Describe MI(MYOCARDIAL INFARCTION)
Reading File
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have enough rich content from authoritative textbooks. Let me compile the comprehensive answer.
Myocardial Infarction (MI)
Definition
Myocardial infarction (MI) - commonly called a "heart attack" - is necrosis of the heart muscle resulting from ischemia. The 2018 joint U.S./European Cardiology task force defines it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- Robbins & Kumar Basic Pathology, p. 354
- Harrison's Principles of Internal Medicine 22E, p. 2156
Epidemiology
- In the United States, ~605,000 patients experience a new AMI and ~200,000 experience a recurrent AMI each year
- About half of AMI-related deaths occur before reaching hospital
- In-hospital mortality has declined from ~10% to ~5%; 1-year mortality is ~15%
- Men are at greater risk than women, but the gap narrows with age; women are relatively protected during reproductive years due to estrogen
- ~10% of MIs occur before age 40; ~45% occur before age 65
- Mortality is approximately fourfold higher in patients >75 years
Harrison's Principles of Internal Medicine 22E, p. 2156
Classification (ACS Framework)
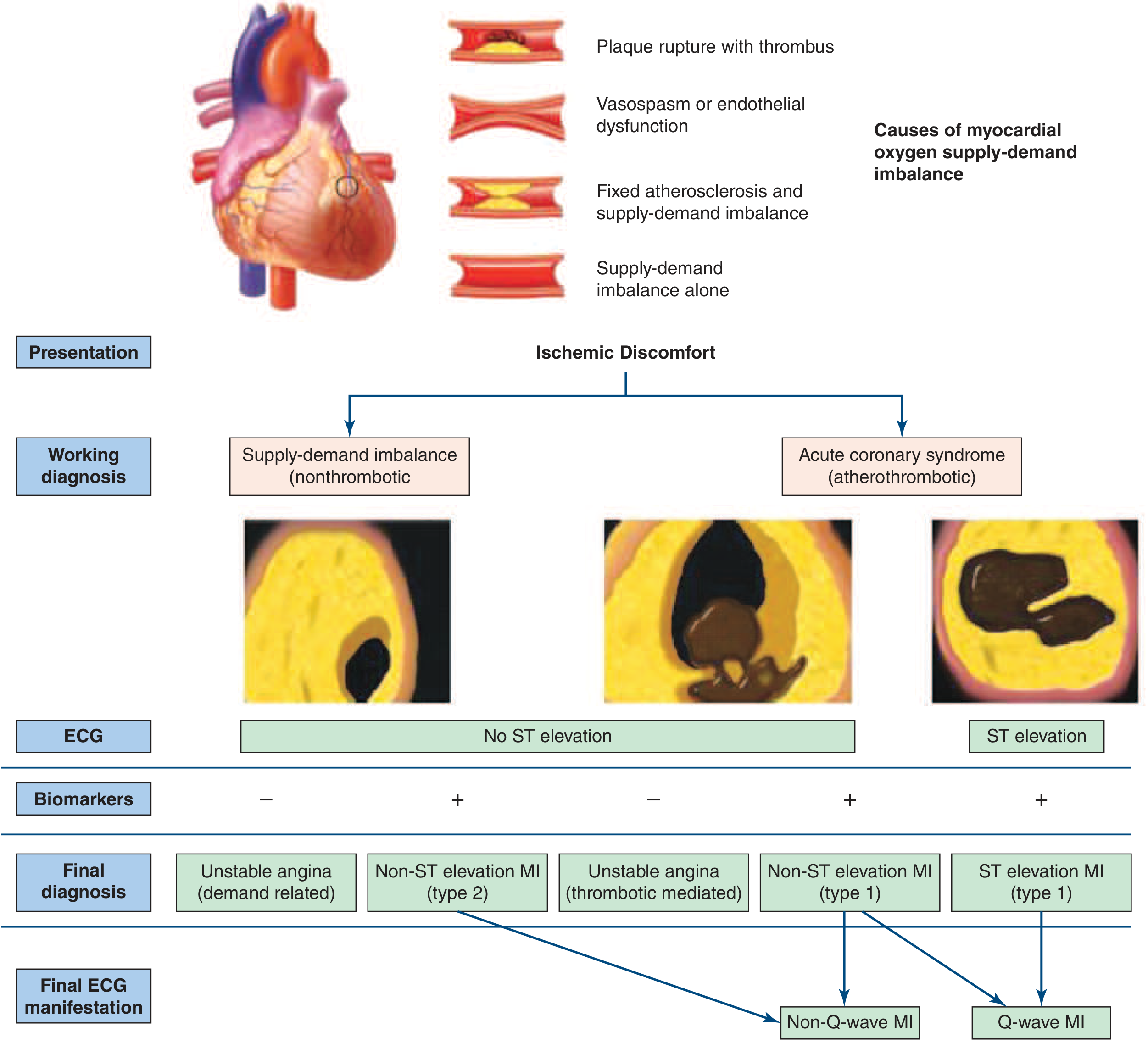
MI is a subtype of Acute Coronary Syndrome (ACS). The classification is:
| Type | ECG | Biomarkers | Key Feature |
|---|---|---|---|
| STEMI | ST elevation | Positive | Complete occlusion; Q-wave MI develops |
| NSTEMI | No ST elevation | Positive | Partial/transient occlusion; Non-Q-wave MI |
| Unstable Angina | No ST elevation | Negative | No myocardial necrosis |
Type 1 MI - spontaneous, due to atherothrombotic plaque disruption
Type 2 MI - demand-supply mismatch (vasospasm, tachycardia, hypotension, anemia) without primary plaque rupture
Harrison's Principles of Internal Medicine 22E, p. 2157
Pathogenesis
Primary Mechanism
STEMI usually occurs when coronary blood flow decreases abruptly after thrombotic occlusion of an atherosclerotic coronary artery. The sequence of events:
- An atheromatous plaque is eroded or suddenly disrupted by endothelial injury, intraplaque hemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood
- Platelets adhere, aggregate, and activate - releasing thromboxane A2, ADP, and serotonin (causing further platelet aggregation and vasospasm)
- Coagulation cascade activation via tissue factor adds to the growing thrombus
- Within minutes, the enlarging thrombus completely occludes the coronary artery lumen
- Glycoprotein IIb/IIIa receptor conformational change allows fibrinogen cross-linking, further stabilizing the thrombus
Plaques prone to rupture have a rich lipid core, thin fibrous cap, expansive remodeling, neovascularization, plaque hemorrhage, and adventitial inflammation.
Angiography within 4 hours of MI onset demonstrates coronary thrombosis in nearly 90% of cases. By 12-24 hours, evidence of thrombosis falls to 60%, even without intervention - indicating some occlusions clear spontaneously.
Robbins & Kumar Basic Pathology, p. 355 | Harrison's 22E, p. 2157
Non-atherosclerotic causes (~10% of MIs)
- Coronary vasospasm
- Embolization from mural thrombi (e.g., atrial fibrillation) or valve vegetations
- Vasculitis, amyloid deposition, sickle cell disease (small vessel occlusion)
- Cocaine abuse (vasospasm + thrombosis)
- Spontaneous coronary artery dissection
Progression of Necrosis
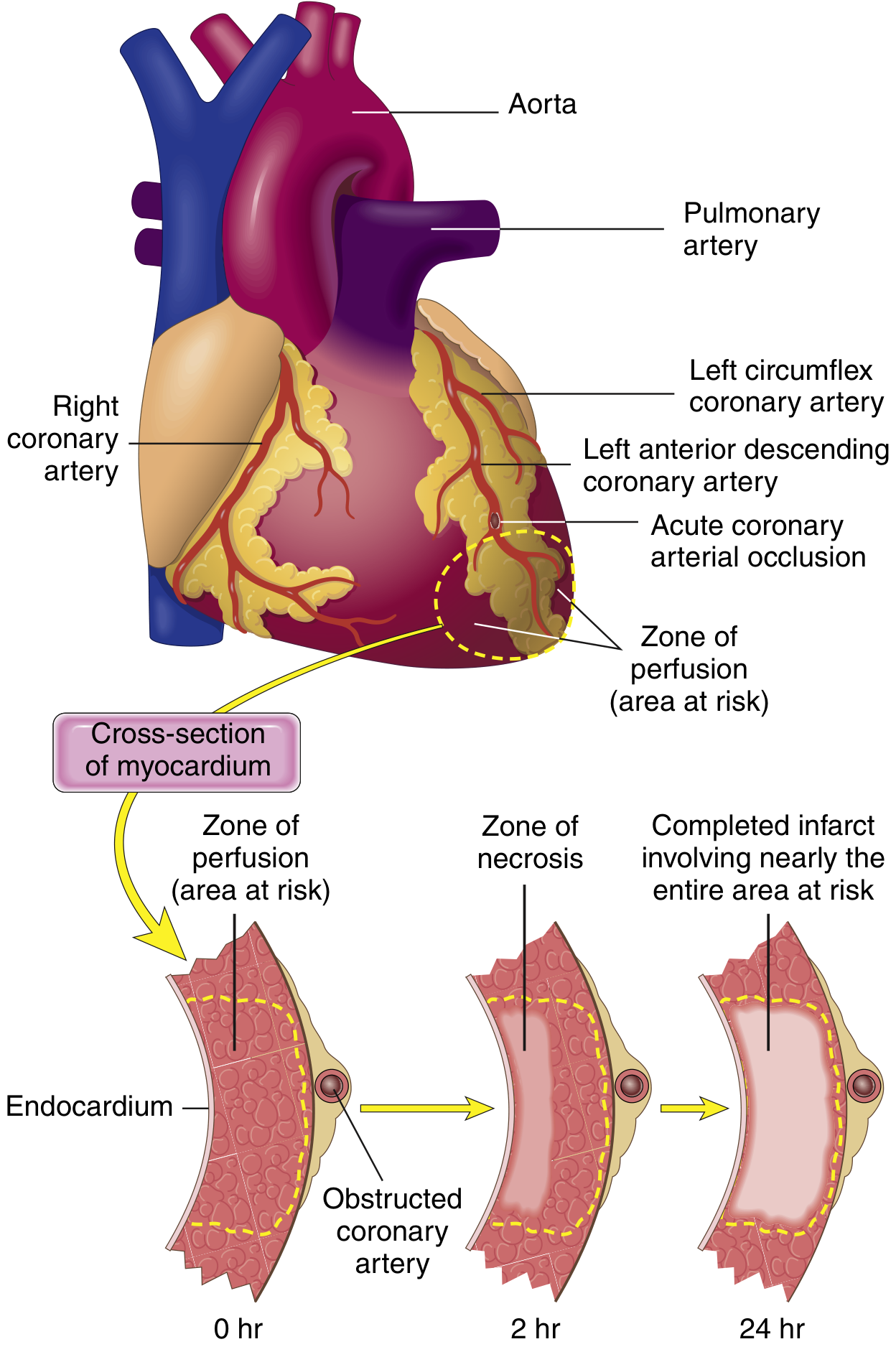
- Within seconds: aerobic metabolism ceases; ATP drops; lactic acid accumulates
- Within minutes: loss of contractility
- 20-40 minutes: irreversible damage and coagulative necrosis begins
- Necrosis starts in the subendocardial zone (most vulnerable - last to receive blood, highest intramural pressure)
- With prolonged ischemia, a wavefront of cell death moves outward through the myocardium
- Without intervention, a transmural infarct develops over 3-6 hours
Cardiac muscle requires ~1.3 mL O₂/100g/min just to remain alive. In the central portion of a large infarct where collateral flow is absent, muscle dies. Even 15-30% of normal resting coronary flow may prevent death.
Guyton & Hall Textbook of Medical Physiology, p. 271 | Robbins & Kumar Basic Pathology, p. 354
Patterns of Infarction
By Location
| Vessel Occluded | Territory Infarcted | Frequency |
|---|---|---|
| LAD (proximal) | Anterior LV, anterior 2/3 of septum, apex | 40-50% |
| RCA (proximal) | RV, posterior LV, posterior 1/3 of septum | 30-40% |
| LCX (proximal) | Lateral LV | 15-20% |
By Depth
- Transmural infarction: Full thickness; caused by complete epicardial vessel occlusion with atherosclerosis + acute thrombosis
- Subendocardial infarction: Inner 1/3 of myocardium; caused by a thrombus that lyses spontaneously or therapeutically before transmural extension occurs
- Microscopic infarcts: Small-vessel occlusions (vasculitis, emboli, vasospasm)
Robbins & Kumar Basic Pathology, p. 356
Morphology (Gross & Microscopic Changes)
Histological cross-sections of coronary atherosclerosis:
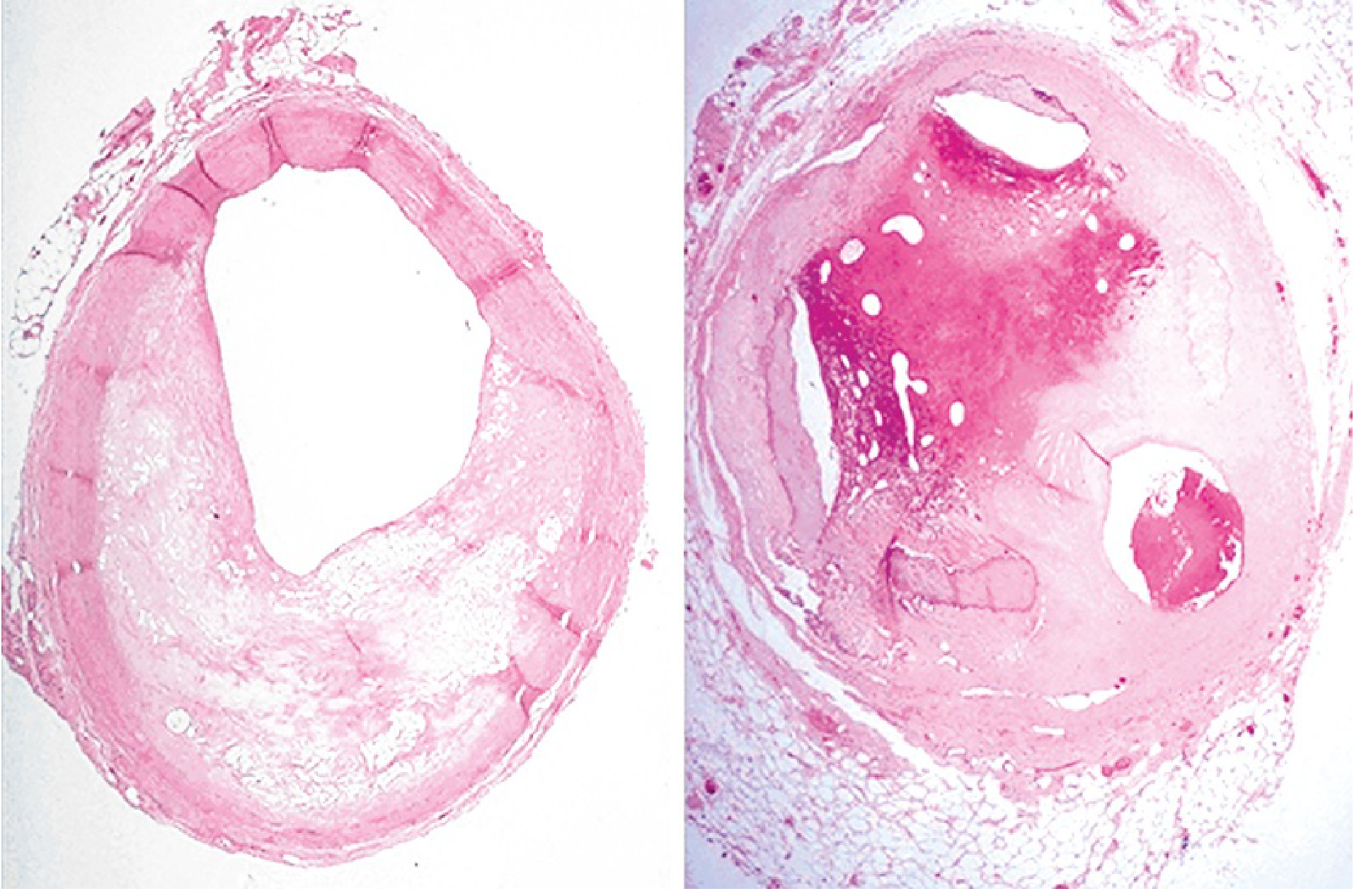
(Left: 60-70% lumen narrowing by atherosclerosis. Right: Near-complete occlusion by organized thrombus)
| Time | Gross Changes | Microscopic Changes |
|---|---|---|
| <12 hours | Usually not grossly apparent (TTC stain needed after 3 hrs) | Waviness of myofibers at periphery; stretched, thin fibers; contraction band necrosis if reperfused |
| 12-24 hrs | Dark mottling | Coagulative necrosis begins; edema; hemorrhage |
| 1-3 days | Tan/yellow pallor at center | PMN infiltration; hypereosinophilic myofibers with nuclear loss |
| 3-7 days | Yellow-tan pallor, soft (risk of rupture) | Macrophage infiltration begins; removal of necrotic debris |
| 1-3 weeks | Yellow-tan with red-pink borders | Granulation tissue; neovascularization |
| >3 weeks (months) | White scar | Dense collagenous scar |
Myocardial necrosis proceeds invariably to scar formation without significant regeneration.
Robbins & Kumar Basic Pathology, p. 356-357
Clinical Presentation
Up to half of STEMI cases have a precipitating factor: vigorous exercise, emotional stress, surgical illness, or circadian variation (morning clustering within hours of awakening).
Symptoms
- Chest pain (most common) - deep, visceral; described as heavy, squeezing, or crushing; occasionally stabbing or burning
- Pain radiates to arms (especially left), neck, jaw, back, shoulders
- More severe and prolonged than typical angina; lasts >30 minutes; not relieved by rest
- Nausea and vomiting (especially in inferior MI)
- Diaphoresis (profuse sweating)
- Dyspnea - from impaired LV function and pulmonary congestion
- Fatigue, lightheadedness
- Silent MI - occurs in ~25%, especially in diabetics and elderly; may present only with dyspnea, confusion, or syncope
Signs
- Anxious, pale, diaphoretic patient
- Tachycardia, hypotension (cardiogenic shock if large MI)
- S3 or S4 gallop; paradoxical S2 split
- Crackles at lung bases (if LV failure)
- Jugular venous distension (if RV failure)
Harrison's Principles of Internal Medicine 22E, p. 2158
ECG Changes
Three major ECG abnormalities in acute MI (Ganong's physiology):
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential (K+ loss) | Into infarct | TQ depression (seen as ST elevation) |
| Delayed depolarization | Out of infarct | ST segment elevation |
- Acute STEMI: ST elevation in leads over infarct; reciprocal ST depression in opposite leads
- Q waves develop days-weeks later when dead muscle becomes electrically silent (Q-wave MI = transmural)
- Non-Q-wave MI (NSTEMI) tends to be less severe but carries high risk of reinfarction
- "Failure of progression of R wave" in anterior LV infarction is another key finding
Ganong's Review of Medical Physiology 26E, p. 534
Cardiac Biomarkers
| Biomarker | Rises | Peaks | Returns to Normal | Notes |
|---|---|---|---|---|
| Troponin I/T (cardiac) | 3-6 hrs | 24-48 hrs | 7-14 days | Most sensitive and specific; gold standard |
| CK-MB | 4-6 hrs | 12-24 hrs | 48-72 hrs | Useful for reinfarction detection |
| Myoglobin | 1-3 hrs | 6-9 hrs | 24 hrs | Earliest but non-specific |
| LDH | 24-48 hrs | 3-6 days | 7-10 days | Historical; rarely used now |
Troponin is released as the sarcolemmal membrane is disrupted, allowing intracellular macromolecules to leak into the vasculature.
Complications
Immediate (hours)
- Ventricular fibrillation - most common cause of sudden cardiac death (80-90% of in-hospital cardiac deaths in MI setting)
- Cardiogenic shock - decreased cardiac output from systolic stretch of infarcted segments
- Acute pulmonary edema - blood damming in pulmonary vessels due to LV failure
Early (days)
- Myocardial rupture (day 3-7, peak at 1 week) - free wall rupture, papillary muscle rupture (mitral regurgitation), ventricular septal rupture
- Right ventricular infarction (with inferior MI)
- Arrhythmias: complete heart block (especially inferior MI affecting AV node via RCA)
- Pericarditis (Dressler syndrome - autoimmune, at 1-8 weeks)
Late (weeks-months)
- Left ventricular remodeling and aneurysm formation
- Mural thrombus and systemic embolism
- Chronic heart failure
- Sudden cardiac death (risk remains elevated post-MI) - a 2024 meta-analysis found the risk of sudden cardiac death post-MI remains significant for years, particularly in the first year (Peek et al., Eur Heart J 2024, PMID 39378245)
Guyton & Hall Textbook of Medical Physiology, p. 271-272 | Robbins & Kumar Basic Pathology, p. 358
Management
STEMI - Emergency Treatment (Tintinalli's Emergency Medicine)
Reperfusion is the cornerstone - "time is muscle"
| Priority | Intervention | Detail |
|---|---|---|
| Primary PCI (preferred) | Door-to-balloon time <90 min | Superior to fibrinolysis when available |
| Fibrinolysis (if PCI unavailable) | Within 12 hrs of symptom onset | Alteplase, streptokinase, tenecteplase |
| Antiplatelet agents | Aspirin 162-325 mg + P2Y12 inhibitor | Clopidogrel 600 mg loading; Ticagrelor 180 mg; Prasugrel 60 mg |
| Antithrombins | Heparin or enoxaparin | UFH: 60 units/kg bolus + 12 units/kg/h; Enoxaparin: 30 mg IV + 1 mg/kg SC |
| Beta-blockers | Reduce infarct size, arrhythmias | Avoid in cardiogenic shock, bradycardia, AV block |
| Nitrates | Reduce preload; pain relief | Avoid if hypotension or RV infarct |
| ACE inhibitors / ARBs | Reduce LV remodeling | Start within 24 hrs |
| Statins | High-intensity (atorvastatin 80 mg) | Start immediately |
| Oxygen | Only if SpO₂ <90% | Routine O₂ no longer recommended for all |
| Morphine | Pain relief + anxiolysis | Use with caution (may mask symptoms) |
Tintinalli's Emergency Medicine, p. 384-385
NSTEMI/Unstable Angina
- Antiplatelet therapy + anticoagulation
- Risk-stratify with TIMI/GRACE score
- Early invasive strategy (angiography ± PCI within 24-48 hrs) for high-risk patients
- GP IIb/IIIa inhibitors for high-risk/refractory cases or PCI
Recent Evidence Update
A 2025 meta-analysis (Chi et al., Eur J Prev Cardiol, PMID 39298680) suggests beta-blockers may have limited benefit in secondary prevention after MI in patients without reduced ejection fraction or heart failure - challenging the long-standing practice of routine post-MI beta-blockade in all patients.
Risk Factors
Modifiable: Hypertension, dyslipidemia, cigarette smoking, diabetes mellitus, obesity, sedentary lifestyle, cocaine use
Non-modifiable: Age (men >45, women >55), male sex, family history of premature CAD, post-menopausal state
Key Concepts Summary
| Feature | Detail |
|---|---|
| Core mechanism | Plaque rupture → thrombosis → coronary occlusion → ischemic necrosis |
| Most vulnerable zone | Subendocardial (highest demand, lowest supply) |
| Time to irreversible injury | 20-40 minutes |
| Window for intervention | 3-6 hours (full infarct); best within 90 min |
| Most common cause of death | Ventricular fibrillation |
| Best biomarker | Cardiac troponin I or T |
| ECG hallmark of acute MI | ST segment elevation over the infarcted area |
| Gold standard treatment | Primary PCI (door-to-balloon <90 min) |
Sources: Robbins & Kumar Basic Pathology (9780323790185); Harrison's Principles of Internal Medicine 22E (9781265977061); Guyton & Hall Textbook of Medical Physiology (9780443111013); Ganong's Review of Medical Physiology 26E (9781260122404); Tintinalli's Emergency Medicine (9781260019933)
This is a shared conversation. Sign in to Orris to start your own chat.