CSF analysis and lumber puncture procedure explain from standard medicine book
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile the full response.
Lumbar Puncture (LP) and CSF Analysis
Sources: Pfenninger & Fowler's Procedures for Primary Care (3rd ed.), Harrison's Principles of Internal Medicine (22nd ed., 2025), Roberts & Hedges' Clinical Procedures in Emergency Medicine, Quick Compendium of Clinical Pathology (5th ed.), Textbook of Family Medicine (9th ed.), Tietz Textbook of Laboratory Medicine (7th ed.)
1. LUMBAR PUNCTURE
Definition
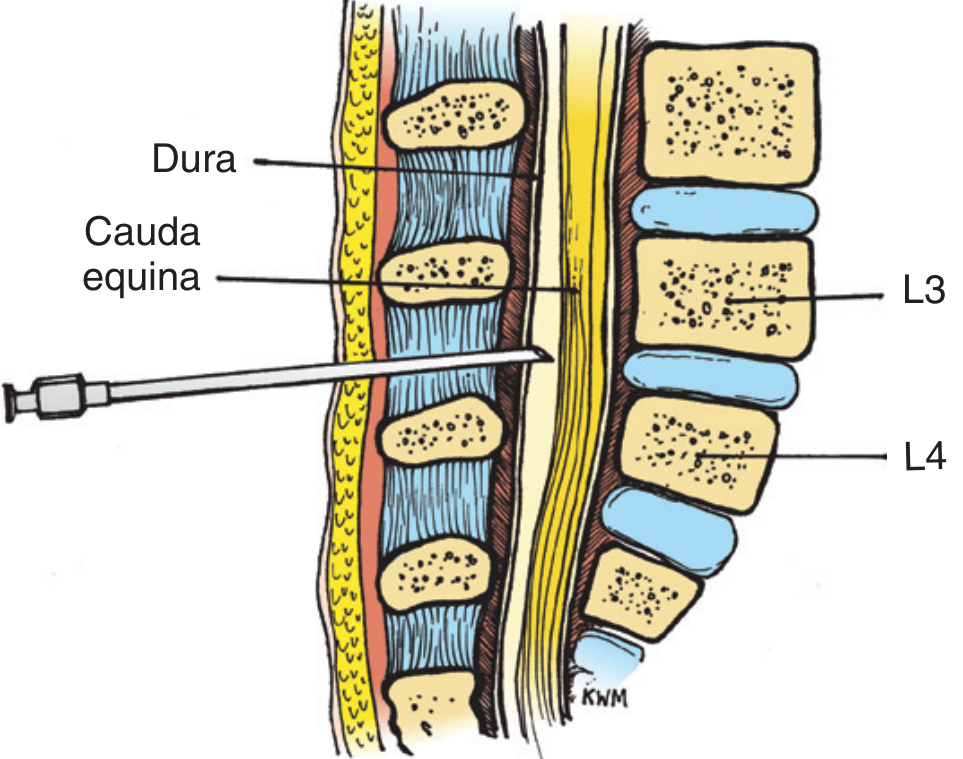
Lumbar puncture (LP) is a procedure in which a spinal needle is inserted into the subarachnoid space at the lumbar level under local anesthesia to withdraw CSF for diagnostic or therapeutic purposes. The spinal cord ends at approximately L1-L2 in adults, so the needle is inserted safely below this level - at L3-L4 or L4-L5 - where only the cauda equina floats freely and the risk of cord injury is minimal.
- Tietz Textbook of Laboratory Medicine, 7th Ed.
Indications
Urgent/emergent:
- Suspected CNS infection (bacterial/viral/fungal/TB meningitis, encephalitis)
- Suspected subarachnoid hemorrhage (SAH) with negative CT
Non-urgent/elective:
-
Dementia workup (when normal-pressure hydrocephalus, syphilis, vasculitis suspected)
-
Unexplained neurologic disorders (altered consciousness, polyneuropathy, seizures)
-
Multiple sclerosis workup (oligoclonal bands)
-
Meningeal carcinomatosis / lymphomatous meningitis
-
Intrathecal drug administration (antibiotics, chemotherapy, anesthesia)
-
Imaging procedures (myelography, cisternography)
-
Pseudotumor cerebri - both diagnosis and therapeutic drainage
-
Pfenninger & Fowler's Procedures for Primary Care, p. 1438
Contraindications
| Type | Condition |
|---|---|
| Absolute | Local skin infection at the puncture site |
| Absolute | Raised intracranial pressure with papilledema (risk of herniation) |
| Absolute | Supratentorial mass with midline shift or obliterated cisterns on CT |
| Relative | Severe coagulopathy or platelet count <20,000/mm³ |
| Relative | Anticoagulated patient (INR >1.4) |
| Relative | Uncooperative patient / hemodynamically unstable |
Key note: The absence of papilledema is NOT always reassuring - papilledema may take >48 hours to develop and is absent in up to 15% of adults and 50% of children with early raised ICP. Always check for clinical risk factors (Box 206-1 criteria include: age ≥60, altered level of consciousness, focal neurologic deficits, seizure within 1 week, immunocompromised state, history of CNS disease).
- Pfenninger & Fowler's Procedures for Primary Care, pp. 1438-1439
Equipment
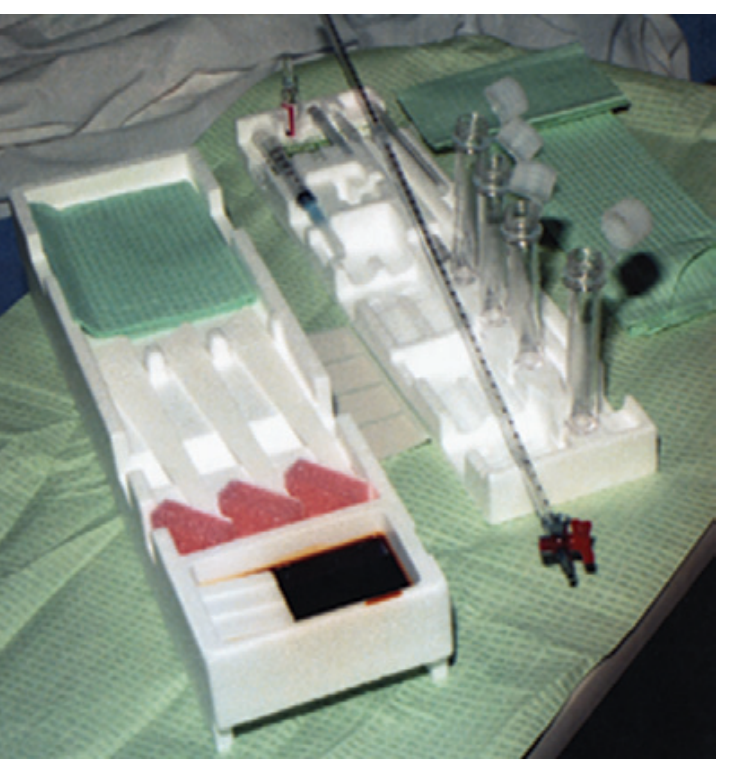
Figure: Lumbar puncture equipment tray (Pfenninger & Fowler)
Standard LP tray includes:
-
Povidone-iodine swabs and alcohol swabs
-
Fenestrated drape and sterile gloves
-
Manometer with three-way stopcock (to measure opening pressure)
-
1% lidocaine in a 3-mL syringe; 25-27 gauge skin needle for local anesthesia
-
20-22 gauge spinal needle (Quincke with beveled tip) - standard choice. A 24-27 gauge atraumatic needle reduces post-LP headache but cannot measure opening pressure reliably
-
Four numbered, capped sterile test tubes
-
Sterile dressing
-
Pfenninger & Fowler's Procedures for Primary Care, p. 1439
Patient Positioning
Lateral decubitus (fetal/embryo position): Patient lies on their side at the edge of the bed, knees drawn up to the abdomen, neck slightly flexed. Shoulders and pelvis must be exactly perpendicular to the bed (no forward or backward tilt). This is the preferred position when measuring opening pressure.
Seated upright position: Patient sits and leans forward. Easier to identify the midline in obese patients, but cannot measure accurate opening pressure. Most commonly used in adults.
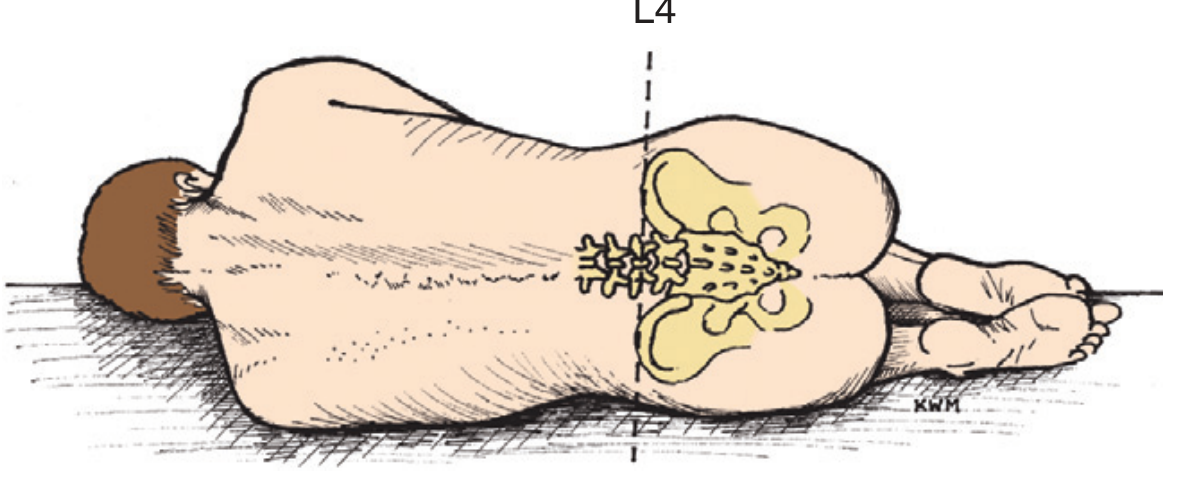
Figure: Lateral decubitus position with L4 anatomic landmark
Anatomic Landmark Identification
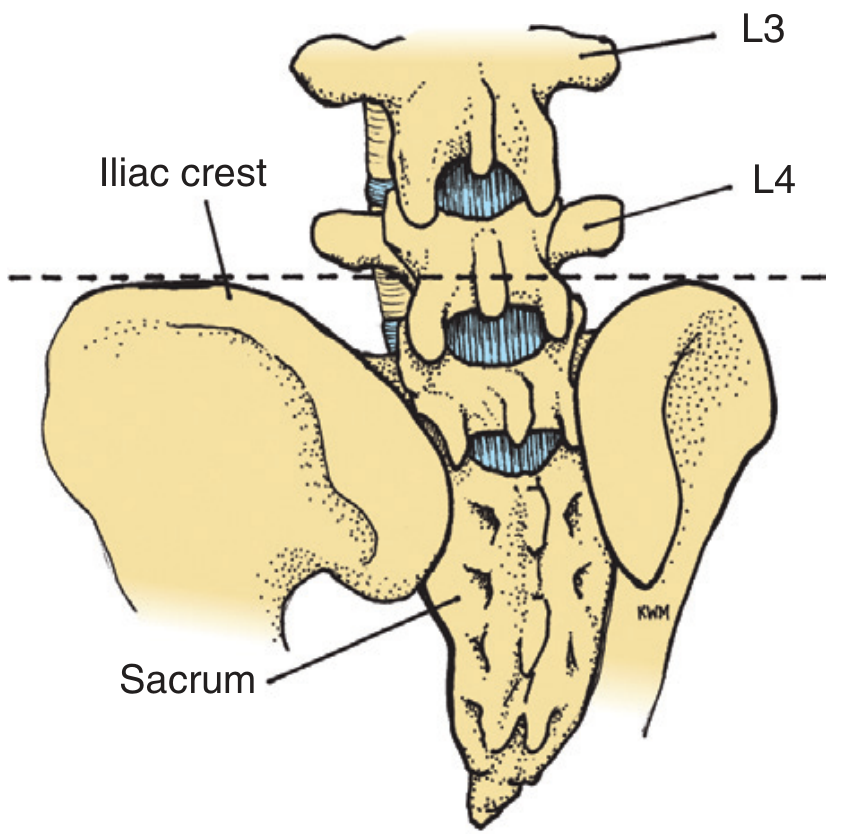
Figure: A horizontal line connecting the superior aspects of the iliac crests (Tuffier's line) intersects the body of L4 - use this to identify the L3-L4 interspace
The L3-L4 interspace is the primary entry point. The L2-L3 or L4-L5 interspaces may also be used if needed.
Step-by-Step Technique (Midline Approach)
Step 1 - Pre-procedure safety check:
Patients with focal neurologic deficits, altered mentation, immunocompromise, papilledema, or suspected SAH should have CT imaging first. However, if bacterial meningitis is suspected, do NOT delay antibiotics waiting for CT.
Step 2 - Positioning:
Place the patient in lateral decubitus or seated position at the edge of the bed. The patient should "roll up into a ball" to open the interspinous spaces. Maintain strict alignment of shoulders, back, and pelvis.
Step 3 - Set up sterile field:
Open the spinal tray aseptically. Put on sterile gloves. Pre-assemble the manometer by joining its two pieces and inserting it into the vertical port of the three-way stopcock. Open and upright the four numbered test tubes in order.
Step 4 - Skin preparation and draping:
Clean the selected interspace plus one above and below with povidone-iodine in a circular motion (at least 10 cm diameter). Apply the fenestrated drape.
Step 5 - Local anesthesia:
Draw 3 mL of 1% lidocaine. Raise a skin wheal at the L3-L4 midline interspace with a 25-27 gauge needle. Inject deeper into the posterior spinous region along the direction the spinal needle will travel.
Step 6 - Needle insertion:
Insert the 20-22 gauge spinal needle through the skin in the midline, angled approximately 15 degrees cephalad toward the umbilicus. Keep the bevel of the needle parallel to the longitudinal axis of the spine (bevel turned up/down in lateral decubitus; turned sideways when seated) - this spreads rather than cuts the longitudinal dural fibers and reduces post-LP headache.
The needle passes through:
- Skin and subcutaneous tissue
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum
- Epidural space
- Dura mater and arachnoid
- Subarachnoid space (target - CSF flows freely)
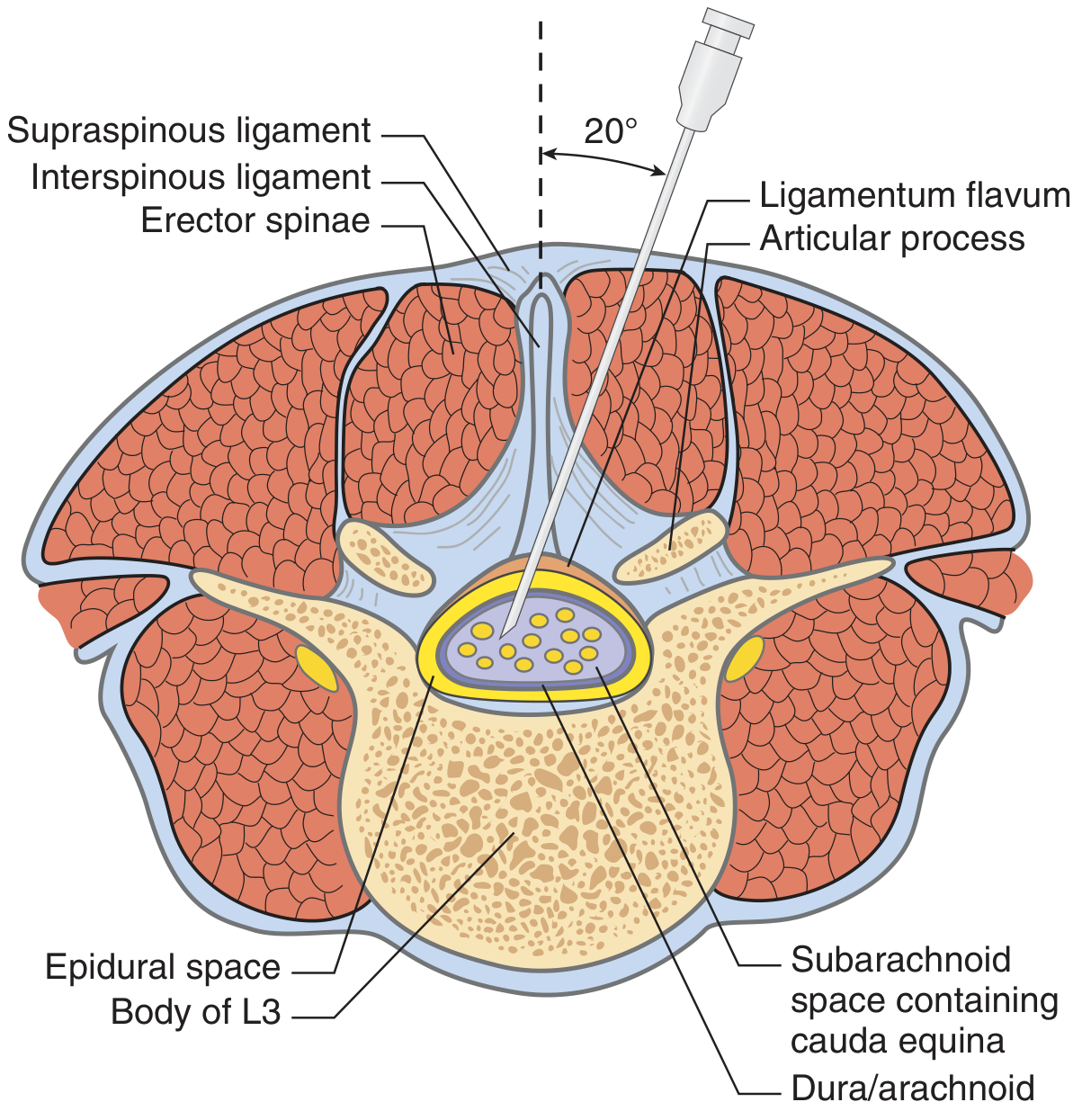
Figure: Lateral approach cross-section at L3 showing layers traversed, cauda equina in the subarachnoid space, and the 20-degree angle of entry (Pfenninger & Fowler)
A "give" or "pop" is felt as the needle penetrates the ligamentum flavum, and again as it pierces the dura-arachnoid. If bone is encountered, withdraw slightly and redirect more cephalad.
Step 7 - Measure opening pressure:
Remove the stylet. Attach the manometer via the three-way stopcock as CSF flows in. Record the opening pressure in mm H₂O. Normal adult range: 70-180 mm H₂O.
Step 8 - CSF collection:
Turn the stopcock to allow CSF to flow into the numbered test tubes. Collect 2-3 mL per tube (at least 4 tubes). Label tubes in the order collected.
- If the fluid is bloody and does not clear by the 3rd tube: this suggests true SAH (traumatic tap clears progressively)
- Replace the stylet before removing the needle (reduces post-LP headache risk)
Step 9 - Needle removal and dressing:
Once sufficient CSF is obtained, replace the stylet, withdraw the needle, and apply a sterile dressing.
Step 10 - Post-procedure:
Have the patient lie flat for 1-4 hours (reduces post-LP headache, though evidence is mixed).
Lateral Approach (Alternative)
Used when the midline approach fails or in elderly patients with calcified interspinous ligaments. Insert the needle 1.5-2 cm lateral to the midline, directed 20 degrees toward midline and 15 degrees cephalad. This bypasses the calcified midline ligaments.
- Pfenninger & Fowler's Procedures for Primary Care, pp. 1439-1441
Tube Order and Tests Sent
| Tube | Test |
|---|---|
| Tube 1 | Bacteriology: Gram stain, acid-fast stain*, culture (bacteria, fungal*, TB*, viral*) |
| Tube 2 | Biochemistry: glucose, protein, protein electrophoresis* |
| Tube 3 | Hematology: cell count, differential |
| Tube 4 (optional) | VDRL*, India ink*, cryptococcal antigen*, cytology*, oligoclonal bands*, myelin basic protein*, PCR studies |
If clinically indicated.
Practical tip: Tube 1 is most likely contaminated with blood from needle insertion. Use Tube 3 for the definitive cell count. For traumatic tap assessment, compare RBC count in Tube 1 vs. Tube 4 - a decreasing count favors traumatic tap. Correction factor: for every 700 RBCs, CSF leukocytes increase by 1 and CSF protein rises by 1 mg/dL.
- Pfenninger & Fowler's Procedures for Primary Care, p. 1441
2. CSF ANALYSIS
Normal CSF Values
| Parameter | Neonate | Infant | Child | Adult |
|---|---|---|---|---|
| Opening pressure (mm H₂O) | - | 50-80 | 50-80 | 70-180 |
| WBC count (/mm³) | 8 (0-22) | - | <7 | <5 |
| Neutrophils | 61% | - | None | None |
| Glucose (mg/dL) | 34-119 mg/dL | - | 40-80 | 50-80 |
| CSF:serum glucose ratio | 44-128% | - | ~50% | 60-70% |
| Protein (mg/dL) | 20-170 (mean 90) | - | 5-40 | 15-45 |
- Pfenninger & Fowler's Procedures for Primary Care, p. 1440
Opening Pressure
- Normal: 70-180 mm H₂O in adults (lateral decubitus; higher in seated position)
- Elevated (>250 mm H₂O): suggests meningitis, SAH, intracranial mass, pseudotumor cerebri, or venous sinus thrombosis
- Reduced: suggests CSF leak, dehydration, or spinal block below the tap level
Appearance / Color
| Appearance | Interpretation |
|---|---|
| Clear and colorless | Normal |
| Turbid / cloudy | Cell count >200 WBC/mm³ or >400 RBC/mm³ - suggests infection |
| Bloody (tube 1 → clears by tube 3-4) | Traumatic tap |
| Uniformly bloody (all tubes) | True SAH |
| Pink xanthochromia | Free hemoglobin - suggests SAH |
| Yellow xanthochromia | Bilirubin from hemoglobin metabolism - begins ~12 hrs after hemorrhage, peaks at 72 hrs, disappears in 2-4 weeks |
| Artifactual xanthochromia | Hyperbilirubinemia, CSF protein >150 mg/dL, carotenoids, rifampin, delay >1 hour before analysis |
Xanthochromia and erythrophagocytosis (or hemosiderin-laden macrophages) confirm true subarachnoid blood vs. traumatic tap.
- Quick Compendium of Clinical Pathology, 5th ed.; Tintinalli's Emergency Medicine
Glucose
- Normal CSF glucose = ~60-70% of serum glucose (always check a simultaneous serum glucose)
- Hypoglycorrhachia (CSF glucose <40 mg/dL, or CSF:serum ratio <30%): bacterial meningitis, TB meningitis, fungal meningitis, carcinomatous meningitis, hypoglycemia
- Normal glucose: viral meningitis, early bacterial meningitis, brain abscess
Protein
- Normal adult: 15-45 mg/dL
- Elevated protein: infection (bacterial > viral), MS, Guillain-Barré syndrome, brain tumor, SAH, hypothyroidism, diabetes, spinal cord compression
- Very high protein (Froin's syndrome - >500 mg/dL, yellowish, clots spontaneously): spinal block
- CSF:serum albumin ratio <1:230 when blood-brain barrier is intact
- CSF glutamine is elevated in hepatic encephalopathy
Cell Count and Differential (Pleocytosis)
| Cell type predominance | Causes |
|---|---|
| PMN (neutrophils) | Bacterial meningitis (early), early TB/fungal meningitis, chemical meningitis |
| Lymphocytes/monocytes | Viral meningitis, TB meningitis, fungal meningitis (chronic), MS, sarcoidosis, syphilis |
| Eosinophils | Parasitic infections (angiostrongyliasis, gnathostomiasis, cysticercosis), fungal meningitis (coccidioidal - 6-20% eos), lymphoma, sarcoidosis |
- Harrison's Principles of Internal Medicine, 22nd Ed.
Comparison of CSF Findings in Meningitis
| Parameter | Bacterial Meningitis | Viral Meningitis | TB/Fungal |
|---|---|---|---|
| Opening pressure | >180 mm H₂O | Often normal or elevated | Elevated |
| WBC count (/mm³) | 1,000-10,000 (median 1,195) | <300 (median 100) | 100-500 |
| Cell type | Neutrophils >80% | Lymphocytes >80% | Lymphocytes |
| Glucose (mg/dL) | <40 | >40 (normal) | Low |
| Protein (mg/dL) | 100-500 | Normal to mildly elevated | Elevated |
| Gram stain | Positive 60-90% | Negative | Negative |
| Culture | Positive 70-85% | Positive ~50% (viral PCR better) | Low yield |
- Textbook of Family Medicine, 9th Ed., p. 1233
Special CSF Tests
| Test | Indication/Significance |
|---|---|
| India ink preparation | Cryptococcal meningitis (visualizes capsule) |
| Cryptococcal antigen | More sensitive than India ink for Cryptococcus |
| VDRL | Neurosyphilis (highly specific, ~70% sensitive; negative does not exclude) |
| Oligoclonal bands | Multiple sclerosis (intrathecal IgG synthesis); also seen in CNS infections |
| Myelin basic protein | Active myelin destruction (MS, CNS injury) |
| Cytology / flow cytometry | Malignant cells in leptomeningeal carcinomatosis or lymphoma |
| PCR (16S rRNA) | Broad bacterial detection; useful in partially treated meningitis |
| 18S/28S rRNA PCR | Broad fungal detection |
| Beta-glucan assay | Fungal meningitis when other tests negative |
| Metagenomic NGS | Challenging infectious cases; unbiased pathogen detection |
| CSF beta-2 transferrin | CSF leak detection (rhinorrhea/otorrhea) |
| CSF glutamine | Hepatic encephalopathy |
- Harrison's Principles of Internal Medicine, 22nd Ed.
3. COMPLICATIONS
| Complication | Details |
|---|---|
| Post-LP headache | Most common (10-25%); positional (worse sitting, better lying); 90% within 48 hrs, may last up to 2 weeks. Treat with oral caffeine 300 mg or theophylline 200 mg; IV caffeine benzoate 500 mg for refractory cases; epidural blood patch (15 mL autologous blood) if no relief at 24 hrs - 85% immediate relief, 98% after 2nd patch |
| Traumatic/bloody tap | Inadvertent puncture of spinal venous plexus; self-limiting in most; risk of spinal hematoma in coagulopathy |
| Spinal epidural hematoma (SEH) | Rare but catastrophic; risk increased with anticoagulants, traumatic LP, concurrent aspirin + heparin. Diagnose with emergency MRI; treat with urgent laminectomy |
| Brain herniation | Occurs if LP done with unrecognized raised ICP and mass lesion; always check fundi for papilledema; obtain CT if any risk factors present |
| Intracranial subdural hematoma | Due to downward brain displacement from persistent CSF leak; tearing of bridging veins |
| Epidermoid tumor | Late complication when LP done without stylet (implanted dermal cells) |
| Infection | <0.01% risk; meningitis or epidural abscess |
| Seizures | Rare; reported with post-LP headache |
Reducing post-LP headache:
-
Use a 24-27 gauge atraumatic (pencil-point/Whitacre) needle
-
Use the smallest gauge that allows adequate flow
-
Orient the bevel parallel to the longitudinal axis of the spine
-
Replace the stylet before removing the needle
-
Use a 22-gauge in practice (balance between headache risk and technical success)
-
Pfenninger & Fowler's Procedures for Primary Care, pp. 1441-1442; Roberts & Hedges' Clinical Procedures in Emergency Medicine
4. ANTICOAGULATION AND LP
| Drug | Recommendation |
|---|---|
| Aspirin / NSAIDs alone | Generally safe without stopping (unless combined with heparin or another antiplatelet) |
| Clopidogrel / ticlopidine | Stop 7-10 days before (ASRA/AHA guideline) |
| Abciximab | Stop 24-48 hours before |
| Tirofiban / eptifibatide | Stop 8 hours before |
| IV heparin | Stop; 2% risk of SEH if LP done while on heparin; wait 4 hours after stopping |
| LMWH | Follow ASRA guidelines |
| Warfarin | INR must be ≤1.4 before LP |
If LP must be performed on anticoagulated patients: most experienced operator, smallest needle available, and monitor closely for SEH.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine; Pfenninger & Fowler's Procedures for Primary Care
Clinical pearl: In suspected bacterial meningitis, never delay empiric antibiotics while waiting for CT or LP. Blood cultures + immediate antibiotics, then LP as soon as safely possible. In suspected SAH with negative CT, LP is essential - xanthochromia (yellow tint of centrifuged CSF) confirms the diagnosis and takes at least 12 hours to develop after hemorrhage, so LP should ideally be done ≥12 hours after headache onset.
CSF analysis and lumber puncture procedure explain from standard medicine book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, multi-source textbook content. Let me compile the full detailed response.
Lumbar Puncture (LP) and CSF Analysis
Sources: Pfenninger & Fowler's Procedures for Primary Care (3rd ed.) | Henry's Clinical Diagnosis and Management by Laboratory Methods (23rd ed.) | Tietz Textbook of Laboratory Medicine (7th ed.) | Harrison's Principles of Internal Medicine (22nd ed., 2025) | Quick Compendium of Clinical Pathology (5th ed.)
PART 1 - LUMBAR PUNCTURE
Anatomy and Rationale
The spinal cord ends at approximately L1-L2 in adults. Below this level, only the cauda equina (a bundle of nerve roots) floats freely in the subarachnoid space, making the lumbar region safe for needle insertion. The needle enters the subarachnoid space between L3-L4 (most common), L2-L3, or L4-L5.
CSF physiology (Henry's Clinical Diagnosis, 23rd ed.):
- ~500 mL produced per day (0.3-0.4 mL/min); total volume 90-150 mL in adults
- ~70% derived from choroid plexuses; remainder from ventricular ependymal lining
- Total CSF volume replaced every 5-7 hours
- Reabsorbed at arachnoid villi along the superior sagittal sinus
- Functions: buoyancy (1500g brain weighs ~50g in CSF), shock absorption, CNS waste excretion, ionic homeostasis, transport of hypothalamic factors
Indications
Urgent indications:
- Suspected CNS infection: bacterial/viral/fungal/TB meningitis, encephalitis
- Suspected subarachnoid hemorrhage (SAH) after negative CT
Non-urgent indications:
- Dementia workup (normal-pressure hydrocephalus, neurosyphilis, vasculitis)
- Unexplained neurologic disorders: altered consciousness, polyneuropathy, seizures
- Multiple sclerosis workup (oligoclonal bands, IgG index)
- Meningeal carcinomatosis / lymphomatous meningitis
- Intrathecal drug delivery (chemotherapy, antibiotics, anesthesia)
- Myelography, cisternography (contrast instillation)
- Pseudotumor cerebri (diagnosis and therapeutic drainage)
- Pfenninger & Fowler's Procedures for Primary Care, p. 1437
Contraindications
| Type | Condition |
|---|---|
| Absolute | Local skin infection at the puncture site |
| Absolute | Raised ICP with papilledema - risk of transtentorial herniation |
| Absolute | Supratentorial mass with midline shift, obliterated cisterns, or posterior fossa mass on CT |
| Relative | Platelet count <20,000/mm³ or rapidly dropping; INR >1.4 |
| Relative | Hemodynamically unstable patient (shock, status asthmaticus) |
| Relative | Uncooperative patient |
Important note: Absence of papilledema does NOT exclude raised ICP - papilledema may take >48 hours to develop and is absent in up to 15% of adults and 50% of children with early raised ICP. Always assess clinical risk factors:
Box 206-1 - Clinical Risk Factors for Intracranial Pathology (do CT first):
- Age ≥60 years
- Altered level of consciousness
- History of CNS disease
- Immunocompromised state
- Seizure within 1 week of presentation
- Focal neurologic deficits (arm/leg drift, facial palsy, gaze palsy, visual field abnormality)
- Abnormal language; inability to answer 2 questions or follow 2 commands
Critical pearl: In suspected bacterial meningitis, never delay antibiotics while awaiting CT. Give empiric antibiotics after blood cultures, then perform LP as soon as safely possible.
- Pfenninger & Fowler's Procedures for Primary Care, pp. 1438-1439
Equipment
Standard LP tray contains:
- Povidone-iodine swabs + alcohol swabs
- Fenestrated sterile drape + sterile gloves
- Manometer + three-way stopcock (to measure opening pressure)
- 3 mL syringe with 1% lidocaine; 25-27 gauge skin needle for local anesthesia; 20-23 gauge needle to draw up anesthetic
- 20-22 gauge spinal needle (Quincke) - standard. 24-27 gauge atraumatic (Whitacre/pencil-point) reduces post-LP headache but cannot reliably measure opening pressure
- Four numbered sterile capped test tubes
- Sterile dressing
- Optional: EMLA cream (apply 30-60 min before), 1 mL syringe for gentle suction if CSF not flowing, ultrasound for obese patients
- Pfenninger & Fowler's Procedures for Primary Care, p. 1439
Patient Positioning
Lateral decubitus (preferred for opening pressure measurement):
Patient lies on their side at the edge of the bed, knees drawn to the abdomen, neck slightly flexed. Shoulders and pelvis must be strictly perpendicular to the bed - any forward/backward tilt rotates the spine and makes needle insertion difficult.
Seated upright position: Patient sits and leans slightly forward. Easiest for landmark identification in obese patients. Cannot give accurate opening pressure. Most commonly used in practice.
Anatomic Landmark Identification
Key surface landmark (Tuffier's line): A line connecting the tops of both iliac crests crosses the body of L4. The L3-L4 interspace is just above this line. Mark with a pen or gentle skin indentation.
Step-by-Step Procedure (Midline Approach)
Step 1 - Pre-procedure assessment:
Consider CT imaging first if any clinical risk factors for raised ICP are present (Box 206-1 above).
Step 2 - Consent and positioning:
Explain procedure, risks, and alternatives. Obtain informed consent. Position the patient (lateral decubitus preferred). A nurse or assistant should help maintain the patient's position.
Step 3 - Sterile setup:
Open the LP tray aseptically. Don sterile gloves. Preassemble the manometer (two pieces slide together); attach to the three-way stopcock. Stand the four numbered test tubes upright in their tray slots.
Step 4 - Skin preparation:
Swab the selected interspace plus one above and below with povidone-iodine in a widening circular motion (minimum 10 cm diameter). Apply fenestrated drape over the area.
Step 5 - Local anesthesia:
Draw up 3 mL of 1% lidocaine. Raise a skin wheal at the L3-L4 midline with a 25-27 gauge needle. Infiltrate deeper along the path the spinal needle will follow (into the interspinous ligament region).
Step 6 - Needle insertion:
Insert the spinal needle through the skin in the midline, angled ~15 degrees cephalad (toward the umbilicus), maintaining the needle in the sagittal midplane.
Critical technique point: Orient the bevel parallel to the longitudinal axis of the spine (bevel pointing up or down in lateral decubitus; pointing sideways when seated). This spreads - rather than cuts - the longitudinal dural fibers, significantly reducing post-LP headache.
The needle passes through these layers in sequence:
- Skin and subcutaneous fat
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum (a definite "give" or resistance change is felt here)
- Epidural space (fat, veins)
- Dura mater + arachnoid (second "pop" may be felt)
- Subarachnoid space - target
After advancing 3-4 cm, stop and withdraw the stylet to check for CSF flow. If no flow, replace stylet and advance a few mm more. If bone is hit, withdraw slightly and redirect more cephalad. Rotating the needle 90-180 degrees can help if flow is minimal. Dry tap is more often due to malposition than obliterated space - reposition the patient or try a different interspace.
Step 7 - Measure opening pressure:
Once CSF flows, anchor the needle hub firmly against the patient's back. Attach the stopcock-manometer assembly. Ask the patient to relax and extend the legs slightly (flexed neck/legs artificially elevate pressure). CSF rises in the manometer - read the opening pressure (in mm H₂O). Normal adult range: 70-180 mm H₂O (Henry's: 90-180 mm H₂O in lateral decubitus).
If opening pressure is >200 mm H₂O in a relaxed patient, withdraw no more than 2.0 mL.
Step 8 - Collect CSF:
Turn the stopcock to allow CSF to flow into the numbered test tubes (2-3 mL per tube). Collect at least 3-4 tubes. Note: if the fluid is bloody and does not clear from Tube 1 to Tube 3, this suggests true SAH rather than traumatic tap.
Tube allocation:
| Tube | Contents |
|---|---|
| Tube 1 | Bacteriology: Gram stain, acid-fast stain, culture (bacteria, fungal, TB, viral) |
| Tube 2 | Biochemistry: glucose, protein, protein electrophoresis |
| Tube 3 | Hematology: cell count, differential (use this for definitive cell count, not Tube 1) |
| Tube 4 | Optional: VDRL, India ink, cryptococcal antigen, cytology, oligoclonal bands, myelin basic protein, PCR |
Note from Henry's: Tube 1 should never be used for microbiology (skin contamination risk), and if Tube 1 is hemorrhagic from a traumatic tap, it should not be used for protein studies (e.g., suspected MS). Tube 3 should be examined for the primary purpose of CSF collection. Process specimens immediately - cellular degradation begins within 1 hour. Do NOT refrigerate culture specimens (Haemophilus, Neisseria are fastidious).
Step 9 - Therapeutic LP (if indicated):
For pseudotumor cerebri: remove CSF until closing pressure reaches ≤100 mm H₂O (typically 25-35 mL). For suspected normal-pressure hydrocephalus: removal of 35-50 mL may cause transient improvement in gait or cognition (diagnostic).
Step 10 - Needle removal:
Replace the stylet before withdrawing the needle (this reduces risk of post-LP headache). Apply sterile dressing.
Lateral Approach (Alternative)
Used when midline approach fails or calcified ligaments prevent entry (elderly patients). Insert needle 1.5-2 cm lateral to midline, directed 20 degrees toward midline and 15 degrees cephalad. This bypasses the ossified supraspinous and intraspinous ligaments.
Complications
| Complication | Details |
|---|---|
| Post-LP headache | Most common (10-25%); positional - worse upright, better supine; 90% onset within 48 hrs (may appear up to 14 days later); may be debilitating |
| Traumatic/bloody tap | ~20% of LPs; inadvertent puncture of epidural venous plexus; self-limiting |
| Spinal epidural hematoma (SEH) | Rare but catastrophic; highest risk with anticoagulants + traumatic LP; presents as back pain then paraplegia; diagnose with emergency MRI; treat with urgent laminectomy |
| Brain herniation | Occurs when LP is done with unrecognized mass lesion or raised ICP; check fundi for papilledema before every LP |
| Intracranial subdural hematoma | Rare; from downward brain displacement due to persistent CSF leak - tearing of bridging veins |
| Epidermoid tumor | Late risk when LP done without a stylet (implanted dermal cells) - especially in neonates |
| Infection (meningitis/abscess) | <0.01% risk |
Treatment of post-LP headache:
- First-line: bed rest, oral hydration, analgesics
- Oral caffeine 300 mg or theophylline 200 mg
- IV caffeine benzoate 500 mg over a few minutes (repeat in 1 hour for 85% relief rate)
- Epidural blood patch (if no relief at 24 hours): inject 15 mL autologous blood into the epidural space - provides immediate relief in 85%; after 2nd patch, 98% relief
Minimizing post-LP headache:
- Use a 24-27 gauge atraumatic (Whitacre/pencil-point) needle when opening pressure measurement is not critical
- In practice, 22-gauge Quincke is used for balance of success rate and headache risk
- Keep bevel parallel to the long axis of the spine
- Replace the stylet before needle withdrawal
- Pfenninger & Fowler's Procedures for Primary Care, pp. 1441-1442
PART 2 - CSF ANALYSIS
Opening Pressure
| Age Group | Normal Range |
|---|---|
| Infants | 10-100 mm H₂O |
| Children | 50-80 mm H₂O |
| Adults | 70-180 mm H₂O (some sources 90-180) |
| Obese adults | May be up to 250 mm H₂O (normal for them) |
- >250 mm H₂O = intracranial hypertension (meningitis, hemorrhage, tumor, pseudotumor, venous sinus thrombosis)
- Cryptococcal meningitis and pseudotumor cerebri may show elevated pressure as the only CSF abnormality
- Low pressure: spinal-subarachnoid block, dehydration, CSF leak, circulatory collapse
- Henry's Clinical Diagnosis & Management, 23rd Ed.; Pfenninger & Fowler's
Gross Appearance
| Appearance | Meaning |
|---|---|
| Clear and colorless | Normal |
| Turbid / cloudy | WBC >200/μL or RBC >400/μL; suggests infection |
| Frankly purulent | Severe bacterial meningitis |
| Uniformly bloody (all tubes) | True subarachnoid hemorrhage |
| Bloody, clears tube 1 → 3 | Traumatic tap |
| Pink xanthochromia | Oxyhemoglobin from RBC lysis; SAH (detectable 2-4 hrs after bleed) |
| Yellow xanthochromia | Bilirubin from hemoglobin breakdown; SAH (appears ~12 hrs after bleed) |
| Orange | RBC lysis OR dietary hypervitaminosis A (carotenoids) |
| Yellow-green | Hyperbilirubinemia (biliverdin) |
| Brown | Meningeal metastatic melanoma |
| Viscous | Cryptococcal meningitis (capsular polysaccharide); mucin-producing carcinoma |
| Clot formation | Traumatic tap, complete spinal block (Froin syndrome), suppurative/TB meningitis |
Xanthochromia timeline (Henry's, 23rd Ed.):
- Pink (oxyhemoglobin): detectable 2-4 hours after SAH; peaks at 24-36 hrs; disappears over 4-8 days
- Yellow (bilirubin): appears ~12 hours after SAH; peaks at 2-4 days; persists 2-4 weeks
Artifactual xanthochromia (false positive): hyperbilirubinemia, CSF protein >150 mg/dL, traumatic tap with >100,000 RBCs/μL, carotenoids, rifampin therapy, detergent contamination, delay >1 hour without processing
Distinguishing traumatic tap from true SAH:
- Bloody CSF that progressively clears from Tube 1 to Tube 3/4 = traumatic tap
- Xanthochromia after centrifugation = true SAH
- Erythrophagocytosis or hemosiderin-laden macrophages = true SAH
- Very high opening pressure (up to 500 mm H₂O) = more consistent with SAH
- Henry's Clinical Diagnosis & Management, 23rd Ed., p. 589; Quick Compendium of Clinical Pathology, 5th ed.
Normal CSF Reference Values
| Parameter | Adult Normal | Neonates |
|---|---|---|
| Opening pressure (mm H₂O) | 70-180 | 10-100 |
| WBC count (/μL) | 0-5 | 0-30 |
| Lymphocytes | 62 ± 34% | 20 ± 18% |
| Monocytes | 36 ± 20% | 72 ± 22% |
| Neutrophils | 2 ± 5% (≤7% acceptable) | 3 ± 5% |
| Glucose (mg/dL) | 50-80 | Varies |
| CSF:serum glucose ratio | 60-70% (range 40-80%) | 44-128% |
| Total protein (mg/dL) | 15-45 | 20-170 (mean 90) |
| RBC | None | None (minor traumatic bleeding common) |
Normal CSF: lymphocytes and monocytes in a 70:30 ratio. Higher proportion of monocytes in young children (up to 80% monocytes normal).
- Pfenninger & Fowler's Procedures for Primary Care, p. 1440; Henry's Clinical Diagnosis & Management, 23rd Ed.
Glucose
- Normal CSF glucose = 60-70% of plasma glucose
- Always order a simultaneous serum glucose (ideally obtained 2-4 hours before LP for equilibration)
- Hypoglycorrhachia (CSF glucose <40 mg/dL, or CSF:serum ratio <30%): bacterial meningitis, TB meningitis, fungal meningitis, carcinomatous meningitis, hypoglycemia
- Normal glucose favors: viral meningitis, early bacterial meningitis, aseptic meningitis
Protein
- Normal adult: 15-45 mg/dL
- Protein concentration increases from ventricular CSF (lowest) → lumbar CSF (highest) - because proteins diffuse from plasma along a concentration gradient down to the lumbar space
- Elevated CSF protein seen in: bacterial meningitis (100-500 mg/dL), TB/fungal meningitis, viral meningitis (mild), MS, Guillain-Barré, tumors, SAH, hypothyroidism, spinal cord compression
- Froin syndrome: protein >500 mg/dL, yellow xanthochromic CSF that clots spontaneously - indicates complete spinal block
- More than 80% of CSF protein originates from plasma ultrafiltration; remainder from intrathecal synthesis
Special protein markers:
- Oligoclonal IgG bands: intrathecal IgG synthesis - hallmark of MS (also seen in CNS infections)
- Myelin basic protein: active myelin destruction (MS, acute CNS injury)
- CSF albumin index (CSF albumin/serum albumin): assesses blood-brain barrier integrity; ratio <1:230 = intact BBB
- Beta-2 transferrin (asialated transferrin): specific for CSF - diagnoses CSF rhinorrhea/otorrhea
- Tau protein and beta-amyloid isoforms: Alzheimer disease diagnosis/prognosis
- 14-3-3 protein: Creutzfeldt-Jakob disease
- S-100B, NSE, GFAP: traumatic/ischemic brain injury markers
- CSF glutamine: elevated in hepatic encephalopathy
- Tietz Textbook of Laboratory Medicine, 7th Ed.; Henry's Clinical Diagnosis & Management, 23rd Ed.
Cell Count and Differential
Normal: 0-5 WBCs/μL in adults (0-30 in neonates). No RBCs.
Pleocytosis patterns and clinical significance:
Neutrophilic (PMN) pleocytosis - Causes (Box 30.3, Henry's):
- Bacterial meningitis (>60% PMNs; PMN count >1,180/μL has 99% predictive value for bacterial meningitis)
- Early viral meningoencephalitis (PMNs may predominate first 24-48 hrs, then shift to lymphocytes)
- Early TB and fungal meningitis
- Amebic encephalomyelitis
- CNS abscess, subdural empyema
- Following seizures, CNS hemorrhage, or CNS infarct
- Metastatic tumor in contact with CSF
- Injection of foreign material (methotrexate, contrast media)
Lymphocytic pleocytosis - Causes:
- Viral meningitis (aseptic meningitis)
- Tuberculous meningitis
- Fungal meningitis (cryptococcal, coccidioidal)
- Syphilitic meningoencephalitis
- MS, Guillain-Barré syndrome
- Sarcoidosis, subacute sclerosing panencephalitis
- Parasitic CNS infestations (cysticercosis, toxoplasmosis)
- Early bacterial meningitis with low leukocyte counts
Eosinophilic pleocytosis (rare):
- Parasitic infections: Angiostrongylus cantonensis, Gnathostoma, Baylisascaris, cysticercosis, schistosomiasis
- Fungal meningitis (coccidioidal: 6-20% eosinophils with lymphocytic pleocytosis)
- Lymphoma, leukemia, metastatic carcinoma
- Sarcoidosis, hypereosinophilic syndrome
- Henry's Clinical Diagnosis & Management, 23rd Ed., pp. 590-591
CSF Lactate
- Normal: ~1.1-2.4 mmol/L
- Increased in: bacterial meningitis (marked), fungal/TB meningitis (mild-moderate), viral meningitis (normal to mildly elevated)
- Can help differentiate bacterial from viral meningitis when Gram stain is negative
Typical CSF Findings in Meningitis (Comparison Table)
| Parameter | Bacterial | Viral | Fungal | Tuberculous |
|---|---|---|---|---|
| Opening pressure | Elevated (>180 mm H₂O) | Usually normal | Variable | Variable (often elevated) |
| WBC count | ≥1,000/μL | <100/μL | Variable | Variable |
| Cell differential | Mainly neutrophils* | Mainly lymphocytes† | Mainly lymphocytes | Mainly lymphocytes |
| Protein | Mild to marked increase (100-500 mg/dL) | Normal to mild increase | Increased | Increased |
| Glucose | Usually ≤40 mg/dL | Normal | Decreased | Decreased (<45 mg/dL) |
| CSF:serum glucose | Normal to marked decrease | Usually normal | Low | Low |
| Lactic acid | Mild to marked increase | Normal to mild increase | Mild-moderate increase | Mild-moderate increase |
| Gram stain | Positive 60-90% | Negative | Negative | Negative |
| Culture | Positive 70-85% | ~50% (PCR better) | Low-moderate | Low yield |
* Lymphocytosis present in ~10% of bacterial meningitis cases
† Neutrophils may predominate early in viral disease (shift to lymphocytes in 2-3 days)
- Henry's Clinical Diagnosis & Management, 23rd Ed., p. 598
Special/Advanced CSF Tests
| Test | Use |
|---|---|
| India ink | Cryptococcus neoformans - visualizes large capsule |
| Cryptococcal antigen (latex agglutination) | More sensitive than India ink for cryptococcal meningitis |
| VDRL | Neurosyphilis - highly specific but only ~70% sensitive |
| Oligoclonal bands + IgG index | Multiple sclerosis (intrathecal IgG synthesis) |
| Myelin basic protein | Active demyelination |
| Beta-2 transferrin | CSF leak diagnosis (rhinorrhea, otorrhea) |
| Cytology / flow cytometry | Leptomeningeal malignancy, lymphoma, leukemia |
| PCR (16S rRNA) | Broad bacterial detection; useful in partially treated meningitis |
| Multiplex PCR panels | Bacteria, viruses, fungi simultaneously |
| Beta-glucan assay | Fungal meningitis when other tests negative |
| Metagenomic next-generation sequencing | Unbiased pathogen identification in challenging cases |
| Tau / beta-amyloid | Alzheimer disease workup |
| 14-3-3 protein | Creutzfeldt-Jakob disease |
| PLAP (placental alkaline phosphatase) | Pineal germ cell tumors (radio-sensitive) |
| CSF lactate + adenosine deaminase (ADA) | TB meningitis workup |
| Ferritin | Late-presenting SAH (elevated) |
Diseases Detected by CSF Laboratory Examination (Henry's Clinical Diagnosis, 23rd Ed.)
| Diagnostic Accuracy | Conditions |
|---|---|
| High sensitivity + High specificity | Bacterial meningitis, TB meningitis, viral meningitis, fungal meningitis, viral encephalitis |
| High sensitivity + Moderate specificity | Subarachnoid hemorrhage, multiple sclerosis, neurosyphilis, infectious polyneuritis, paraspinal abscess |
| Moderate sensitivity + High specificity | Meningeal malignancy |
| Moderate sensitivity + Moderate specificity | Intracranial hemorrhage, subdural hematoma |
Practical summary for traumatic tap correction (Henry's): For every 700 RBCs in CSF (traumatic tap), CSF WBC count increases by ~1 cell/μL and CSF protein rises by ~8 mg/dL per 10,000 RBCs/μL. Formally:
- WBC corrected = WBC observed - (WBC blood × RBC csf / RBC blood)
- These corrections are valid only if all measurements are made from the same tube and peripheral counts are not extremely abnormal.
This is a shared conversation. Sign in to Orris to start your own chat.