything else.
This is a shared conversation. Sign in to Orris to start your own chat.