External ear anatomy in detail and clinical also
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the key content and images needed for a comprehensive answer. Let me compile the full response.
External Ear - Detailed Anatomy and Clinical Correlations
Overview
The external ear has two parts:
- Auricle (pinna) - the visible cartilaginous projection on the side of the head
- External acoustic meatus (EAC) - the canal leading inward to the tympanic membrane
Part 1: The Auricle (Pinna)
Surface Anatomy
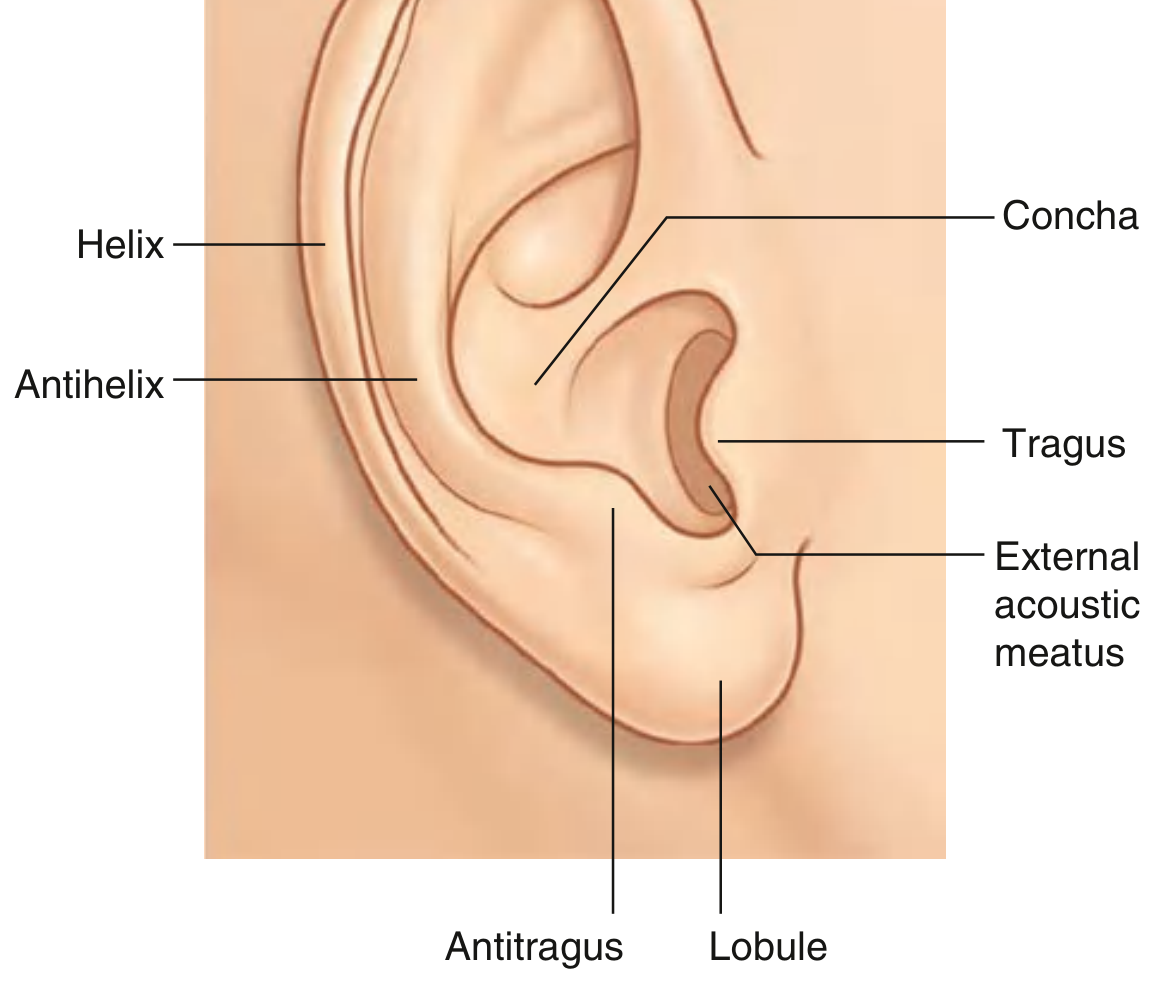
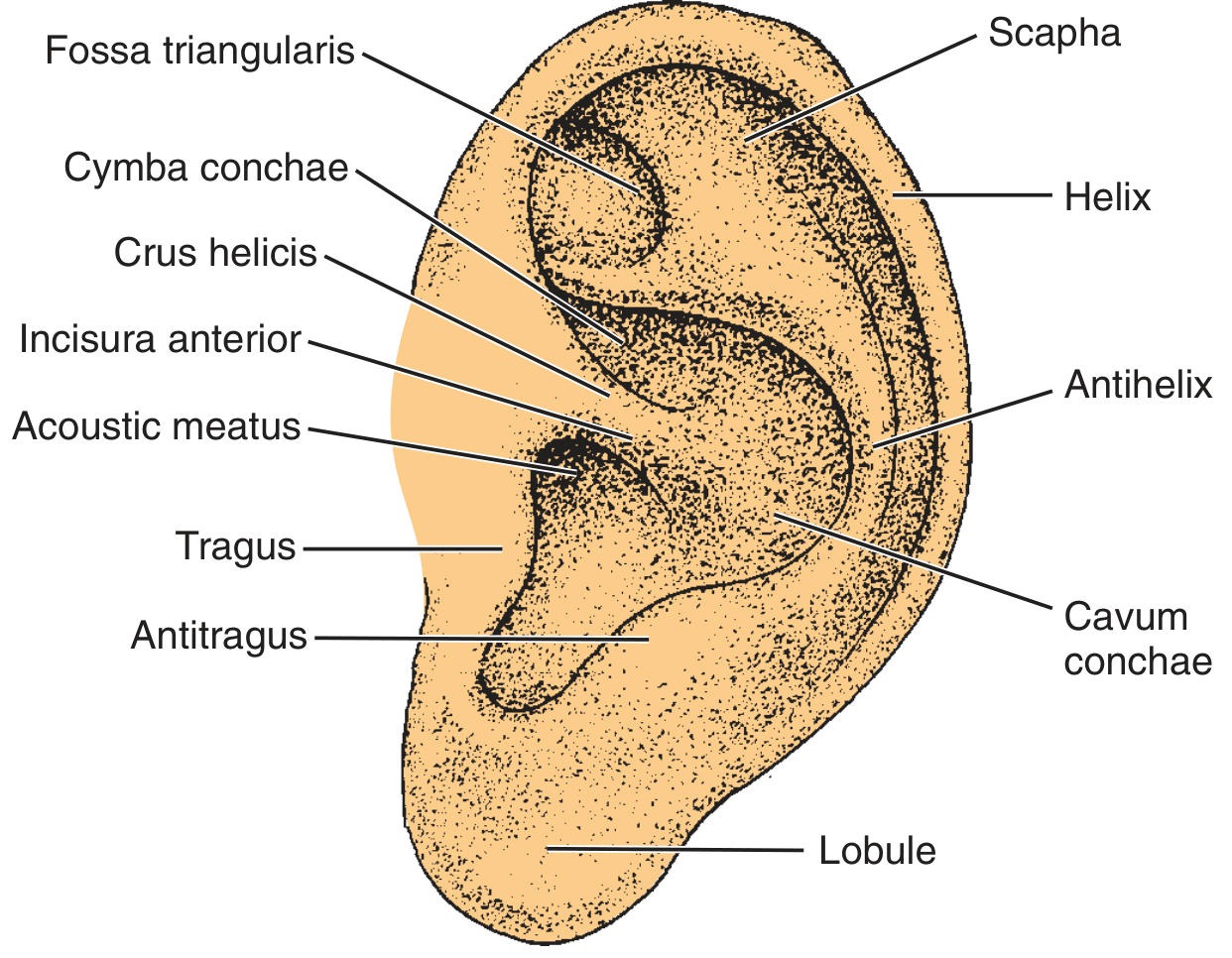
The auricle is a funnel-shaped cartilaginous structure covered with skin, forming intricate ridges and depressions. Key landmarks:
| Structure | Description |
|---|---|
| Helix | Large outer rim of the auricle; ends inferiorly at the lobule |
| Antihelix | Smaller curved rim, parallel and anterior to the helix; forms a Y-shape with two crura superiorly |
| Scapha | Groove between helix and antihelix |
| Concha | Hollow center of the auricle; divided into cymba conchae (superior) and cavum conchae (inferior) |
| Tragus | Elevation anterior to the EAC opening |
| Antitragus | Elevation opposite the tragus, above the lobule |
| Fossa triangularis | Depression between the two crura of the antihelix |
| Crus helicis | The root of the helix that traverses the concha |
| Incisura anterior | Notch between crus helicis and tragus |
| Lobule | The only part of the auricle not supported by cartilage (fibro-fatty tissue) |
Cartilage
The auricle consists of a single piece of elastic fibrocartilage (except the lobule). The cartilage is covered by perichondrium and skin on both surfaces. The skin is tightly adherent on the lateral surface but slightly more mobile on the medial (cranial) surface.
Part 2: External Acoustic Meatus (EAC)
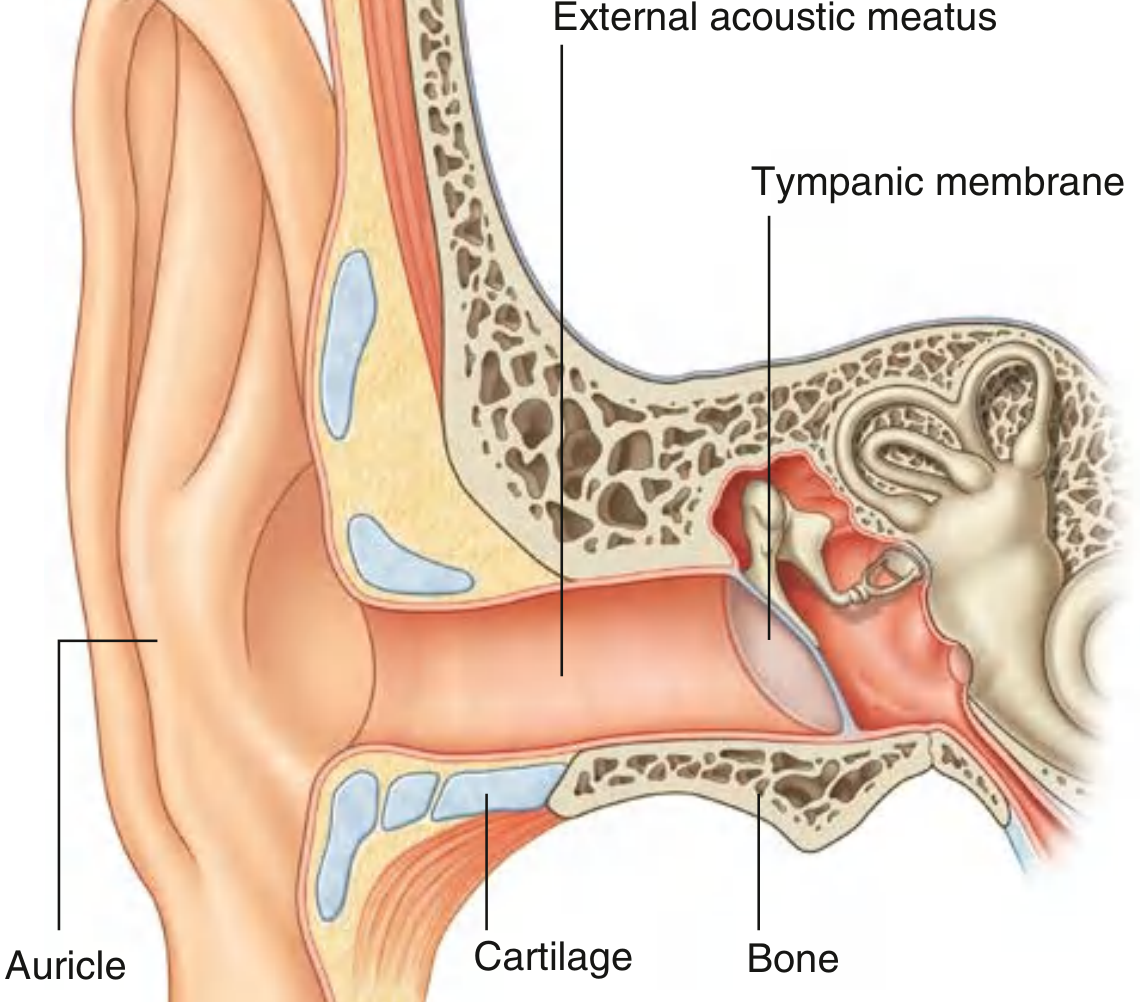
- Length: ~2.5 cm
- Lateral 1/3: Cartilaginous (membranous) portion
- Medial 2/3: Bony portion (within the temporal bone)
Skin Lining
| Portion | Skin Characteristics |
|---|---|
| Cartilaginous canal | Thick, mobile skin with sebaceous glands, apocrine (ceruminous) glands, and hair follicles |
| Bony canal | Thin, immobile skin; no hair or glands; continuous with tympanic membrane epithelium |
The sebaceous and apocrine ducts empty into a follicular canal around each hair follicle. Cerumen (earwax) is a mixture of the secretions of these glands.
Course of the EAC
The canal is not straight - it follows an S-shaped course:
- From the external opening: runs upward and anteriorly
- Then: turns slightly posteriorly, still passing upward
- Finally: turns again anteriorly with a slight descent
Clinical tip: To straighten the canal for otoscopy in an adult, pull the ear superiorly, posteriorly, and slightly laterally (in infants/young children, pull inferiorly and posteriorly).
Key Anatomical Points
- Isthmus: The bony-cartilaginous junction is the narrowest point of the EAC. It represents a potential pathway for spread of malignancy - hence en bloc resection is needed for EAC cancers.
- Foramen of Huschke: Incomplete ossification of the anterior bony canal wall creates this opening into the infratemporal region - a route for tumor spread to the deep lobe of the parotid.
- Fissures of Santorini: Natural defects in the cartilaginous portion - provide pathways for spread to the superficial parotid lobe and are the route through which P. aeruginosa in malignant otitis externa escapes to the skull base.
Part 3: Muscles
Intrinsic Muscles
Pass between cartilaginous parts of the auricle - may change its shape.
Extrinsic Muscles
| Muscle | Action |
|---|---|
| Anterior auricular | Pulls auricle anteriorly |
| Superior auricular | Elevates auricle |
| Posterior auricular | Pulls auricle posteriorly |
All auricular muscles are innervated by the facial nerve [VII]. These muscles are largely vestigial in humans.
Part 4: Neurovascular Supply
Arterial Supply
The blood supply originates from the external carotid artery:
- Posterior auricular artery (from external carotid) - main supply to posterior auricle
- Superficial temporal artery - anterior auricular branches
- Occipital artery - contributes a branch
Venous Drainage
Follows corresponding arteries.
Lymphatic Drainage
| Drainage Region | Nodes |
|---|---|
| Anterior auricular nodes | Lateral pinna and anterior canal wall |
| Postauricular (mastoid) nodes | Superior and posterior pinna, posterior canal wall |
| Superficial and deep cervical nodes | Lobule and floor of EAC |
Sensory Innervation of the Auricle
Supplied by multiple nerves - clinically important:
| Nerve | Area Supplied |
|---|---|
| Great auricular nerve (C2, C3 - cervical plexus) | Anterior and posterior inferior portions |
| Lesser occipital nerve (C2 - cervical plexus) | Posterosuperior portion |
| Auriculotemporal nerve (V3 - mandibular) | Anterosuperior portion |
| Auricular branch of vagus [X] | Deeper parts (concha, EAC posterior/inferior walls) |
| Facial nerve [VII] | Branch to auricular branch of vagus |
Sensory innervation of the EAC:
- Auriculotemporal nerve (V3): anterior and superior walls
- Auricular branch of vagus [X] (Arnold's nerve): posterior and inferior walls
Arnold's reflex: Stimulation of the posterior EAC (posterior/inferior wall - vagal territory) triggers cough reflex. Clinically seen when syringing ears or taking ear swabs.
Part 5: Embryology
The external ear develops from ectodermal and mesodermal components of the 1st and 2nd branchial arches and the intervening 1st branchial groove:
- Hillocks of His (6 condensations of tissue around the 1st branchial groove):
- 1st arch hillocks (1-3): tragus and most of the helix
- 2nd arch hillocks (4-6): antihelix, antitragus, lobule, and inferior helix
- EAC: develops from the dorsal portion of the 1st branchial cleft
- A transient meatal plug forms and later dissolves to leave a patent canal
Embryological errors:
- Failed involution of meatal plug → canal atresia or stenosis with conductive hearing loss and risk of canal cholesteatoma
- Imperfect hillock development → anotia, preauricular cysts, or sinuses
- Preauricular sinuses/cysts arise from duplication of the 1st branchial groove and arch
Part 6: Clinical Correlations
1. Otitis Externa (Swimmer's Ear)
The EAC's self-cleaning mechanism (epithelial migration from the umbo outward), cerumen's acidic pH (~6.1), and intact skin are the primary defenses.
Types of otitis externa (per Textbook of Family Medicine):
| Type | Organism | Features |
|---|---|---|
| Acute localized (furunculosis) | S. aureus | Pustule/furuncle in hair-bearing cartilaginous canal; itching, pain, swelling |
| Acute diffuse (swimmer's ear) | P. aeruginosa | Severe otalgia, discharge, diffuse erythema/edema; tragal tenderness |
| Erysipelas | Group A Strep | Diffuse red, painful ear; hemorrhagic bullae in canal |
| Chronic | Mixed / eczematous | Mild discomfort, flaking skin, long duration |
| Eczematous | Allergic/dermatitis | Scaling, crusting, oozing, severe itch |
| Malignant (necrotizing) | P. aeruginosa (Aspergillus in immunosuppressed) | See below |
Malignant (Necrotizing) Otitis Externa:
- Occurs in diabetics, immunocompromised (HIV, chemotherapy)
- P. aeruginosa penetrates through fissures of Santorini → temporal bone osteomyelitis → skull base → cranial nerve palsies (VII most common; IX, X, XII)
- Granulation tissue at bony-cartilaginous junction is pathognomonic
- Diagnosis: CT temporal bone or Technetium-99m bone scan; MRI with gadolinium
- Treatment: 6-8 weeks antipseudomonal antibiotics (ciprofloxacin + antipseudomonal 3rd gen cephalosporin); surgical debridement
2. Auricular Hematoma
- Blunt trauma shears perichondrium from cartilage → blood collects between them
- Untreated: fibroblast proliferation → cauliflower ear (wrestler's ear)
- Treatment: incision and drainage + through-and-through sutures + bolster dressing + systemic antibiotics (fluoroquinolones)
3. Auricular Lacerations
- Types: simple (with/without cartilage), stellate (blunt), partial or total avulsion
- Treatment: deep cleaning, debridement, surgical repair ± flap reconstruction, bolster to prevent hematoma
- Complication: perichondritis, cartilage necrosis
4. Perichondritis
- Infection of the perichondrium (cartilage's blood supply is entirely through perichondrium)
- Can lead to avascular necrosis of cartilage
- Common after ear piercing through the cartilage
- Organism: P. aeruginosa; treatment: fluoroquinolones
5. Frostbite
- Subfreezing exposure → endothelial disruption, platelet aggregation, sludging
- Treatment: slow warming, antibiotics, anticoagulants, debridement after demarcation; no pressure dressings
6. Keloids and Hypertrophic Scars
- Higher incidence in African American and Hispanic populations (up to 30%)
- Treatment: steroid injection, surgical excision, pressure dressing, rarely radiation
7. Carcinoma of the External Ear
- 6% of skin cancers involve the ear
- BCC and SCC are most common
- TNM staging (skin/pinna):
- T1: ≤2 cm
- T2: >2 cm but <5 cm
- T3: >5 cm
- T4: invades bone, muscle, cartilage
- Lymphatic spread follows depth of invasion
- EAC malignancy can spread via fissures of Santorini and foramen of Huschke to parotid and skull base
8. Congenital Anomalies
| Anomaly | Description |
|---|---|
| Microtia / Anotia | Underdevelopment or absence of auricle |
| Canal atresia | Failed meatal plug involution; conductive hearing loss |
| Preauricular pit/sinus | From duplicated 1st branchial groove; can become infected |
| Preauricular tags | Accessory hillocks of His |
| Low-set ears | Associated with chromosomal syndromes (Trisomy 18, 21) |
9. Referred Otalgia
Because the EAC receives sensory supply from CN V3, VII, X, and cervical plexus, pain can be referred to the ear from many distant sites:
- Teeth/TMJ (V3)
- Tonsil, pharynx, larynx (IX, X)
- Cervical spine (C2, C3 via great auricular/lesser occipital)
- In adults with otalgia and a normal exam: always examine the pharynx, larynx, and dentition to exclude malignancy
Sources: Gray's Anatomy for Students (p. 1094-1095); Cummings Otolaryngology Head and Neck Surgery (Ch. 126); K.J. Lee's Essential Otolaryngology (Ch. 23); Textbook of Family Medicine 9e (p. 267)
This is a shared conversation. Sign in to Orris to start your own chat.