Mercle cell tumor role of radiotherapy
Reading File
Finding Sources
Finding Sources
Searching PubMed
Merkel cell carcinoma radiotherapy
Reading File
Reading File
Reading File
Reading Article
PMID: 39749718
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have a comprehensive set of textbook content and recent systematic review data. Let me compile the full answer.
Merkel Cell Carcinoma (MCC): Role of Radiotherapy
Merkel cell carcinoma (also spelled "Merkel" - note the correct spelling) is a rare but aggressive cutaneous neuroendocrine carcinoma. It is highly radiosensitive, and radiotherapy (RT) plays a central role across all stages of management.
Background: Why Radiotherapy Matters
MCC has a strong tendency for local recurrence and regional nodal spread. Without treatment of regional lymph nodes, recurrence is seen in 46-76% of cases. The tumor's radiosensitivity makes RT one of the most effective tools in its management. - Andrews' Diseases of the Skin, p. 761
Roles of Radiotherapy in MCC
1. Adjuvant RT After Surgery (Primary Site)
The most common application. Recommended after surgical excision even when margins are negative in most cases.
- Even after Mohs micrographic surgery, adjuvant RT reduces local recurrence rates from 16% to near 0%.
- Adjuvant RT to the primary site is "often indicated" unless all of the following low-risk features are present: primary lesion ≤1 cm, not on head/neck, no lymphovascular invasion, widely negative pathologic margins, negative SLNB, and patient is immunocompetent. - Dermatology 2-Volume Set 5e, p. 2493
A 2025 systematic review and meta-analysis (n = 46,215) confirmed that adjuvant RT (surgery + RT) significantly improved overall survival (HR = 0.78, 95% CI 0.62-0.99) and disease-free survival (HR = 0.35, 95% CI 0.13-0.93) compared to surgery alone. Adjuvant RT was more effective for local than regional disease. - Mbous et al., Cancer Med 2025 (PMID: 39749718)
2. Adjuvant RT to Regional Lymph Node Basins
- RT is directed at both the primary site and the draining/regional lymph node basins in most cases.
- Should be considered even when sentinel lymph nodes are negative, given the high occult nodal failure rate.
- Prophylactic lymph node dissection enhances local control but does not improve survival - it is gradually being replaced by RT of the affected nodal basin.
- When SLNB is positive: RT to primary site + draining lymph node basin and/or lymphadenectomy. - Andrews' Diseases of the Skin, p. 761
3. Definitive (Primary) RT - When Surgery Is Not Feasible
RT alone is a valid and effective treatment for patients unable to tolerate surgery:
- Definitive RT for MCC "confers clinically meaningful in-field locoregional control." (Gunaratne et al., JAAD 2017)
- Radiotherapy alone has been used successfully as primary treatment, particularly in elderly patients or those with comorbidities.
- Indicated when the tumor is unresectable or surgical morbidity is prohibitive. - Andrews' Diseases of the Skin, p. 761
4. Palliative RT
In Stage IV (metastatic) MCC, RT can be used for:
- Local symptom control
- Management of individual metastatic deposits
- In combination with immunotherapy (immune checkpoint inhibitors such as avelumab/pembrolizumab) or chemotherapy
Treatment Algorithm by Stage
The figure below illustrates the NCCN-aligned evaluation and treatment algorithm from Dermatology 2-Volume Set 5e:
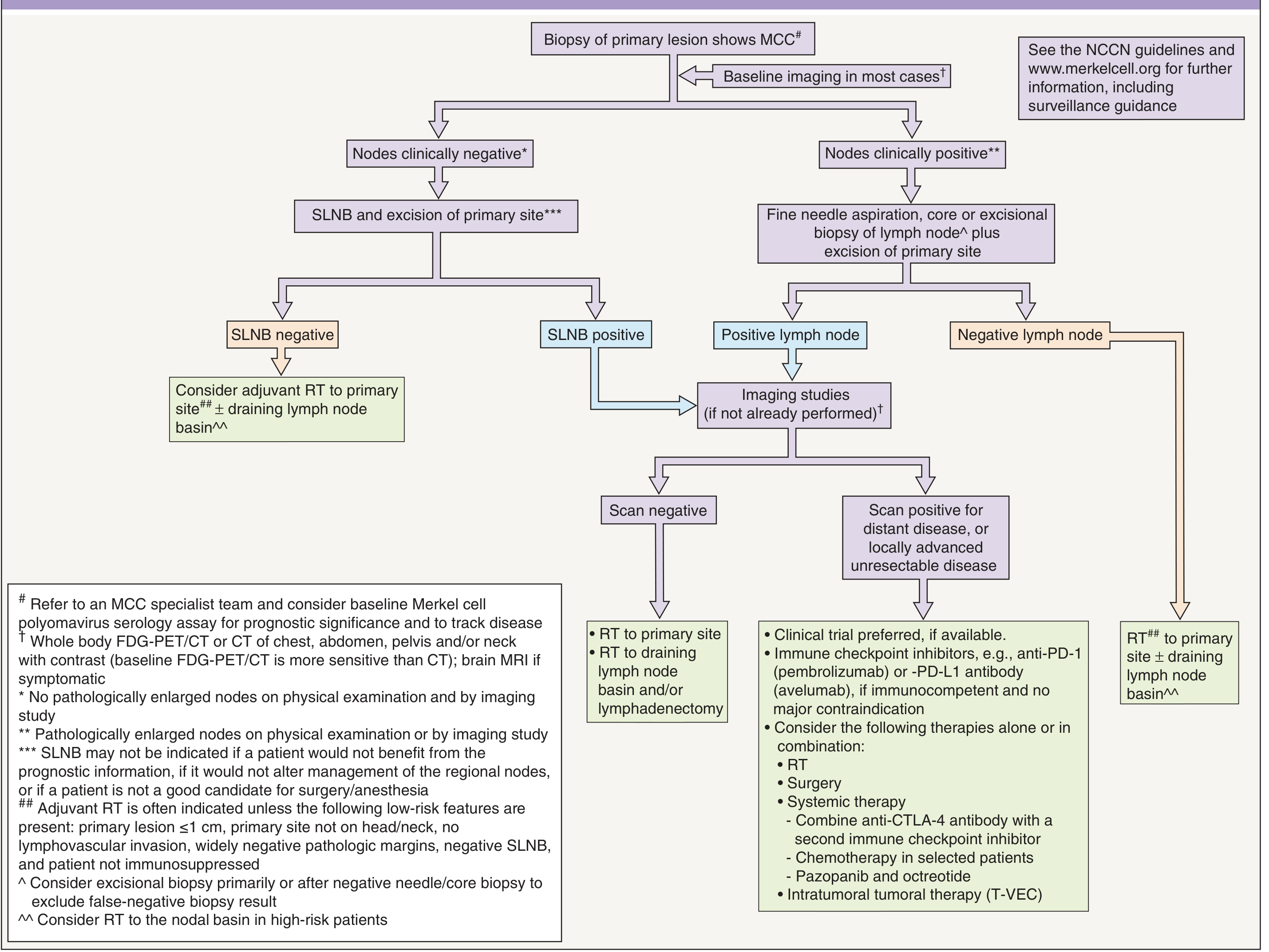
Key points from the algorithm:
- Clinically node-negative + SLNB negative: Consider adjuvant RT to primary site ± draining lymph node basin
- SLNB positive: RT to primary site + draining lymph node basin and/or lymphadenectomy
- Positive lymph nodes, scan negative: RT to primary site + draining lymph node basin ± lymphadenectomy
- Locally advanced/unresectable or scan-positive disease: Clinical trial preferred; consider RT + surgery + systemic therapy (immune checkpoint inhibitors, chemotherapy)
- Node-negative (clinically), negative lymph node biopsy: RT to primary site ± draining lymph node basin
Radiation Doses and Fields
| Setting | Typical Dose |
|---|---|
| Adjuvant (post-excision, negative margins) | 50-56 Gy |
| Adjuvant (positive or close margins) | 56-60 Gy |
| Definitive/primary (unresectable) | 60-66 Gy |
| Elective nodal irradiation | 46-50 Gy |
Field design typically includes the primary tumor bed with a 3-5 cm margin, and elective nodal fields to at-risk regional basins.
RT vs. Chemotherapy
| Feature | Radiotherapy | Chemotherapy |
|---|---|---|
| Role in local/regional disease | Primary - first-line adjuvant | Not recommended adjuvant |
| Response | High (radiosensitive tumor) | Initial response, but disease progression occurs |
| Survival benefit | Proven | No evidence for adjuvant benefit |
| Metastatic setting | Palliative | Palliative |
Traditional adjuvant chemotherapy has been disappointing and is not recommended as it does not prevent metastatic, regional, or local disease recurrence. - Andrews' Diseases of the Skin, p. 761
Special Situations
- Head and neck MCC: RT is particularly important due to complex anatomy limiting surgical margins; the head/neck is the most common site (~36% of cases).
- Immunosuppressed patients: Higher risk of recurrence; RT indication is even stronger.
- Unknown primary with nodal disease (Stage IIIA): RT to the nodal basin remains standard.
- In-transit metastases (Stage IIIB): RT can be combined with immunotherapy.
Summary
RT is the most effective non-surgical treatment for MCC. The key indications are:
- Adjuvant RT to primary site - after excision, reduces recurrence from ~16% to near 0%
- Adjuvant RT to nodal basin - even with negative SLNB in most cases
- Definitive RT - when surgery is not possible
- Palliative RT - for symptom control in metastatic disease
The emerging standard of care is surgery + adjuvant RT (both to primary site and regional lymph node basins), with immunotherapy (avelumab, pembrolizumab) reserved for advanced/metastatic disease.
Sources: Andrews' Diseases of the Skin (p. 761); Dermatology 2-Volume Set 5e (p. 2490-2493); Cummings Otolaryngology Head and Neck Surgery; Mbous et al., Cancer Med 2025 - PMID: 39749718
This is a shared conversation. Sign in to Orris to start your own chat.