Goiter
Reading File
Finding Sources
Searching PubMed
goiter thyroid management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Here is a thorough review of goiter:
Goiter
Definition
Goiter is any enlargement of the thyroid gland. In common clinical usage it refers to benign enlargement - whether diffuse or nodular - though technically any cause of thyroid enlargement (including malignancy) qualifies. The key physiologic principle is that high TSH levels (or TSH-like substances) exert a trophic/growth effect on the thyroid, which underlies goiter formation across most etiologies.
- Costanzo Physiology 7th Edition, p. 431
Classification
| Type | Features |
|---|---|
| Simple (colloid) goiter | Diffuse, euthyroid; iodine deficiency most common worldwide cause |
| Toxic diffuse goiter | Graves disease; driven by thyroid-stimulating immunoglobulins |
| Toxic multinodular goiter | Multiple autonomously functioning nodules; hyperthyroid |
| Nontoxic multinodular goiter | Nodular, euthyroid; most common in iodine-sufficient areas |
| Endemic goiter | Iodine-deficient region; may be diffuse or nodular |
| Substernal/Intrathoracic goiter | Extension below the thoracic inlet; potential airway emergency |
Epidemiology
-
The most common anatomic disease of the thyroid worldwide, with iodine deficiency as the global leading cause.
-
In iodine-sufficient countries (like the US), goiter independent of Graves disease is typically associated with Hashimoto's autoimmune thyroiditis as it progresses toward a hypothyroid state.
-
Strong genetic component when it occurs in areas of adequate iodine intake.
-
More common in women; frequency increases with age.
-
Textbook of Family Medicine 9e, p. 1024
Pathogenesis
Causes and TSH Status
| Condition | Thyroid Status | TSH | Goiter? |
|---|---|---|---|
| Graves disease | Hyperthyroid | Low (suppressed by T4/T3) | Yes - TSH-like immunoglobulins are trophic |
| TSH-secreting pituitary tumor | Hyperthyroid | High | Yes |
| Exogenous T4 ingestion (factitious) | Hyperthyroid | Low | No - gland involutes |
| Autoimmune (Hashimoto's) thyroiditis | Hypothyroid | High (by negative feedback) | Yes - even though gland is dysfunctional |
| TSH deficiency (pituitary failure) | Hypothyroid | Low | No |
| Iodine deficiency | Euthyroid or hypothyroid | High (by negative feedback) | Yes |
Key concept: Goiter can coexist with hypo-, hyper-, or euthyroid states. Its presence depends on TSH/TSH-like trophic drive, NOT on hormone output.
Nontoxic Multinodular Goiter - Specific Pathogenesis
The thyroid undergoes repeated cycles of stimulation and regression, producing:
- Solid nodules and colloid cysts
- Areas of fibrosis
- Functional heterogeneity within the gland
Contributing factors include iodine deficiency, dietary goitrogens (bamboo shoots, maize, sweet potatoes), genetic factors, and dyshormonogenesis.
- Current Surgical Therapy 14e, p. 880
Clinical Features
Symptoms
- Most goiters are asymptomatic and discovered incidentally
- Compressive symptoms arise with enlargement:
- Dyspnea / stridor - tracheal compression/deviation (crowing inspiration)
- Dysphagia - esophageal compression
- Hoarseness - direct laryngeal pressure or, less commonly, recurrent laryngeal nerve (RLN) stretch/compression (RLN palsy from a benign goiter is uncommon; malignant invasion is the more common cause)
- Neck pressure / choking sensation, especially with certain movements
- Venous congestion with certain head positions
Key Examination Signs
- Thyroid moves on swallowing - attached to the larynx via pretracheal fascia (distinguishes from other neck masses)
- Tracheal deviation - asymmetric enlargement pushes trachea contralaterally
- Pemberton's sign - raising both arms above the head produces facial plethora and redness from venous obstruction (indicates significant substernal extension)
- Nodularity, irregular ("knobby") surface in multinodular goiter
Rapid Enlargement - Red Flags
Rapid thyroid enlargement should raise suspicion for:
- Hemorrhage into a benign nodule
- Anaplastic thyroid carcinoma
- Thyroid lymphoma
Diagnosis
Workup Algorithm
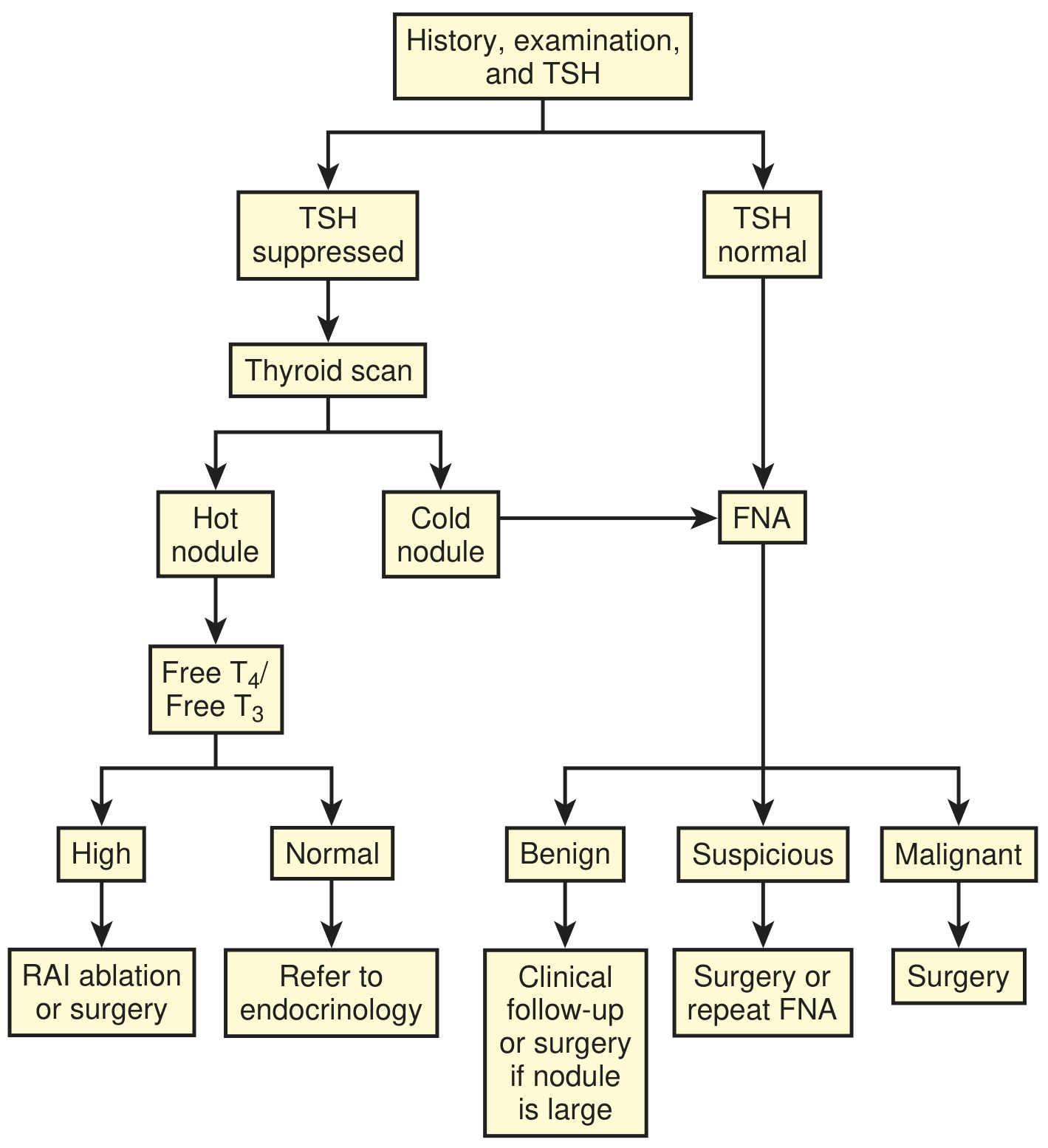
Step 1 - Thyroid function tests:
- TSH, free T4, free T3
- Identifies subclinical/overt thyrotoxicosis, hypothyroidism, or euthyroid state
Step 2 - Imaging:
- Ultrasound - first-line; evaluates nodule characteristics
- Features raising malignancy risk: hypoechogenicity, microcalcifications, hypervascularity, solid components within cystic nodules, regional lymphadenopathy
- CT (non-contrast preferred) - most sensitive for airway compromise, substernal extension, mediastinal involvement. Avoid iodinated contrast in Graves disease or toxic nodular goiter - iodine load can precipitate acute hyperthyroidism
- MRI - alternative to CT for soft-tissue detail
Step 3 - Nuclear imaging:
- Thyroid scan (radioiodine): if TSH is suppressed, to assess hot vs cold nodules. Hot (autonomous) nodules are almost never malignant.
Step 4 - FNA biopsy:
- For any suspicious nodule (cold on scan, or TSH-normal + nodule ≥1 cm, or with suspicious ultrasound features)
- Ultrasound-guided preferred
- Results: Benign, Suspicious, Malignant → guide further management
Additional tests for large goiters:
-
Pulmonary function tests / flow-volume loop - detect fixed upper airway obstruction
-
Fiber-optic laryngoscopy - mandatory if voice changes or prior neck surgery (assess vocal cord mobility)
-
Barium swallow - if dysphagia is prominent (less commonly needed in modern practice)
-
Goldman-Cecil Medicine, p. 3278; Sabiston Textbook of Surgery
Graves Disease - The Five Hallmarks
Goiter is one of the five classic hallmarks of Graves disease:
- Thyrotoxicosis
- Goiter (present in nearly 100% of patients)
- Ophthalmopathy (exophthalmos)
- Pretibial (local) myxedema
- Acropachy (clubbing of fingers and toes)
Treatment
Treatment Principles
Address the underlying cause first. Management depends on etiology (Graves vs Hashimoto's vs nontoxic multinodular) and on thyroid functional status.
Indications for Active Treatment of Nontoxic Goiter
- Local discomfort, choking, or tightness (especially with movement)
- Mechanical partial obstruction of the aerodigestive tract
- Substantial substernal extension (even without symptoms - relative indication, as future operation may be more disruptive)
- Cosmesis is rarely an isolated indication
Treatment Modalities
1. TSH-suppressive therapy (levothyroxine)
- Has little to no role in established multinodular goiter management
- Prospective trials show no benefit
- Side effects (bone loss, atrial arrhythmias) particularly significant in elderly patients
2. Radioiodine (RAI) ablation
- Can reduce goiter size by 40-60% within 2 years
- Decreases compressive symptoms
- Complications: radiation thyroiditis, hypothyroidism, transient gland enlargement (potentially dangerous in large goiters with airway compromise)
- Can be combined with exogenous TSH (recombinant TSH) to boost radioiodine uptake in goiters with limited iodine uptake
- Useful in patients with comorbidities who are poor surgical candidates
3. Surgery (thyroidectomy)
- Definitive treatment for large or symptomatic goiters
- Options: total thyroidectomy or subtotal thyroidectomy
- Substernal goiter may require manubriotomy/median sternotomy for mediastinal component
- Preoperative vocal cord assessment mandatory (fiber-optic laryngoscopy if any voice changes or prior neck surgery)
Complications of thyroidectomy:
-
Hypoparathyroidism / hypocalcemia - from trauma or inadvertent removal of parathyroid glands; manifests as tingling in hands, feet, and perioral region, carpopedal spasm, and tetany
-
RLN injury - hoarseness, voice change
-
Hypothyroidism (requiring lifelong levothyroxine)
-
Current Surgical Therapy 14e, p. 880-881; Goldman-Cecil Medicine
Special Situations
Endemic Goiter
Caused by iodine deficiency in certain geographic regions. Public health iodination of salt has significantly reduced prevalence. Treatment targets iodine repletion.
Substernal (Intrathoracic) Goiter
- Extension below the thoracic inlet
- Can compress the trachea, SVC (superior vena cava syndrome), or esophagus
- Pemberton's sign positive
- CT chest (non-contrast) is critical for surgical planning
- Surgical resection generally via cervical incision; mediastinal extension may require manubriotomy
Pregnancy
Thyroid enlargement is physiologically normal in pregnancy. Pathologic goiter in pregnancy requires careful evaluation with thyroid function tests and ultrasound; radioiodine is contraindicated in pregnancy.
Summary Table
| Feature | Detail |
|---|---|
| Definition | Any thyroid enlargement |
| Global cause | Iodine deficiency |
| US/iodine-sufficient cause | Hashimoto's thyroiditis, Graves disease |
| Classic sign | Moves on swallowing, Pemberton's sign |
| Key trophic driver | Elevated TSH or TSH-like immunoglobulins |
| First-line imaging | Thyroid ultrasound |
| Malignancy workup | FNA for suspicious nodules |
| Medical therapy | RAI (40-60% size reduction) |
| Definitive therapy | Total/subtotal thyroidectomy |
| Surgical complication | Hypocalcemia (hypoparathyroidism) |
Sources: Goldman-Cecil Medicine (International Edition); Current Surgical Therapy 14e; Textbook of Family Medicine 9e; Costanzo Physiology 7th Edition; Gray's Anatomy for Students; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.