List of Inhalation devices in copd full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full 15-mark MD exam answer.
Inhalation Devices in COPD - Full Details (15 Marks Answer)
Introduction
Inhaled therapy is the cornerstone of pharmacological management in COPD. It targets drug directly to the lungs, provides faster onset of action, allows lower drug doses, and reduces systemic adverse effects compared to oral therapy. Only 10-20% of an inhaled drug reaches the lungs - the remaining 80-90% is swallowed and enters systemic circulation via the GI tract and liver (first-pass effect).
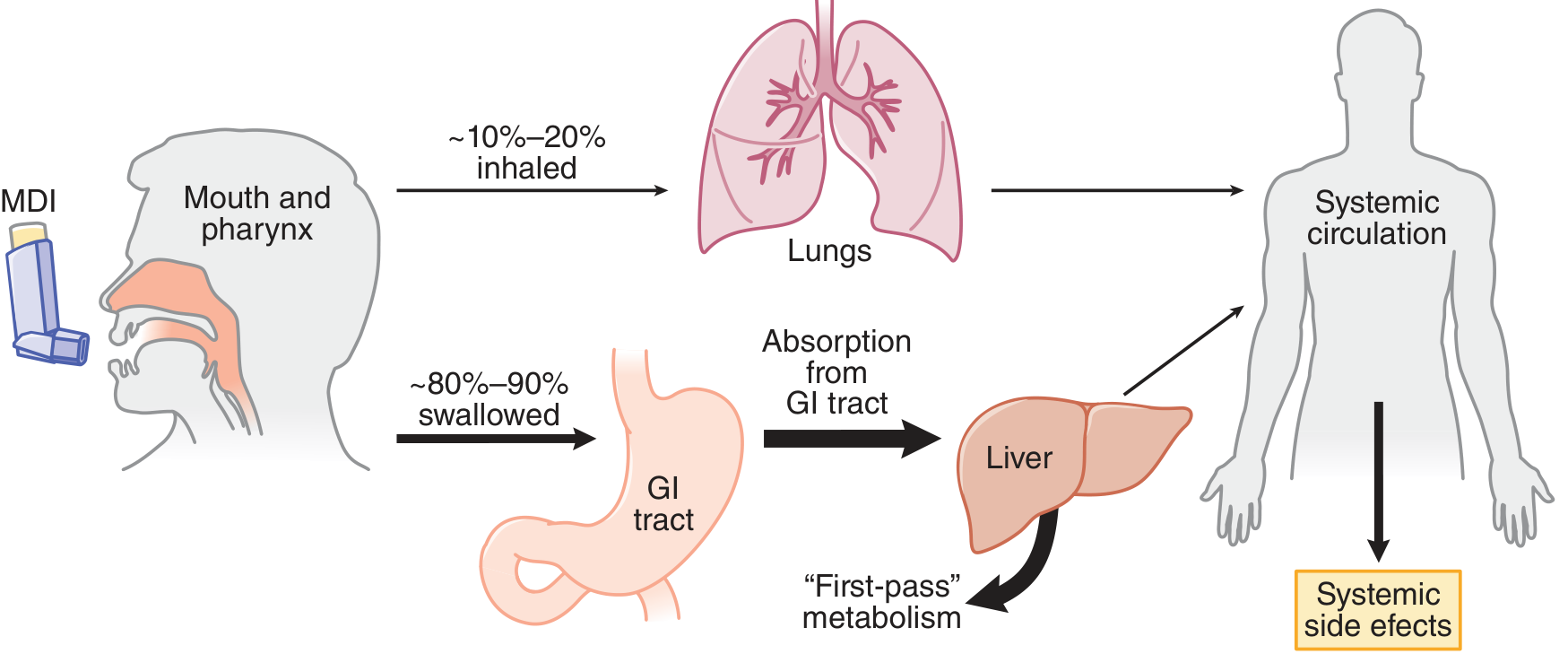
Drug deposition after inhalation - Goodman & Gilman's Pharmacological Basis of Therapeutics
Classification of Inhalation Devices
| Device | Type |
|---|---|
| 1. Pressurized Metered-Dose Inhaler (pMDI) | Propellant-driven |
| 2. Spacer / Valved Holding Chamber | pMDI add-on |
| 3. Dry Powder Inhaler (DPI) | Breath-actuated, propellant-free |
| 4. Nebulizer (Jet / Ultrasonic / Mesh) | Solution/suspension aerosolization |
| 5. Soft Mist Inhaler (SMI) | e.g., Respimat |
1. Pressurized Metered-Dose Inhaler (pMDI)
Mechanism
- Drug is formulated as a liquid suspension or solution with a propellant inside a sealed pressurized canister.
- Older propellant: Chlorofluorocarbons (CFC/Freon) - now replaced by ozone-friendly Hydrofluoroalkanes (HFA) / Hydrofluorocarbons (HFC).
- On actuation, rapid vaporization of propellant aerosolizes the drug into fine particles.
- Typically delivers 50-200 doses per canister.
Particle Size and Lung Deposition
- Optimal particle size for lower airway deposition: 1-5 micrometers (MMAD)
- HFA pMDIs deliver finer particles to smaller airways but also increase systemic absorption.
- With standard technique: only ~10-20% of the dose reaches the lungs.
Correct Inhalation Technique (Critical for Exams)
- Shake the inhaler
- Exhale fully
- Place mouthpiece in mouth and form a tight seal
- Actuate at the START of a deep, slow inhalation lasting ~5 seconds
- Hold breath for at least 5 seconds at end of inspiration
- Wait 1 minute before second puff if needed
- Common errors: failure to inhale slowly and deeply; poor hand-mouth coordination (especially in elderly).
Breath-Actuated pMDI
- Triggered by patient's inspiratory flow to overcome coordination problems.
- Examples: Autohaler, Easi-Breathe.
- However, studies show no advantage over correct conventional pMDI technique.
Advantages
- Compact and portable
- Multidose (50-200 doses)
- Quick treatment time
- Drug in sealed canister (protected from humidity)
- Inexpensive
Disadvantages
- High oropharyngeal deposition (up to 80-90% without spacer)
- Requires good hand-mouth coordination
- Propellants may cause "cold Freon" effect
- HFA propellants contribute to climate change (carbon footprint)
- Difficult to assess when canister is empty
2. Spacer Devices (Valved Holding Chambers)
Mechanism
- A spacer is an add-on chamber placed between the pMDI and the patient's mouth.
- Reduces the high velocity of aerosol cloud.
- Allows evaporation of liquid propellant, producing smaller drug particles that deposit deeper in the lungs.
- Traps large particles on the plastic walls, reducing oropharyngeal impaction.
Types of Spacers
| Type | Description |
|---|---|
| Valved holding chamber | Has a one-way inhalation valve - allows drug to be inhaled when patient is ready |
| Simple extension device | Non-valved; still requires reasonable coordination |
| Reverse-flow device | Aerosol actuated away from patient into a collapsible bag |
Clinical Importance in COPD
- Reduces oropharyngeal deposition of inhaled corticosteroids (ICS) - thus reducing local side effects (oral candidiasis, dysphonia) and systemic absorption via GI tract.
- Useful in elderly patients and children as young as 3 years with face mask attachment.
- Particularly helpful in patients with poor coordination.
Key Points for Correct Spacer Use
- Prime the spacer with the pMDI before use.
- Actuate one puff at a time - not multiple simultaneous doses (reduces electrostatic charge effect).
- Wash with ionic detergent and air dry to reduce electrostatic charge.
- Should be prescribed with compatible pMDI only - not interchangeable between devices.
- Antistatic spacers are available.
Advantages
- Overcomes coordination problems
- Reduces oropharyngeal deposition
- Reduces local and systemic ICS side effects
- Useful for elderly, children, and acute exacerbations
Disadvantages
- Bulky and less portable
- Electrostatic charge can reduce drug delivery
- Must be device-specific (not universally compatible)
3. Dry Powder Inhaler (DPI)
Mechanism
- Propellant-free devices.
- Drug is present as finely milled powder particles either:
- Bound to larger lactose carrier molecules
- As loose powder aggregates
- Breath-actuated: patient's own inspiratory effort disperses and de-aggregates the drug from the carrier particle.
- Requires minimum inspiratory flow rate for adequate drug dispersion (usually >30-60 L/min).
Classification of DPIs
| Type | Examples | Details |
|---|---|---|
| Single-dose (unit-dose) | Handihaler (tiotropium) | Drug loaded individually from gelatin capsules; capsule is punctured and drug inhaled |
| Multi-unit-dose | Accuhaler/Diskus | Drug sealed in individual foil blisters on a moving strip |
| Multi-dose (reservoir) | Turbuhaler, Genuair | Drug metered from a powder reservoir; requires priming |
DPI Devices Used in COPD (Examples)
- Turbuhaler - Budesonide, formoterol
- Accuhaler (Diskus) - Salmeterol/fluticasone, tiotropium
- Handihaler - Tiotropium (single-capsule device)
- Breezhaler - Indacaterol, glycopyrronium
- Genuair/Pressair - Aclidinium
- Ellipta - Umeclidinium/vilanterol, fluticasone furoate
Problems in COPD Patients
- Patients with moderate-to-severe COPD may not generate adequate inspiratory flows.
- Insufficient inspiratory effort is the most common inhaler error with DPIs - associated with worsening disease and increased exacerbation frequency.
- Children under 7 years cannot use DPIs effectively.
- Humidity can degrade the powder - must be stored in dry environment.
Advantages
- Compact and portable
- Quick treatment time
- Breath-actuated - no hand-mouth coordination needed
- No propellant (no ozone/climate issue)
- Simple to use if adequate inspiratory flow can be generated
Disadvantages
- Requires adequate inspiratory flow (problematic in severe COPD)
- High oropharyngeal deposition
- Humidity degrades the drug
- Patients may be intolerant to lactose carrier (rare)
- Not suitable for very young children or acutely ill patients with very poor inspiratory effort
4. Nebulizers
Mechanism
- Drug is dissolved or suspended in liquid (saline-based) and aerosolized into a fine mist for tidal breathing inhalation.
- Does NOT require coordination or high inspiratory effort.
- Suitable for tidal breathing at rest.
- Can deliver much higher drug doses than pMDIs.
Types of Nebulizers
A. Jet Nebulizer
- Uses compressed gas (air or oxygen) or an electrical compressor.
- High-velocity air directed through a Venturi opening across the liquid drug to produce aerosolized droplets.
- Most widely used type.
- Larger, noisier.
- Effective for both solutions and suspensions.
B. Ultrasonic Nebulizer
- Uses a rapidly vibrating piezoelectric crystal at high frequency to produce aerosol.
- Does NOT require a compressed gas source.
- Smaller and quieter than jet nebulizers.
- More expensive and less robust.
- Less effective for nebulizing suspensions.
C. Mesh Nebulizer (newer generation)
- Drug passes through a vibrating mesh with thousands of laser-drilled holes.
- More efficient drug delivery, less waste during exhalation.
- Better portability and consistency.
- Provides feedback for compliance monitoring.
- More expensive but cost-effective due to reduced drug waste.
Clinical Use in COPD
- Acute exacerbations of COPD - most common use, especially in hospital.
- When airway obstruction is extreme (severe COPD, inability to use other devices).
- Patients who are very old, very young, or mentally incapacitated.
- Delivery of high-dose antibiotics (e.g., inhaled tobramycin in bronchiectasis/COPD overlap).
- Drugs that must be given at high doses.
Factors Affecting Nebulizer Delivery
- Crying in children greatly reduces lung deposition.
- Shallow/rapid breathing reduces efficiency.
- Face mask must fit correctly to avoid drug deposition on the face and eyes.
- Significant variability in output between different nebulizer models.
Advantages
- Large doses of drug can be delivered
- Tidal breathing - no coordination or inspiratory effort needed
- Suitable for all ages including very young, elderly, acutely ill
- Many drug solutions can be aerosolized
- No patient cooperation needed for technique
Disadvantages
- Bulky, cumbersome, and expensive
- Wasted drug in nebulizer reservoir (significant loss during exhalation with conventional nebulizers)
- Variable aerosol output between models
- Time consuming (5-15 minutes per treatment)
- Requires power source
- Requires regular cleaning and maintenance (infection risk)
5. Soft Mist Inhaler (SMI) - e.g., Respimat
- Uses a spring-driven mechanical system to produce a slow-moving fine aerosol mist without propellant.
- More drug reaches the lungs (~50%) compared to pMDI (~10-20%).
- Slow aerosol velocity reduces oropharyngeal impaction.
- The combination of albuterol + ipratropium is available in SMI form.
- Useful in patients who struggle with pMDI coordination.
- Does not require strong inspiratory effort like DPIs.
Comparison Table: Advantages and Disadvantages
| Device | Advantages | Disadvantages |
|---|---|---|
| pMDI | Compact, portable, multidose, inexpensive, sealed canister | Poor oropharyngeal deposition, needs coordination, propellant issues |
| Spacer | Reduces side effects, helps elderly/children, better lung deposition | Bulky, device-specific, electrostatic charge issues |
| DPI | Compact, breath-actuated, no propellant | Needs high inspiratory flow, humidity-sensitive, not for severe COPD |
| Nebulizer | High dose delivery, tidal breathing, universal | Bulky, slow, expensive, variable output, maintenance required |
| SMI | Higher lung deposition, slow mist, no propellant | More expensive, specific device |
Factors Determining Choice of Inhaler in COPD
- Disease severity - Severe COPD patients may not achieve adequate inspiratory flow for DPIs; nebulizers may be preferred.
- Patient ability - Poor coordination favors DPIs, SMI, or spacer+pMDI; very old/young patients may need nebulizers.
- Setting - Acute exacerbation: nebulizer preferred; stable outpatient: pMDI or DPI.
- Drug availability - Not all drugs are available in all devices.
- Cost - pMDI generally cheapest; mesh nebulizers most expensive.
- Compliance - Same device type for all drugs improves compliance.
- Technique training - Healthcare workers must assess and regularly review inhaler technique.
- Environmental considerations - pMDI propellants (HFAs) contribute to climate change.
Key Exam Points
- DPIs are breath-actuated - require adequate inspiratory flow; problematic in severe COPD.
- pMDIs need hand-mouth coordination - solved by spacers or breath-actuated pMDIs.
- Nebulizers are gold standard in acute exacerbations and extreme airway obstruction.
- Spacers reduce ICS side effects (oral candidiasis, dysphonia, systemic absorption).
- Studies show pMDI, DPI, and SMI are equally effective as nebulizers in stable COPD patients who use correct technique.
- GOLD guidelines emphasize periodic reassessment of inhaler technique - incorrect technique is universal and worsens outcomes.
- More than 250 device-drug combinations exist; prescribers and patients are commonly confused.
- A newer generation of DPIs requires lower inspiratory flows or delivers drug independent of breathing maneuver.
Sources: Fishman's Pulmonary Diseases and Disorders (5th ed.) - Inhaler Devices, p. 804-805; Goodman & Gilman's Pharmacological Basis of Therapeutics - Delivery Devices, p. 2351-2357; Murray & Nadel's Textbook of Respiratory Medicine - COPD Management, p. 1826-1828
This is a shared conversation. Sign in to Orris to start your own chat.