Meniers disease in detail its etiopathogenesis, diagnosis, clinical features , medical management and surgery for meiners from standard ent textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent! I now have comprehensive data from both Cummings Otolaryngology and Scott-Brown's. Let me compile the complete detailed answer.
Ménière's Disease - A Comprehensive ENT Textbook Review
Sources: Cummings Otolaryngology Head and Neck Surgery, 6th Ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 | K.J. Lee's Essential Otolaryngology
1. Definition
Ménière's disease (MD) is defined as idiopathic endolymphatic hydrops - a disorder of the inner ear characterized by recurring attacks of spontaneous vertigo, fluctuating sensorineural hearing loss, tinnitus, and aural fullness. The eponym honors Prosper Ménière, who in 1861 first recognized the inner ear as the source of these attacks.
2. Epidemiology
- Incidence varies widely: ~17/100,000 (Japan) to 513/100,000 (Finland). In the US, approximately 1 in 500 persons is affected.
- More prevalent in Caucasians, with roughly equal gender distribution (slight female predominance in some series).
- Peak age of onset: 4th and 5th decades (though it can occur at almost any age).
- Bilateral disease occurs in 19-24% of patients; onset of bilateral disease may occur decades after unilateral symptoms.
- Familial occurrence in 10-20% of cases, with autosomal dominant inheritance suggested; also autosomal recessive and mitochondrial patterns described.
3. Etiopathogenesis
3a. The Endolymphatic Hydrops Theory (Core Pathology)
The hallmark pathologic finding is distortion of the membranous labyrinth due to over-accumulation of endolymph (endolymphatic hydrops). This was simultaneously reported by Hallpike & Cairns, and by Yamakawa in 1938.
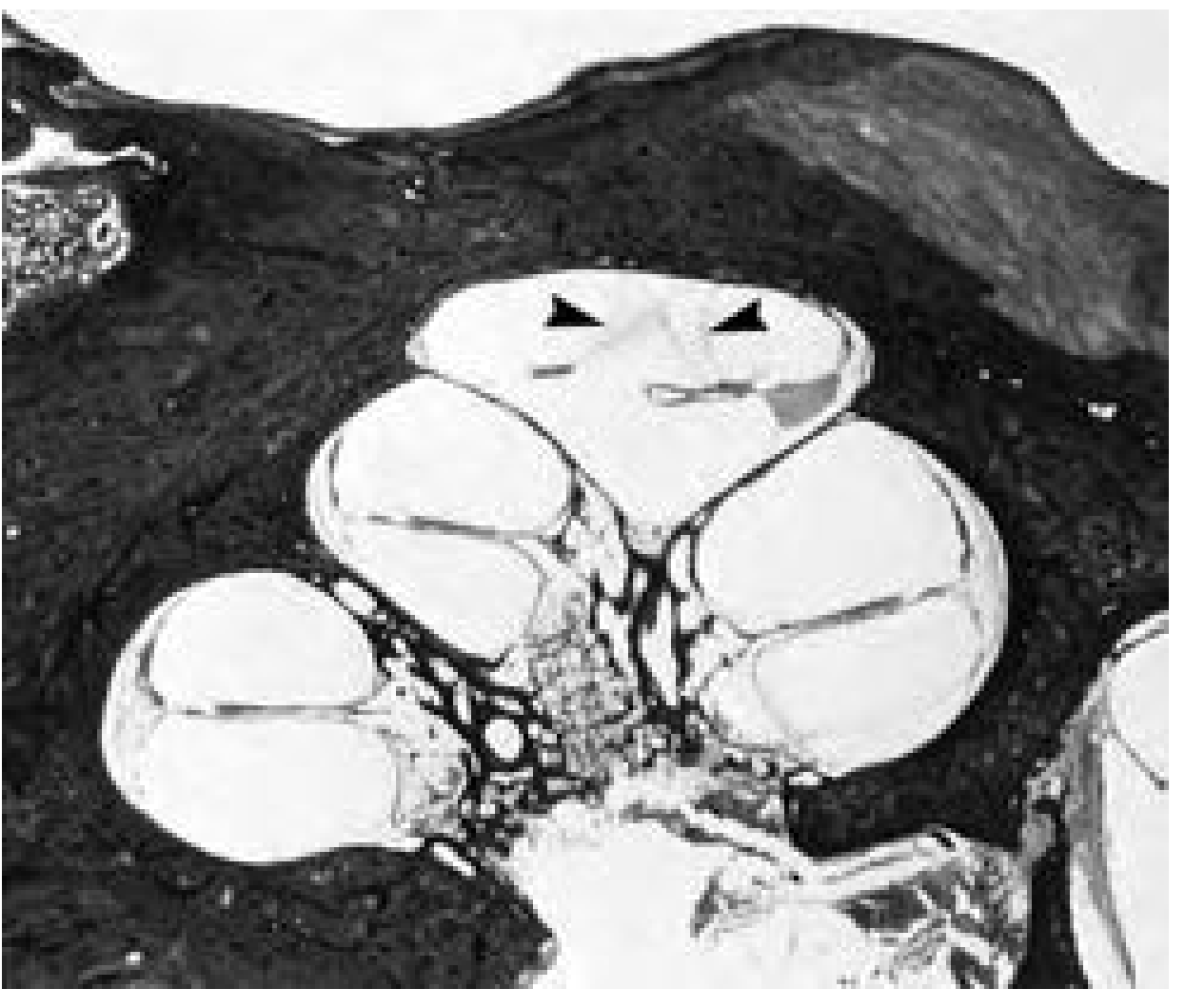
Photomicrograph: Cross-section of human cochlea showing endolymphatic hydrops. Note distension of Reissner's membrane into the scala tympani (arrowheads). Cummings Otolaryngology, Fig. 167.3
Key points on pathophysiology:
- Endolymph is produced by the stria vascularis (cochlea) and dark cells (vestibular labyrinth), circulating in radial and longitudinal fashion.
- In hydrops, the pathophysiology is controversial, but inadequate absorption by the endolymphatic sac is the prevalent theory.
- The endolymphatic duct may act as a valve to regulate endolymph homeostasis.
- Distension occurs at the expense of the perilymphatic space.
- Endolymphatic hydrops is uniformly observed in temporal bones of MD patients - but it is not pathognomonic, as hydrops has been found in temporal bones of patients without the classic MD symptoms.
- Membrane ruptures were proposed to cause acute attacks (mixing of K+-rich endolymph with perilymph), but Merchant et al. found ruptures in patients without a history of vertigo, undermining this as the sole explanation.
- Current thinking: hydrops may be a marker of disordered inner ear homeostasis, with an unknown factor producing both the clinical symptoms and the hydrops. - Cummings Otolaryngology
3b. Contributing Etiological Factors
Autoimmune factors:
- Present in approximately 1 in 3 patients.
- Theories include cross-reactions between similar antigens, innocent bystander damage via cytokine release, acquired intolerance to inner ear antigens (sequestered antigens exposed by trauma/infection), and genetic MHC-linked factors.
- HLA associations: HLA B8/DR3 and Cw7 linked to MD (possibly autoimmune etiology in these individuals).
- Polymorphisms of heat-shock protein 70 gene, PTPN22, and interleukin-1 gene (IL1) have been implicated.
Genetic factors:
- Familial MD is more prone to bilateral presentation.
- MHC associations identified; COCH-gene mutations implicated in some hereditary cases.
- Gluten sensitivity has recently been implicated as a possible etiology.
Viral factors:
- Herpes simplex virus most commonly implicated.
- Viral structures observed by electron microscopy in vestibular ganglion cells of one MD patient.
- Vertigo control in 91% of MD patients treated with acyclovir supports viral etiology.
- Delayed endolymphatic hydrops: symptomatic hydrops occurring many years after unexplained deafness, suggesting a viral insult can trigger late-onset hydrops.
Allergic factors:
- Derebery demonstrated association with allergy; vertigo control (Class A/B) achieved in 47.9% of patients accepting allergy treatment.
- Mechanisms: endolymphatic sac targeted by allergic reaction; deposition of circulating immune complexes in fenestrated blood vessels of the endolymphatic sac and stria vascularis; viral antigen-allergic T-cell interaction.
Vascular factors:
- Endolymphatic hydrops impairs blood flow autoregulation.
- Combination of hydrops + venous obstruction shown to induce Ménière-like vertigo attacks in animal models.
Anatomical factors:
- Cone-beam CT studies identify anatomical variations in the temporal bone that may predispose to blockage of the endolymphatic canal.
- Foreign protein deposition in perilymph can also cause hydrops.
4. Diagnostic Criteria
The 2015 Bárány Society / AAO-HNS / EAONO / Japanese Society for Equilibrium Research diagnostic criteria are the current gold standard:
| Diagnosis | Criteria |
|---|---|
| Definite Ménière's disease | ≥2 definitive spontaneous episodes of vertigo lasting 20 minutes to 12 hours PLUS audiometrically documented low- to mid-frequency SNHL in the affected ear on at least one occasion PLUS fluctuating aural symptoms (hearing loss, tinnitus, or fullness) in the affected ear - other causes excluded |
| Probable Ménière's disease | ≥2 episodes of vertigo or dizziness each lasting 20 minutes to 24 hours PLUS fluctuating aural symptoms (hearing, tinnitus, or fullness) in the reported ear - other causes excluded |
| Certain Ménière's disease (historical) | Definite MD + histopathologic confirmation at autopsy |
- Scott-Brown's, Table 63.1
AAO-HNS Staging (Hearing Level Staging)
Based on the 4-frequency pure tone average (PTA) of 500, 1000, 2000, and 3000 Hz:
| Stage | PTA (dBHL) |
|---|---|
| Stage 1 (mild) | ≤25 dB |
| Stage 2 (moderate) | 26-40 dB |
| Stage 3 (moderately severe) | 41-70 dB |
| Stage 4 (severe) | >70 dB |
5. Clinical Features
Triad / Tetrad
- Episodic vertigo (96.2%): most distressing symptom
- Fluctuating SNHL (87.7%): low-frequency, typically unilateral
- Tinnitus (91.1%): low-pitched, roaring quality, ipsilateral
- Aural fullness/pressure: a sense of pressure or plugging in the affected ear
The Typical Attack
- Often preceded by an aura: increasing fullness in the ear, rising tinnitus, hearing change
- Attacks may also be sudden without warning
- Duration: 20 minutes to several hours (most commonly 2-3 hours)
- Attacks lasting >24 hours should cast doubt on the diagnosis
- Accompanied by nausea, vomiting, diaphoresis, diarrhea
- Horizontal nystagmus is the cardinal finding; direction varies over the course of an attack (initially toward the affected ear, then away)
- No loss of consciousness
- Post-attack: fatigue, disequilibrium, which may persist for days
Variable Presentation
- Early disease may show predominantly either vestibular or auditory complaints.
- Kitahara series: 50% presented with vertigo + hearing loss together; 19% with vertigo only; 26% with only deafness.
- "Cochlear Ménière" and "vestibular Ménière" are subtypes not endorsed by AAO-HNS.
Special Presentations
Tumarkin Crises (Otolithic Crises / Drop Attacks):
- Sudden unexplained falls without loss of consciousness or vertigo
- Reported in 2-6% of MD patients
- Due to abrupt utriculosaccular dysfunction generating an erroneous vertical gravity reference via the vestibulospinal pathway
- Occur in clusters then spontaneously remit
- Risk of significant injury
Lermoyez Syndrome:
- Tinnitus and hearing loss precede the onset of vertigo; when the vertiginous episode occurs, the tinnitus and hearing loss dramatically resolve
- Attributed to hydrops and membrane ruptures isolated to the basal cochlear turns and saccule
Natural History
- Highly variable; patients often have clusters of attacks separated by long remissions
- Vertigo ceases spontaneously in 57% within 2 years, and 71% by 8.3 years (Silverstein)
- Progressive sensorineural hearing loss accumulates over time, typically beginning in low frequencies and eventually becoming flat or all-frequency
- Vestibular responsiveness of the affected ear decreases over time (partial compensation)
- Disease is emotionally disabling in addition to physically incapacitating
6. Investigations
Pure Tone Audiometry (PTA)
- Low-frequency SNHL initially (250-1000 Hz affected first)
- Fluctuating pattern early; becomes flat at later stages
- "Tent-shaped" audiogram (poorer at low and high frequencies, relative preservation at 2 kHz) in early disease
- Minimum of 30 dB hearing loss at two frequencies distinguishing from the better ear required for diagnosis by AAO-HNS
Electrocochleography (ECoG)
- Records sound-evoked electrical activity near the cochlea (transtympanic or extratympanic)
- Evaluates SP/AP (summating potential / action potential) ratio - enlarged SP reflects basilar membrane displacement toward scala tympani (hydrops marker)
- Diagnostic thresholds: SP/AP ratio >0.42 (extratympanic) or >0.35 (transtympanic) using click stimuli
- Elevated SP on tone-burst stimuli: <-2 µV (<-3 µV at 1 kHz) transtympanically
- Sensitivity: large SP found in approximately 50-70% of MD patients
- SP can be reduced with hyperosmotic substances (e.g., glycerol), a diagnostic maneuver
COCHLEAR HYDROPS ANALYSIS MASKING PROCEDURE (CHAMP)
- Alternative ECoG-based diagnostic tool
Vestibular Testing
- Caloric testing: may show canal paresis (reduced response) on the affected side
- VEMP (Vestibular Evoked Myogenic Potentials): can assess saccular and utricular function
- vHIT (Video Head Impulse Test): may show reduced gain on affected side in later disease
- Rotational chair testing
Imaging
- MRI with gadolinium (IV or intratympanic):
- Delayed MRI after intratympanic/IV gadolinium injection visualizes endolymphatic hydrops in vivo
- Can confirm endolymphatic hydrops as in vivo surrogate for histopathologic confirmation
- Unilateral MD often shows bilateral hydrops on delayed Gd-MRI
- Mandatory to exclude vestibular schwannoma and other CPA lesions, inner ear malformations, neurovascular conflicts
- Rule out white matter lesions (inflammatory, vasculoischaemic)
Blood Tests
- Thyroid function tests (if thyroid disease suspected)
- Immunological panel (if autoimmune disease suspected)
- HLA typing in familial cases
- COCH-gene mutation screening in familial MD
Differential Diagnosis
Important differentials include (with their criteria available for comparison):
- Vestibular migraine (headache features, photophobia/phonophobia with vestibular episodes)
- Vestibular paroxysmia (very short <1 min attacks, neurovascular conflict on MRI)
- Chronic subjective dizziness
- Labyrinthitis, perilymphatic fistula, autoimmune inner ear disease, superior canal dehiscence
7. Medical Management
Step 1 - Lifestyle and Dietary Measures (First Line)
Low-sodium diet:
- Traditional cornerstone of MD management
- Reduces endolymphatic pressure/volume
- Recommended sodium intake: <1500-2000 mg/day (typically <2 g/day)
- Luxford et al. demonstrated that compliance with low-sodium and caffeine-free diet for >6 months produced statistically significant improvement in vertigo frequency and functional level, with higher Class A/B vertigo outcomes - Scott-Brown's
- Avoidance of caffeine (vasoconstrictive, may exacerbate hydrops)
- Avoid alcohol, monosodium glutamate, and nicotine
Stress reduction:
- Stress is a well-recognized precipitant of attacks
- Relaxation techniques, vestibular rehabilitation, and cognitive behavioral therapy are adjuncts
Step 2 - Pharmacological Medical Management
Diuretics (first-line medical therapy):
- Hydrochlorothiazide (alone or combined with triamterene - Dyazide/Maxzide)
- Acetazolamide (carbonic anhydrase inhibitor)
- Mechanism: reduce endolymphatic volume and pressure
- Cochrane analysis (Thirwall & Kundu, 2006): insufficient high-quality evidence of effect, yet diuretics remain first-line in many clinics due to clinical experience
- Monitor for: electrolyte disturbances, drug interactions
Betahistine dihydrochloride:
- Oral histamine analogue - weak H1 agonist, potent H3 receptor antagonist
- H3 antagonism increases histamine release at the stria vascularis, improving microcirculation; also proposed to increase endolymphatic absorption
- Marketed specifically for MD in Europe (not approved in the US)
- Standard dose: 16 mg three times daily; high-dose regimens up to 480 mg/day reported effective in refractory cases (case series)
- Cochrane analysis (James & Burton, 2001): insufficient high-quality evidence; most trials showed some vertigo control but methodology was flawed
- Very well tolerated; generally considered safe
Vestibular suppressants (symptomatic - acute attack):
- Antihistamines: meclizine (25-50 mg), dimenhydrinate, promethazine
- Benzodiazepines: diazepam, lorazepam (reduce vestibular excitability, useful acutely)
- Antiemetics: prochlorperazine, ondansetron
- These are used for symptom relief during attacks and are not disease-modifying
Allergy treatment:
- In patients with identified allergic etiology, allergy immunotherapy/desensitization
- Derebery reported Class A/B vertigo control in 47.9% with allergy treatment
Antiviral therapy:
- Acyclovir considered in cases suspected of viral etiology
Step 3 - Intratympanic (IT) Therapies (Salvage Medical Treatment)
Intratympanic (IT) Corticosteroids:
- Recommended as first-line salvage treatment (recommendation grade A) when medical management fails
- Achieves substantial long-term vertigo control in ~80% of refractory cases without significant hearing loss
- Dexamethasone (4 mg/mL or higher) is the preferred agent because it is better tolerated by middle ear tissues vs. methylprednisolone
- Methylprednisolone achieves higher perilymph/endolymph concentrations but no demonstrated superior clinical results
- First IT steroid protocol (Itoh & Sakata, 1987): 4-5 weekly injections of dexamethasone 2 mg - resulted in vertigo relief in 80%, tinnitus reduction in 74%
- Various protocols described (Table 158.2 in Cummings) including daily × 5 days, weekly × 4 weeks, on-demand
- Possible mechanism: besides anti-inflammatory effect, Na+/K+ channel modulation altering endolymph homeostasis
- No significant permanent hearing loss risk
Intratympanic Gentamicin (Chemical Labyrinthectomy / Partial Vestibulotoxic Ablation):
- Indicated when IT steroids fail, or in end-stage MD with drop attacks
- Gentamicin selectively destroys vestibular hair cells (vestibulotoxic), producing partial chemolabyrinthectomy
- Typical Ménière's vertigo attacks cease because the peripheral vestibular input is ablated
- Patient may develop some imbalance or visual-vestibular mismatch post-treatment (vestibular compensation required)
- Recommendation grade A evidence for vertigo control
- Sensorineural hearing loss is a significant risk (dose-dependent) - must be factored into patient counseling
- "As-needed" or titration protocols preferred over fixed-dose to minimize cochlear toxicity
- Not indicated in the only-hearing ear
Transtympanic Low-Pressure Therapy (Meniett Device):
- Delivers repetitive 0.6-second pulses of low pressure (0-20 cm H2O) via a ventilation tube
- Proposed mechanism: alters endolymphatic pressure via round window
- Requires a pre-existing or surgically placed grommet
- Some positive results but Cochrane analysis results were mixed
8. Surgical Management
Surgery is reserved for patients who fail aggressive medical management and continue to have disabling vertigo. The decision is based on the hearing level in the affected ear, hearing in the contralateral ear, patient age and general health.
8a. Endolymphatic Sac Surgery (Hearing-Preserving)
Endolymphatic Sac Decompression (ESD):
- The endolymphatic sac, located on the posterior surface of the temporal bone (Trautmann's triangle), is surgically decompressed by removing overlying bone via mastoidectomy
- Rationale: improves endolymph reabsorption by relieving pressure on the endolymphatic sac
Endolymphatic Sac Mastoid Shunting (Endolymphatic Sac-Subarachnoid/Mastoid Shunt):
- A silicone or Dacron wick/tube is placed from the endolymphatic sac into the mastoid cavity or subarachnoid space, theoretically providing a drainage pathway for excess endolymph
Outcomes (Sood et al. meta-analysis):
- ESD: vertigo control (Class A+B) of 79.3% at 12 months, 81.6% at 24 months
- Mastoid shunting: 76.4% at 12 months, 75.7% at 24 months
- Hearing preservation (within 10 dB of preoperative thresholds): ~71-73%
Evidence controversy: Cochrane analysis (Pullens et al., 2010/2013) found no beneficial effect over grommet insertion or mastoidectomy alone in RCTs. The natural history of MD (high spontaneous remission rate) complicates interpretation. Despite the lack of Level 1 evidence, ELS surgery is widely used given its safety profile and hearing preservation.
8b. Tenotomy of Tensor Tympani and Stapedial Muscle Tendons
- Sectioning the tensor tympani and/or stapedius tendons to relieve increased cochlear pressure transmitted via the ossicular chain
- Proposed mechanism: increased cochlear pressure pushes the tympanic membrane laterally against the ossicles; tenotomy alleviates this
- Conflicting evidence: positive results reported only by one centre; a randomized study of IT gentamicin with vs. without simultaneous tenotomy showed no statistically significant difference
8c. Selective Vestibular Nerve Section (Hearing-Preserving Destructive)
- Surgical section of the vestibular division of CN VIII while preserving the cochlear nerve and facial nerve
- Produces vestibular areflexia on the operated side; central compensation follows
- Approaches: retrosigmoid (posterior fossa), middle fossa, or retrolabyrinthine
- Indications: disabling vertigo with useful hearing in the affected ear, failure of medical and IT therapies
- Outcomes: vertigo control comparable to IT gentamicin in case-control studies, but with greater surgical morbidity
- Risks: CSF leak, meningitis, facial nerve injury, hearing loss, headache
- Rarely performed today given effectiveness of IT gentamicin
8d. Labyrinthectomy (Destructive, Non-Hearing Preserving)
- Surgical destruction of the entire membranous labyrinth (cochlear + vestibular)
- Definitively ablates all peripheral inner ear function on the affected side
- Indicated only when:
- Hearing in the affected ear is severely impaired (Stage 4, non-serviceable hearing)
- IT gentamicin has failed or is contraindicated
- The contralateral ear has serviceable hearing
- Approaches: transmastoid labyrinthectomy (most common) or transcanal
- Vertigo control: >95% - most definitive vestibular ablation procedure
- Permanent total deafness on the operated side is certain
- Vestibular rehabilitation required post-operatively for central compensation
Summary Algorithm for Surgical Decision-Making
Disabling MD, failed medical therapy
|
↓
IT Dexamethasone (Grade A)
|
Still failing?
↓
IT Gentamicin (Grade A) ←— Especially if drop attacks
|
Still failing?
↓
Hearing in affected ear?
| |
Yes No
| |
Endolymphatic Labyrinthectomy
Sac Surgery / (>95% vertigo control)
Vestibular Nerve
Section
9. Summary Table
| Feature | Details |
|---|---|
| Pathology | Endolymphatic hydrops (distension of membranous labyrinth) |
| Classic triad | Episodic vertigo + fluctuating SNHL + tinnitus (+/- fullness) |
| Duration of attack | 20 minutes to 12 hours (usually 2-3 hours) |
| Hearing loss | Low-frequency SNHL, fluctuating initially |
| Diagnosis (definite) | ≥2 vertigo attacks (20 min-12 h) + documented low-frequency SNHL + fluctuating aural symptoms |
| Key investigation | PTA, ECoG (SP/AP ratio), delayed Gd-MRI |
| ECoG cutoff | SP/AP >0.42 (extratympanic), >0.35 (transtympanic) |
| First-line treatment | Low sodium diet + betahistine + diuretics |
| IT salvage | IT dexamethasone (hearing-preserving), then IT gentamicin (ablative) |
| Surgery (hearing-preserving) | Endolymphatic sac decompression / shunt; vestibular nerve section |
| Surgery (destructive) | Labyrinthectomy (for non-serviceable hearing) |
| Natural history | Vertigo remits spontaneously in 71% by 8.3 years; hearing loss accumulates |
| Bilateral disease | ~19-24% of cases |
| Drop attacks (Tumarkin crises) | 2-6%, due to otolithic crisis; treat with IT gentamicin |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, 6th Ed. (Flint et al.), Chapters 158 & 167
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed., Vol. 2, Chapter 63
- K.J. Lee's Essential Otolaryngology, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.