Uti (nephrology) everything diagnosis Pathogenesis symptoms grades preliminary diagnosis treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"urinary tract infection" AND diagnosis AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material from authoritative nephrology textbooks. Let me compile the full answer.
Urinary Tract Infection (UTI) — Nephrology Comprehensive Review
1. Definitions & Classification
UTI encompasses a spectrum of infections of the urinary tract and is categorized into six major clinical patterns:
| Category | Definition |
|---|---|
| Acute uncomplicated cystitis | Lower UTI in healthy, non-pregnant females with structurally normal urinary tract |
| Recurrent cystitis | ≥2 UTIs in 6 months or ≥3 in 12 months |
| Acute uncomplicated pyelonephritis | Upper UTI in otherwise healthy females |
| Cystitis in males | Generally considered complicated by default |
| Complicated UTI | UTI with any condition increasing risk of treatment failure or recurrence |
| Asymptomatic bacteriuria (ASB) | ≥10⁵ CFU/mL on two consecutive clean-catch specimens without symptoms |
Bacteriuria threshold:
- ASB / pyelonephritis: ≥ 10⁵ organisms/mL
- Symptomatic cystitis: as few as 10²–10³ CFU/mL in the presence of pyuria and symptoms
- Complicated UTI: ≥ 10³ CFU/mL (females), ≥ 10⁴ CFU/mL (males)
Comprehensive Clinical Nephrology, 7th ed., Ch. 53
2. Epidemiology
- Several million acute uncomplicated cystitis episodes annually in the US
- ~250,000 episodes of acute pyelonephritis per year
- Incidence of cystitis in sexually active young females: ~0.5 per person-year
- Recurrence occurs in 27–44% of healthy females
- Pyelonephritis in young females: ~3 per 1,000 person-years
- Postmenopausal females: ~10% per year symptomatic UTI
- Adult males <50 y: 5–8 per 10,000 annually (much lower than females)
- Catheter-associated UTI (CAUTI): the most common source of gram-negative bacteremia in hospitalized patients
3. Pathogenesis
Route of Infection
- Ascending route (most common): Uropathogens from rectal/perineal flora colonize the urethra → bladder → ureter → renal parenchyma. Women are at higher risk due to a shorter urethra.
- Hematogenous route: Less common; occurs with organisms like Staphylococcus aureus or Candida in immunocompromised patients.
Microbial Virulence Factors
- Type 1 fimbriae (mannose-sensitive): mediate adhesion to bladder epithelium
- P fimbriae / Pap pili (mannose-resistant): critical for ascending to kidney; bind Gal-Gal moieties on uroepithelium — strains with P fimbriae are strongly associated with pyelonephritis
- Hemolysin, aerobactin, serum resistance: additional virulence factors of uropathogenic E. coli (UPEC)
- Toxin production and iron acquisition further facilitate upper tract infection
Bacterial Biofilm & Intracellular Reservoir
UPEC can form intracellular bacterial communities (IBCs) within superficial urothelial cells, enabling persistence and recurrence despite antibiotic treatment.
Host Defense Mechanisms
- Urine flow / voiding: flushes bacteria mechanically
- Urinary IgA, lactoferrin, Tamm-Horsfall protein (uromodulin): binding of type 1 fimbriated bacteria
- Urothelial exfoliation: sheds bacteria attached to luminal cells
- Neutrophil influx (pyuria): innate response to lipopolysaccharide (LPS) signaling via TLR4
Predisposing Conditions
- Female anatomy, sexual activity, spermicide use, lack of estrogen (postmenopausal)
- Urinary tract obstruction (stones, BPH, strictures)
- Vesicoureteral reflux (VUR)
- Diabetes mellitus (impaired neutrophil function, glucosuria)
- Neurogenic bladder, indwelling catheter
- Pregnancy (physiologic hydronephrosis/stasis; 70% of pyelonephritis cases have preceding bacteriuria)
- Immunosuppression, sickle cell disease, polycystic kidney disease
Comprehensive Clinical Nephrology, 7th ed., Ch. 53; Tintinalli's Emergency Medicine, Ch. 91
4. Causative Organisms
| Organism | Notes |
|---|---|
| Escherichia coli | >80% of uncomplicated UTIs; >70% in pregnancy |
| Staphylococcus saprophyticus | 2nd most common in young sexually active females |
| Klebsiella pneumoniae | Common in complicated/nosocomial UTI |
| Proteus mirabilis | Urease-producing; associated with struvite stones, obstruction, diabetes |
| Enterococcus faecalis | More common in complicated/catheter-associated UTI |
| Pseudomonas aeruginosa | Nosocomial/catheter-associated; often MDR |
| Candida spp. | Catheter-associated; immunosuppressed; diabetics |
| Group B Streptococcus | Pregnancy |
5. Symptoms & Clinical Presentation
Lower UTI (Cystitis)
- Dysuria (burning on urination)
- Urgency and frequency
- Strangury (slow, painful passage of urine drop by drop)
- Suprapubic discomfort / pressure
- Hematuria (in hemorrhagic cystitis)
- Malodorous / turbid urine
- Absence of fever (typically — fever suggests upper tract involvement)
Upper UTI (Pyelonephritis)
- Fever (≥38°C), rigors/chills
- Flank pain / costovertebral angle (CVA) tenderness
- Loin pain (unilateral or bilateral)
- Nausea, vomiting
- Systemic malaise, headache
- Lower urinary tract symptoms (in ~50–60% of cases)
- May progress to urosepsis: hypotension, tachycardia, confusion, multi-organ dysfunction
Complicated UTI — Additional Features
- Vague or nonspecific symptoms: fatigue, irritability, abdominal/back pain
- Presentations can be atypical, especially in elderly, diabetic, immunocompromised, or catheterized patients
- Occult renal or prostatic seeding common even when presenting as "cystitis"
Asymptomatic Bacteriuria (ASB)
- By definition: no symptoms. Important in pregnancy and pre-urological procedures; screen and treat; do not treat in most other populations
6. UTI Classification / Grades (Severity & Complexity)
By Anatomical Level
| Grade | Location | Condition |
|---|---|---|
| 1 | Urethra | Urethritis |
| 2 | Bladder | Cystitis |
| 3 | Ureter | Ureteritis |
| 4 | Renal pelvis | Pyelitis |
| 5 | Renal parenchyma | Pyelonephritis |
By Complexity (Clinical Classification)
| Type | Definition |
|---|---|
| Uncomplicated UTI | Young, healthy, non-pregnant female; structurally normal urinary tract; no comorbidities |
| Complicated UTI | Any UTI with complicating factor (see Box below) |
| CAUTI | UTI in catheterized patient |
| Recurrent UTI | ≥2 in 6 months or ≥3 in 12 months |
Complicating Factors (Box 53.2, Comprehensive Nephrology):
- Male sex
- Pregnancy
- Urinary catheter, stent, or nephrolithiasis
- Neurogenic bladder / spinal cord injury
- Diabetes mellitus, sickle cell disease
- Immunosuppression (chemotherapy, HIV, transplant)
- Polycystic kidney disease
- Urinary tract obstruction
- Structural genitourinary anomaly
- Advanced age / nursing home residency
- Recent GU instrumentation
- Known antibiotic resistance
Severe Upper Tract Patterns (Imaging-Defined)
| Entity | Features |
|---|---|
| Acute lobar nephronia (Acute bacterial nephritis) | Focal renal parenchymal inflammation without abscess; CT shows wedge-shaped hypodense area |
| Renal abscess | Liquefied necrotic collection; requires drainage if ≥3 cm |
| Emphysematous pyelonephritis | Gas-forming infection (E. coli, Klebsiella); diabetics; CT diagnostic; mortality up to 40% |
| Xanthogranulomatous pyelonephritis | Chronic destructive infection (Proteus, E. coli); staghorn calculus; CT shows "bear paw" sign |
| Pyonephrosis | Infected, obstructed collecting system; emergency drainage required |
7. Preliminary (Clinical) Diagnosis
History
- Duration, character, and combination of urinary symptoms
- Sexual activity, contraception (spermicide use)
- Previous UTIs, antibiotics, culture results
- Comorbidities (diabetes, renal disease, immunosuppression)
- Catheter or recent instrumentation
- Fever/chills → suggests pyelonephritis
Physical Examination
- CVA tenderness (Murphy's kidney punch) → pyelonephritis
- Suprapubic tenderness → cystitis
- Pelvic/vaginal exam to exclude STI
- Urethral discharge → urethritis / STI
- Signs of sepsis: hypotension, tachycardia, fever, altered mental status
Urinalysis (Dipstick + Microscopy)
| Test | Finding | Significance |
|---|---|---|
| Leukocyte esterase | Positive | Pyuria (>5 WBC/HPF) — sensitivity ~75–96% |
| Nitrite | Positive | Gram-negative bacteria (E. coli, Klebsiella, Proteus); low sensitivity ~35–85% |
| Both positive | High specificity for UTI | Best dipstick combination |
| Microscopy | WBC casts | Upper UTI / pyelonephritis |
| Hematuria | RBCs | Common in hemorrhagic cystitis |
| Bacteria | Gram stain of uncentrifuged urine | 1 organism/HPF ≈ 10⁵ CFU/mL |
Urine Culture
- Gold standard
- When to obtain: All cases of pyelonephritis, complicated UTI, males, pregnancy, treatment failure, recurrent UTI, prior to urological procedures
- When culture may be omitted: Typical uncomplicated cystitis in young females (clinical diagnosis sufficient)
- Sensitivity & susceptibility guides targeted therapy
Blood Tests
- CBC with differential: leukocytosis with left shift in pyelonephritis/urosepsis
- CRP, procalcitonin (elevated in upper tract / systemic infection)
- Blood cultures (2 sets): obtain in pyelonephritis requiring admission, urosepsis
- BMP/renal function (creatinine, BUN, electrolytes) — especially in complicated/severe UTI
- Blood glucose (screen for undiagnosed diabetes)
Imaging
| Modality | Indication | Finding |
|---|---|---|
| Renal ultrasound | First-line; pyelonephritis not responding to treatment; obstruction | Hydronephrosis, abscess, stones |
| CT abdomen/pelvis (without contrast) | Suspected obstruction (stone), abscess, emphysematous PNeph | Gold standard for stones, gas, abscess |
| CT with contrast | Renal abscess, lobar nephronia, focal lesion characterization | Wedge-shaped perfusion defects, ring-enhancing abscess |
| VCUG / Cystogram | Children with first febrile UTI (grade III–V VUR evaluation); adults with recurrent UTI | VUR grading |
| DMSA renal scan | Gold standard for renal cortical scarring / differential renal function | Photopenic areas = scarring |
Standard admission: admitted patients require imaging if no clinical improvement within 48–72 h
8. Treatment
A. Uncomplicated Cystitis (Young, Non-pregnant Female)
| Antibiotic | Dose | Duration |
|---|---|---|
| Nitrofurantoin macrocrystals | 100 mg twice daily | 5 days (preferred 1st line) |
| TMP-SMX | 160/800 mg twice daily | 3 days (use only if local resistance <20%) |
| Fosfomycin trometamol | 3 g sachet single dose | 1 day |
| Pivmecillinam | 400 mg twice daily | 3–5 days |
| Fluoroquinolone (ciprofloxacin) | 250 mg twice daily | 3 days (reserve for complicated cases) |
Fluoroquinolones should be reserved due to collateral damage (resistance, C. difficile, tendinopathy). Nitrofurantoin contraindicated if eGFR <30 mL/min.
B. Uncomplicated Pyelonephritis (Outpatient)
| Antibiotic | Dose | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg PO BID or 1000 mg XR once daily | 7 days |
| TMP-SMX | 160/800 mg PO BID | 14 days (if susceptible) |
| Levofloxacin | 750 mg PO once daily | 5 days |
| β-lactam (e.g., ceftriaxone) | Initial IV dose, then oral step-down | 10–14 days |
C. Complicated UTI (Including Inpatient Pyelonephritis)
| Severity | Antibiotic | Duration |
|---|---|---|
| Moderate illness, oral tolerated | Fluoroquinolone (ciprofloxacin 500 mg BID or levofloxacin 750 mg OD) | 10–14 days |
| Severe / hospitalization required | IV ceftriaxone 1–2 g q24h; or piperacillin-tazobactam 3.375 g IV q6h; or cefepime 2 g IV q8–12h | 14 days; step-down when improving |
| Urosepsis | Broad-spectrum IV (pip-tazo / carbapenem); blood cultures; ICU if shocked | Until source controlled + clinical response |
| MDR P. aeruginosa | Ceftazidime-avibactam 2.5 g IV q8h or ceftolozane-tazobactam 1.5 g IV q8h | 10–14 days |
| Renal abscess ≥3 cm | Percutaneous or surgical drainage + prolonged antibiotics | 4–6 weeks |
| Emphysematous PNeph | IV antibiotics + percutaneous nephrostomy; nephrectomy if severe | Until stable; individualized |
D. UTI in Pregnancy
| Condition | First-line | Duration | Notes |
|---|---|---|---|
| ASB | Amoxicillin or cephalexin; nitrofurantoin | 7 days | Screen all women; treat all positive cultures |
| Cystitis | As ASB; follow-up culture | 7 days | Avoid TMP in 1st trimester (antifolate) |
| Pyelonephritis | Broad-spectrum IV (cephalosporin/penicillin) → oral step-down + suppression | 14 days then suppression until delivery | Hospital admission standard; AKI in 25%; recurrence rate 6–8% |
E. Asymptomatic Bacteriuria — Treat Only In:
- Pregnancy (screen and treat all)
- Pre-urological/cystoscopic procedure
- Renal transplant recipients (controversial — only within first month post-transplant)
Do NOT treat ASB in: healthy non-pregnant women, elderly/institutionalized patients, diabetics without symptoms, catheterized patients (unless pre-procedure or immunosuppressed) — treatment increases resistance risk without clinical benefit.
F. Recurrent UTI — Prevention
- Behavioral modification: post-coital voiding, hydration, avoid spermicide
- Post-coital prophylaxis: TMP-SMX 40/200 mg or nitrofurantoin 50 mg within 2 hours
- Continuous low-dose prophylaxis: nitrofurantoin 50–100 mg nightly or TMP-SMX 40/200 mg nightly (6–12 months)
- Self-start therapy (patient-initiated): for compliant patients with classic symptoms
- Topical estrogen (postmenopausal): restores lactobacilli flora, reduces recurrences
- Cranberry products: modest evidence; proanthocyanidins inhibit fimbriated E. coli adhesion
- Treat underlying anatomic abnormality (VUR, obstruction, stones) if identified
G. Catheter-Associated UTI (CAUTI)
- Remove catheter if clinically feasible — this alone resolves many infections
- 7–10 days for complicated CAUTI
- Avoid treating asymptomatic bacteriuria in catheterized patients
- Consider catheter change for symptomatic CAUTI before starting antibiotics
9. Vesicoureteral Reflux (VUR) Grade & Nephrology Significance
VUR is graded I–V (International Reflux Study Classification):
| Grade | Finding | Risk |
|---|---|---|
| I | Reflux into ureter only | Minimal |
| II | Reflux to renal pelvis without dilation | Low |
| III | Mild dilation of ureter and collecting system | Moderate |
| IV | Moderate dilation; blunting of fornices | High — renal scarring |
| V | Gross dilation; tortuous ureter; severe intrarenal reflux | Highest — reflux nephropathy, CKD |
VUR + UTI = reflux nephropathy (commonest cause of renal scarring in children) → focal cortical scarring → CKD, hypertension, proteinuria. DMSA scan quantifies scarring.
10. Complications
| Complication | Notes |
|---|---|
| Urosepsis | 20–30% of all gram-negative bacteremia; high mortality if delayed |
| Renal abscess | Inadequate treatment of pyelonephritis; drainage required |
| Emphysematous pyelonephritis | Diabetics; gas-forming organisms; mortality 40% without nephrectomy |
| Reflux nephropathy / CKD | Recurrent pyelonephritis + VUR; leads to hypertension and ESRD |
| Papillary necrosis | Diabetics, analgesic nephropathy, sickle cell; ischemic necrosis of papillae |
| Perinephric abscess | Extension of renal abscess into Gerota's fascia |
| Preterm labor / IUGR | Pyelonephritis in pregnancy |
| Antibiotic resistance / MDR organisms | Especially nosocomial / CAUTI |
Key Mnemonics & Quick-Reference
DNUTS — organisms causing UTI: Dysuria = E. coli (>80%), Klebsiella, Proteus, UTI = Staph saprophyticus in young women, Enterococcus, S. aureus
"Complicated" UTI — think DAMPNESS: Diabetes, Abnormality (anatomic/functional), Male sex, Pregnancy, Neurogenic bladder, Extremes of age, Stones/stents, Suppressed immunity
Recent Evidence Update (PubMed 2024–2025)
- [PMID 39495518] — WikiGuidelines Group 2024 consensus (JAMA Network Open): comprehensive UTI guidelines for pediatrics and adults, emphasizing antibiotic stewardship and limiting fluoroquinolone use.
- [PMID 40228579] — 2025 meta-analysis (Clin Microbiol Infect): short-course antibiotics for pyelonephritis/complicated UTI comparable to long courses in RCTs — supports 5–7 day therapy where possible.
- [PMID 38916643] — Systematic review on catheter replacement in CAUTI: catheter removal/replacement at time of antibiotic initiation remains recommended.
Sources: Comprehensive Clinical Nephrology, 7th Ed. (Ch. 53 & 44) | Tintinalli's Emergency Medicine, Ch. 91 | Goldman-Cecil Medicine | Robbins & Cotran Pathologic Basis of Disease | NKF Primer on Kidney Diseases, 8th Ed.
Pyelonephritis in detail (mbbs nephrology)
Finding Sources
Finding Sources
Searching Images
acute pyelonephritis kidney pathology gross histology
Reading File
Reading File
Reading File
Searching Images
chronic pyelonephritis kidney cortical scarring histology microscopy
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material from Harrison's, Robbins & Cotran, Campbell-Walsh, Tintinalli, and Comprehensive Clinical Nephrology. I have enough to compile a detailed MBBS-level answer.
Pyelonephritis — Detailed MBBS Nephrology Notes
1. Definition
Pyelonephritis is an infection of the upper urinary tract — specifically involving the renal parenchyma and pelvicalyceal system. It is differentiated from cystitis (lower UTI) primarily by the presence of systemic features and tissue-invasive infection.
- Acute pyelonephritis (APN): Acute suppurative bacterial infection of the kidney
- Chronic pyelonephritis (CPN): Repeated or persistent renal infection leading to progressive scarring, calyceal deformity, and eventual loss of renal function
Harrison's Principles of Internal Medicine, 22e, Ch. 140; Tintinalli's Emergency Medicine, Ch. 91
2. Epidemiology
- ~250,000 episodes of acute pyelonephritis annually in the US
- Incidence in young females: ~3 per 1,000 person-years
- More common in pregnant women with urological abnormalities or diabetes
- Right kidney more commonly affected in pregnancy (greater physiologic ureteral dilation on right)
- ~70% of women who develop APN have preceding covert bacteriuria
- Up to 30% of women with untreated asymptomatic bacteriuria develop pyelonephritis
3. Etiology / Causative Organisms
| Organism | Frequency | Notes |
|---|---|---|
| E. coli | >70–80% | Most common; P-fimbriated strains especially virulent |
| Klebsiella pneumoniae | Common | Especially complicated/nosocomial UTI |
| Proteus mirabilis | Common | Urease-producing; associated with staghorn calculi |
| Enterococcus faecalis | Less common | Catheter-associated |
| Staphylococcus aureus | Less common | Hematogenous route; suspect distant source |
| Staphylococcus saprophyticus | Young females | Second most common cause of uncomplicated UTI |
| Pseudomonas aeruginosa | Nosocomial/complicated | Often multidrug-resistant |
| Candida spp. | Catheterized/immunosuppressed | Fungal pyelonephritis |
4. Pathogenesis
A. Routes of Infection
1. Ascending Route (Most Common — >95%):
Perineal/fecal flora → Urethra → Bladder → Ureter → Renal pelvis → Parenchyma
- Women are at higher risk due to shorter urethra (4 cm vs. 20 cm in males)
- Predisposed by: sexual activity, pregnancy (hydroureter/stasis), VUR, obstruction
2. Hematogenous Route (~5%):
- S. aureus, Candida seed the kidney from a distant bacteremic source
- Leads to cortical (not medullary) abscess formation initially
- Suspect in IV drug users, endocarditis, immunocompromised
B. Bacterial Virulence Factors
| Factor | Function |
|---|---|
| P fimbriae (Pap pili) | Bind Gal-Gal receptors on uroepithelium; key virulence determinant for renal invasion |
| Type 1 fimbriae | Bind mannose receptors on bladder urothelium (mannose-sensitive) |
| Hemolysin (HlyA) | Lyses RBCs, releases iron; promotes tissue damage |
| Aerobactin / Siderophores | Iron acquisition; essential for growth in tissues |
| Serum resistance | Survives complement → bacteremia |
| Flagella | Motility; facilitate ascending migration |
| LPS (lipopolysaccharide) | Triggers TLR4 → IL-6/IL-8 → neutrophil recruitment → pyuria |
C. Host Risk Factors
- Female sex (anatomic)
- Vesicoureteral reflux (VUR) — allows ascent of infected urine to kidney
- Urinary obstruction (stones, BPH, strictures, tumor) — impairs flushing
- Pregnancy — progesterone-mediated ureteral dilation → stasis
- Diabetes mellitus — impaired neutrophil chemotaxis, glucosuria, autonomic neuropathy → incomplete bladder emptying
- Neurogenic bladder — incomplete voiding
- Indwelling catheters / urinary stents
- Immunosuppression (HIV, transplant, chemotherapy)
- Polycystic kidney disease — cysts as protected niches
- Previous UTI / renal scarring
5. Pathology
A. Acute Pyelonephritis
Gross Pathology:
- Kidney enlarged, swollen, congested
- Cortical surface shows multiple yellow-white abscesses (suppurative foci)
- Pelvis and calyces are hyperemic, may contain pus
- In severe cases: cortical and medullary involvement with necrotic foci
Microscopic (Histopathology):
- Polymorphonuclear leukocyte (neutrophil) infiltration of the renal interstitium and tubules — the hallmark
- Tubular necrosis — tubules filled with neutrophils forming "neutrophilic tubular casts"
- Preservation of glomeruli in early stages (glomeruli are relatively resistant)
- Interstitial edema and vascular congestion
- WBC casts in tubular lumens — pathognomonic of upper UTI (renal parenchymal involvement)
- Granulomatous inflammation → suspect fungal (Aspergillus, Candida) or mycobacterial (TB) infection
B. Chronic Pyelonephritis
Gross Pathology:
- Kidney diffusely contracted, scarred, and pitted
- Scars are "Y-shaped," flat, broad-based depressions with red-brown granular bases
- Scarring is preferentially polar (upper and lower poles — where intrarenal reflux is greatest)
- Calyceal blunting and dilation underlying cortical scars
- Parenchyma thin; loss of corticomedullary demarcation
- Asymmetric involvement (unlike symmetric diabetic nephropathy)
Microscopic:
- Patchy interstitial fibrosis with lymphocytes, plasma cells, occasional PMNs
- Tubular atrophy and dilation — "thyroidization of the kidney" (colloid-like casts in atrophic tubules, resembling thyroid follicles)
- Periglomerular fibrosis → eventual glomerular obsolescence
- Vascular changes in advanced disease (intimal thickening)
- Compensatory hypertrophy of surviving nephrons
6. Clinical Features
Acute Pyelonephritis
| Feature | Details |
|---|---|
| Fever | High-grade (>38.5°C), chills, rigors |
| Flank pain | Unilateral or bilateral; dull ache or colicky |
| CVA tenderness | Costovertebral angle tenderness on percussion — hallmark sign |
| Loin pain | Radiates to ipsilateral iliac fossa or groin |
| Nausea / Vomiting | Common — often limits oral intake |
| Systemic malaise | Headache, myalgias, fatigue |
| Lower urinary symptoms | Dysuria, frequency, urgency in ~50–60% (preceding cystitis) |
| Onset | Acute — hours to 1–2 days |
Severe/Complicated Features:
- High fever, rigors, hypotension → urosepsis (septic shock)
- Acute kidney injury (AKI) — especially in pregnancy (25% of gestational pyelonephritis), bilateral disease, obstruction
- Mental status changes in elderly
Chronic Pyelonephritis
- Asymptomatic until renal insufficiency develops
- History of recurrent febrile UTIs with fever, flank pain, dysuria
- Hypertension (common in advanced disease)
- Polyuria/nocturia (tubular dysfunction — impaired concentrating ability)
- Anemia of chronic kidney disease
- Signs and symptoms of CKD in advanced stages
7. Diagnosis
Clinical Assessment
| Step | Findings |
|---|---|
| History | Acute fever + flank/loin pain + urinary symptoms; sexual activity, prior UTI, diabetes, pregnancy |
| Examination | CVA tenderness (Murphy's kidney punch), fever, tachycardia |
Urinalysis
| Test | Expected Finding | Significance |
|---|---|---|
| Pyuria | >5 WBC/HPF or positive leukocyte esterase | Hallmark of UTI |
| Bacteriuria | Positive nitrites (gram-negative); visible bacteria | Supports infection |
| WBC casts | Cylindrical casts of white cells | Pathognomonic of renal parenchymal infection — distinguishes pyelonephritis from cystitis |
| Hematuria | RBCs present | Common; not specific |
| Proteinuria | Mild (tubular) | Reflects tubular damage |
| Nitrite test | Positive → gram-negative uropathogens | Sensitivity 35–85%, high specificity |
Urine Culture (Gold Standard)
- Quantitative culture: ≥10⁵ CFU/mL of single uropathogen (classic threshold)
- Culture and sensitivity mandatory in all cases of pyelonephritis
- Collect mid-stream clean-catch specimen before antibiotics
- Sensitivity and susceptibility guide targeted therapy
Blood Investigations
| Test | Expected Finding |
|---|---|
| CBC | Leukocytosis with left shift (neutrophilia), bandemia |
| CRP / Procalcitonin | Elevated; PCT particularly useful for upper tract/systemic infection |
| Blood cultures | Positive in 15–20% of hospitalized pyelonephritis cases (2 sets before antibiotics) |
| Serum creatinine/BUN | Elevated if AKI complicating pyelonephritis |
| Serum glucose | Screen for undiagnosed diabetes |
| Electrolytes | Metabolic derangements in sepsis/AKI |
Imaging
CT Abdomen/Pelvis with contrast (gold standard for complications):
- Striated nephrogram — wedge-shaped, lobar hypodense areas extending from medulla to cortex (pathognomonic of focal bacterial nephritis)
- Perinephric stranding — inflammatory reaction
- Renal/perinephric abscess — ring-enhancing fluid collection
- Gas in renal tissue → emphysematous pyelonephritis
- Hydronephrosis → obstruction (stone/stricture)

CECT abdomen showing wedge-shaped hypoperfusion areas in the right kidney — classic "striated nephrogram" of acute pyelonephritis.
Renal Ultrasound:
- First-line in pregnancy, children, and bedside evaluation
- May be normal in uncomplicated APN (poor sensitivity ~30%)
- Shows: hydronephrosis, abscess, echogenic kidney, stones, reduced corticomedullary differentiation
- Cannot diagnose focal APN reliably
DMSA (Dimercaptosuccinic Acid) Scintigraphy:
- Gold standard for detecting cortical scarring
- Shows photopenic (cold) areas = scars from past episodes
- Used in children post-febrile UTI to assess for reflux nephropathy
Chronic Pyelonephritis Imaging (IVP / CT urography):
- Asymmetric, irregular, contracted kidneys
- Calyceal clubbing and blunting
- Cortical scars overlying dilated calyces
- Cortical thinning — preferentially at poles
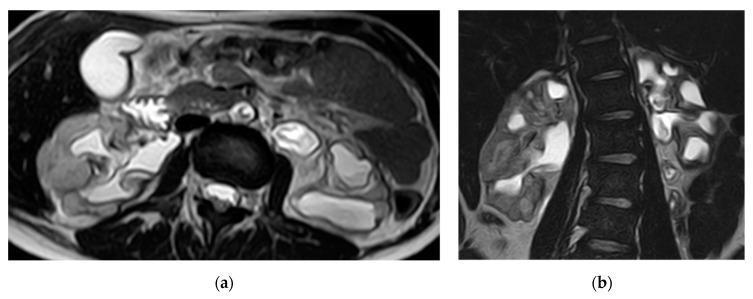
MRI bilateral chronic pyelonephritis — atrophic kidneys, irregular contours, calyceal dilation (calyceal clubbing), classic end-stage sequelae of recurrent pyelonephritis.
VCUG (Voiding Cystourethrogram):
- Detects and grades vesicoureteral reflux (VUR)
- Important in children with first febrile UTI and in adults with recurrent pyelonephritis
8. Complicated Forms of Pyelonephritis
A. Acute Lobar Nephronia (Acute Bacterial Nephritis)
- Severe focal form of pyelonephritis without liquefaction/abscess
- CT: wedge-shaped hypodense mass, does not rim-enhance
- Treat with prolonged IV antibiotics (2–3 weeks); abscess may develop if undertreated
B. Renal Cortical Abscess
- Localized liquefactive necrosis within renal parenchyma
- Often from hematogenous route (S. aureus) in IVDU / endocarditis
- CT: ring-enhancing fluid-filled cavity
- Management: Antibiotics alone if <3 cm; percutaneous drainage if ≥3 cm; nephrectomy if nonfunctioning
C. Renal Corticomedullary Abscess
- From ascending route (complicated UTI, obstruction)
- CT: fluid-filled lesion crossing corticomedullary junction
- Percutaneous drainage + antibiotics
D. Perinephric Abscess
- Extension of infection through the renal capsule into Gerota's fascia
- May track into psoas muscle, diaphragm, or flank
- Hallmark: No improvement after 4–5 days of antibiotics for apparent pyelonephritis
- CT: collection with surrounding fat stranding in perirenal space
- Management: Percutaneous drainage (even small abscesses >3 cm) + prolonged antibiotics (4–6 weeks); nephrectomy if nonfunctioning kidney
E. Emphysematous Pyelonephritis (EPN)
- Life-threatening gas-forming infection of the renal parenchyma
- Organisms: E. coli, Klebsiella (facultative anaerobes fermenting glucose → gas)
- Occurs almost exclusively in poorly controlled diabetics
- CT (diagnostic): gas within renal parenchyma, perinephric space, or collecting system
- Mortality up to 40% without nephrectomy
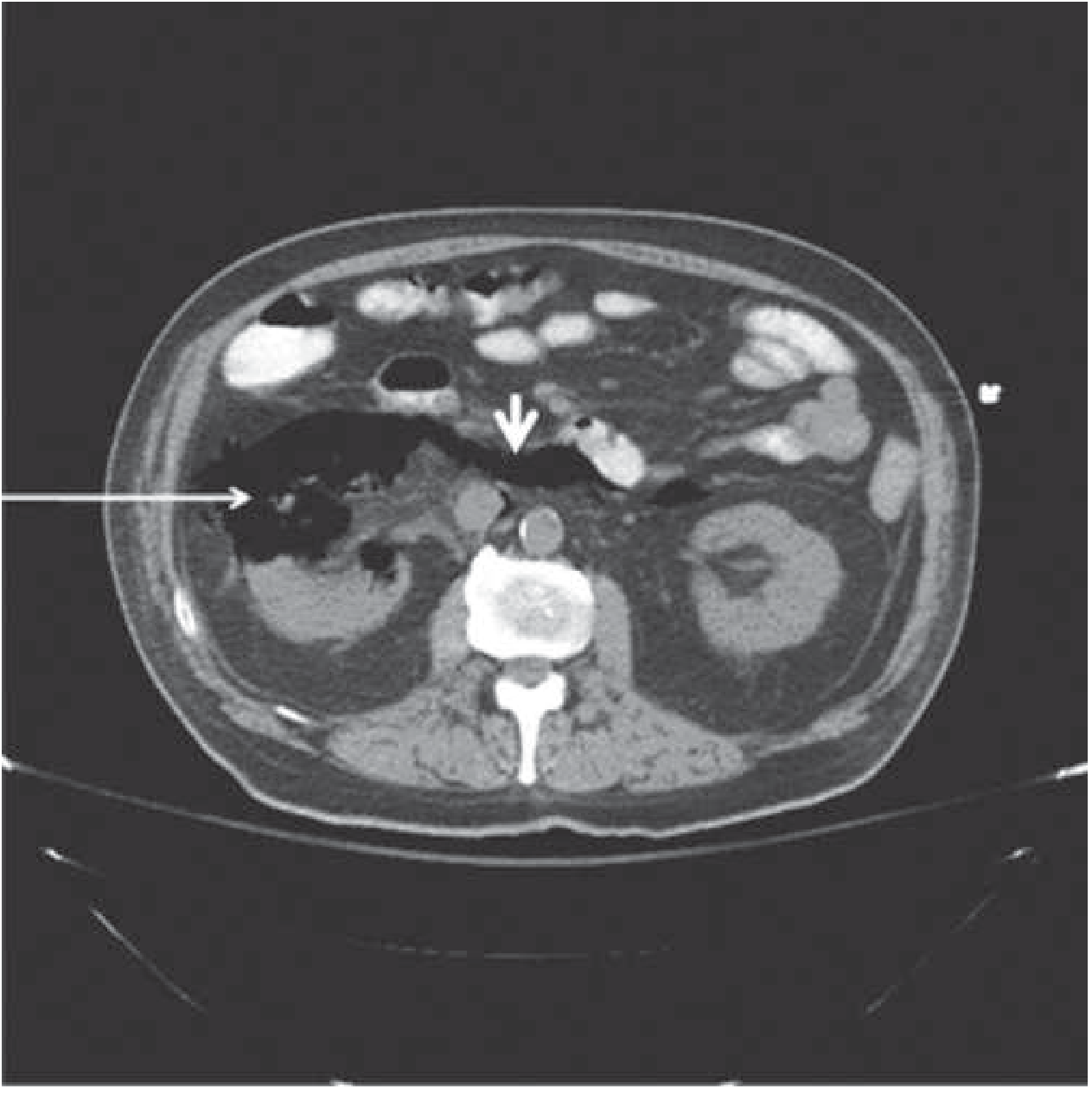
CT: Emphysematous pyelonephritis — gas destruction of right renal parenchyma (arrow) tracking through retroperitoneal space.
- Management: Aggressive IV antibiotics + percutaneous nephrostomy as initial intervention; elective nephrectomy if required
F. Emphysematous Cystitis
- Gas within the bladder wall (not parenchyma)
- Also in diabetics; less severe than EPN
- CT: air in bladder wall
- Usually responds to IV antibiotics alone
G. Xanthogranulomatous Pyelonephritis (XGP)
- Chronic, destructive, suppurative granulomatous inflammation of the kidney
- Caused by: chronic obstruction (staghorn calculus) + chronic infection (Proteus mirabilis 38%, E. coli 33%)
- Virtually always unilateral; F:M = 2:1; middle-aged women
- Pathology: Replacement of renal parenchyma by lipid-laden foamy macrophages (xanthoma cells) + granulomatous tissue + areas of necrosis
- Extension into perinephric fat, psoas, diaphragm possible
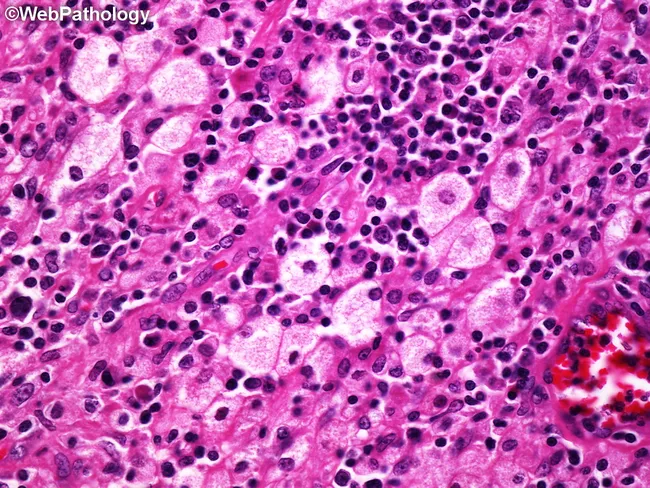
H&E: XGP — foamy (lipid-laden) macrophages, lymphocytes, plasma cells, necrosis — classical xanthogranulomatous reaction.
- Clinical features: Fever, flank/abdominal pain, weight loss, anorexia, recurrent UTIs; all patients have renal calculi; nonfunctioning kidney
- CT: Enlarged kidney, multiple fluid-filled cavities replacing parenchyma, staghorn calculus, perinephric involvement — "bear paw sign"
- Differential: Renal cell carcinoma, renal TB, renal abscess
- Management: Nephrectomy (definitive); antibiotics have only secondary role. Partial nephrectomy if early/focal disease
H. Pyonephrosis
- Infected, obstructed collecting system (pus filling the hydronephrotic kidney)
- Medical emergency: urosepsis + renal destruction if untreated
- Ultrasound: hydronephrosis with echogenic debris
- Management: Emergency nephrostomy or ureteric stent to decompress + IV antibiotics; definitive treatment of obstruction thereafter
I. Renal Papillary Necrosis
- Ischemic necrosis of renal papillae complicating pyelonephritis
- Especially in: diabetes, sickle cell disease, analgesic nephropathy, obstruction
- Sloughed papillae may obstruct ureter → obstructive AKI
- Bilateral papillary necrosis → rapid rise in serum creatinine
- IVP/CT: "ring shadow" or "lobster claw" deformity of calyx
9. Treatment
A. Uncomplicated Acute Pyelonephritis (Outpatient)
Indications for outpatient treatment:
- Clinically stable, tolerating oral fluids, mild-moderate illness, no complicating factors
| Antibiotic | Dose | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg PO BID | 7 days (preferred 1st line) |
| Ciprofloxacin XR | 1000 mg PO OD | 7 days |
| Levofloxacin | 750 mg PO OD | 5 days |
| TMP-SMX | 160/800 mg PO BID | 14 days (if susceptible; avoid if local resistance >20%) |
| Oral β-lactam (amoxicillin-clavulanate) | 875/125 mg PO BID | 10–14 days (less effective; use with caution) |
Consider initial parenteral dose (IV ceftriaxone 1 g or IM gentamicin) before discharge for reliable empirical coverage, especially if local fluoroquinolone resistance is a concern.
NEVER use for pyelonephritis: Nitrofurantoin, fosfomycin, pivmecillinam — inadequate tissue levels.
B. Severe / Hospitalized Pyelonephritis (Inpatient IV Therapy)
Indications for admission:
- Unable to tolerate oral medications (vomiting)
- Urosepsis / hemodynamic instability
- Pregnancy
- Extremes of age (elderly, neonates)
- Immunocompromised / diabetics with severe illness
- Suspected obstruction or abscess
- No improvement after 48–72 h outpatient therapy
| Antibiotic (IV) | Dose | Notes |
|---|---|---|
| Ceftriaxone | 1–2 g IV q24h | Preferred 1st-line IV β-lactam |
| Cefepime | 1–2 g IV q8–12h | Broader spectrum |
| Piperacillin-tazobactam | 3.375 g IV q6h (or 4.5 g q8h) | If broad-spectrum needed |
| Meropenem / Imipenem | 500 mg–1 g IV q8h | MDR organisms, severe sepsis |
| Gentamicin/Amikacin | Based on weight / CrCl | With ampicillin for enterococcal cover |
| Fluoroquinolone IV | Ciprofloxacin 400 mg IV q8–12h | Only if IV required; switch to oral when tolerating |
Step-down to oral therapy: once afebrile and clinically improving (usually 48–72 h)
Total duration: 7–14 days total (IV + oral). Recent meta-analysis (PMID 40228579, 2025) supports shorter courses (5–7 days) for fluoroquinolones when patient responds rapidly.
C. Pyelonephritis in Pregnancy
- Admit all pregnant women (standard practice)
- IV cephalosporin (ceftriaxone) or ampicillin + gentamicin until afebrile → oral step-down
- Total course: 14 days
- Oral suppressive antibiotics until delivery to prevent recurrence (recurrence rate 6–8%)
- AKI in 25% — monitor renal function
- Avoid fluoroquinolones (cartilage toxicity, teratogenicity), TMP in 1st trimester
D. Complicated Pyelonephritis / MDR Organisms
| Organism / Situation | Agent |
|---|---|
| ESBL-producing E. coli/Klebsiella | Ertapenem or meropenem |
| Pseudomonas aeruginosa | Cefepime, piperacillin-tazobactam, ciprofloxacin |
| MDR P. aeruginosa / difficult-to-treat | Ceftazidime-avibactam 2.5 g IV q8h; ceftolozane-tazobactam 1.5 g IV q8h |
| Carbapenem-resistant organisms (CRO) | Ceftazidime-avibactam; cefiderocol; consult ID |
| S. aureus (hematogenous abscess) | Anti-staphylococcal β-lactam (oxacillin); vancomycin if MRSA |
| Enterococcus | Ampicillin + gentamicin; vancomycin if VRE |
Non-antibiotic management (essential):
- Correct obstructing lesion (stone removal, stent, nephrostomy)
- Remove catheter/stent if possible
- Drain any abscess ≥3 cm (percutaneous under CT/US guidance)
- Nephrectomy for emphysematous PNeph (severe) or XGP
E. Follow-up After Treatment
| Action | When |
|---|---|
| Urine culture | 5–7 days post-treatment; repeat at 4–6 weeks |
| Renal imaging (USS/CT) | No improvement within 48–72 h of antibiotics |
| Urological evaluation | Men (any age), children (first febrile UTI), recurrent pyelonephritis |
| DMSA scan | Children with febrile UTI to detect renal scarring |
| VCUG | To evaluate for VUR in children with febrile UTI or recurrent pyelonephritis |
10. Complications
| Complication | Mechanism / Notes |
|---|---|
| Urosepsis / Septic shock | Gram-negative bacteremia; mortality if delayed |
| Acute kidney injury (AKI) | Bilateral disease, obstruction, sepsis; 25% in gestational pyelonephritis |
| Renal abscess | Inadequate treatment; requires drainage |
| Perinephric abscess | Extension beyond capsule; requires drainage + prolonged antibiotics |
| Emphysematous pyelonephritis | Diabetics; gas-forming bacteria; high mortality |
| Papillary necrosis | Ischemia; sloughed papillae may cause obstruction |
| Reflux nephropathy / CKD | Repeated pyelonephritis + VUR → cortical scarring → hypertension → ESRD |
| Hypertension | From renin activation in scarred kidney |
| "Thyroid kidney" (chronic) | Histological — atrophic tubules filled with colloid-like casts |
| Preterm labor / IUGR | In pregnancy |
11. Chronic Pyelonephritis → Reflux Nephropathy
The most clinically important long-term consequence of recurrent pyelonephritis, especially combined with VUR:
VUR (Grade III–V) + Recurrent UTI
↓
Intrarenal reflux → bacteria reach collecting ducts
↓
Inflammatory response → fibrosis → cortical scar
↓
Loss of nephrons → compensatory hypertrophy of remaining nephrons
↓
Hypertension + proteinuria + progressive CKD → ESRD
"Thyroidization of the kidney" — a histological term for chronic pyelonephritis:
- Dilated atrophic tubules filled with eosinophilic, colloid-like casts
- Resembles thyroid follicles microscopically
- Surrounded by interstitial fibrosis and lymphocytic infiltration
12. Key Differentials of Pyelonephritis
| Condition | Distinguishing Features |
|---|---|
| Appendicitis | Right lower quadrant pain; no urinary symptoms; UA usually normal |
| Nephrolithiasis | Colicky severe pain; hematuria; no fever (unless obstructed+infected) |
| Ovarian pathology | Women; pelvic US diagnostic |
| Psoas abscess | Psoas sign; often from vertebral osteomyelitis/Crohn's |
| Renal tuberculosis | "Sterile pyuria" (acid-fast bacilli on ZN stain); chronic; "putty kidney" |
| Renal cell carcinoma | Painless hematuria; CT shows enhancing mass |
| Perinephric abscess | Failure to defile despite 4–5 days antibiotics |
| Liver abscess (right) | Right upper abdominal pain; no urinary symptoms; US/CT diagnostic |
13. MBBS Exam High-Yield Points
| Key Fact | Detail |
|---|---|
| Most common organism | E. coli (>70–80%) — P-fimbriated strains |
| WBC casts | Pathognomonic of upper UTI (renal parenchymal involvement) |
| CVA tenderness | Most important clinical sign |
| CT finding | Striated/wedge-shaped nephrogram = classic APN |
| Thyroidization of kidney | Chronic pyelonephritis — atrophic tubules with colloid-like casts |
| XGP | Foamy macrophages + staghorn calculus + nonfunctioning kidney → nephrectomy |
| Emphysematous PNeph | Diabetics + gas-forming bacteria (E. coli, Klebsiella) → nephrectomy |
| Pyonephrosis | Emergency drainage (nephrostomy) |
| Drugs to AVOID in PNeph | Nitrofurantoin, fosfomycin (insufficient tissue penetration) |
| Duration of treatment | 7 days fluroquinolone; 14 days TMP-SMX; 14 days + suppression in pregnancy |
| No improvement at 72 h | Imaging mandatory to exclude abscess/obstruction |
| Reflux nephropathy | VUR + recurrent pyelonephritis → cortical scarring → CKD + hypertension |
| DMSA scan | Gold standard for renal scarring in children |
Sources: Harrison's Principles of Internal Medicine, 22e | Comprehensive Clinical Nephrology, 7th ed. | Tintinalli's Emergency Medicine, 9e | Robbins & Cotran Pathologic Basis of Disease | Campbell-Walsh-Wein Urology | Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.