Balanced diet Anemia mukt Bharat Community nutrition programmes (Strictly from the park textbook spm - university exam pov)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content needed. Let me compile the full, exam-ready answer.
1. BALANCED DIET
(Park's Textbook of Preventive and Social Medicine)
Definition
A diet is defined as the kinds of food on which a person or group lives.
A balanced diet is defined as one which contains a variety of foods in such quantities and proportions that the need for energy, amino acids, vitamins, minerals, fats, carbohydrates and other nutrients is adequately met for maintaining health, vitality and general well-being, and also makes a small provision for extra nutrients to withstand short durations of leanness.
A balanced diet has become an accepted means to safeguard a population from nutritional deficiencies.
Principles of Constructing a Balanced Diet
When constructing a balanced diet, the following principles should be borne in mind:
| Component | Recommendation |
|---|---|
| (a) Protein | Should be met first; amounts to 10-15% of daily energy intake |
| (b) Fat | Should be limited to 15-30% of daily energy intake |
| (c) Carbohydrates | Rich in natural fibre; should constitute the remaining food energy |
| (d) Micronutrients | Requirements of vitamins and minerals (as per RDA 2020) should be met |
Dietary Goals (WHO "Prudent Diet")
All countries should develop a national nutrition and food policy setting out dietary goals. WHO-recommended dietary goals are:
(a) Dietary fat limited to approximately 15-30% of total daily intake.
(b) Saturated fats: no more than 10% of total energy intake; unsaturated vegetable oils should be substituted.
(c) Excessive consumption of refined carbohydrate should be avoided; carbohydrate rich in natural fibre should be taken.
(d) Sources rich in energy such as fats and alcohol should be restricted.
(e) Salt intake reduced to not more than 5 g/day (India averages 15 g/day).
(f) Protein: approximately 10-15% of daily intake.
(g) Junk foods such as colas, ketchups and other foods that supply empty calories should be reduced.
Note: Diet should be adapted to the special needs of growth, pregnancy, lactation, physical activity, and medical disorders (e.g., diabetes).
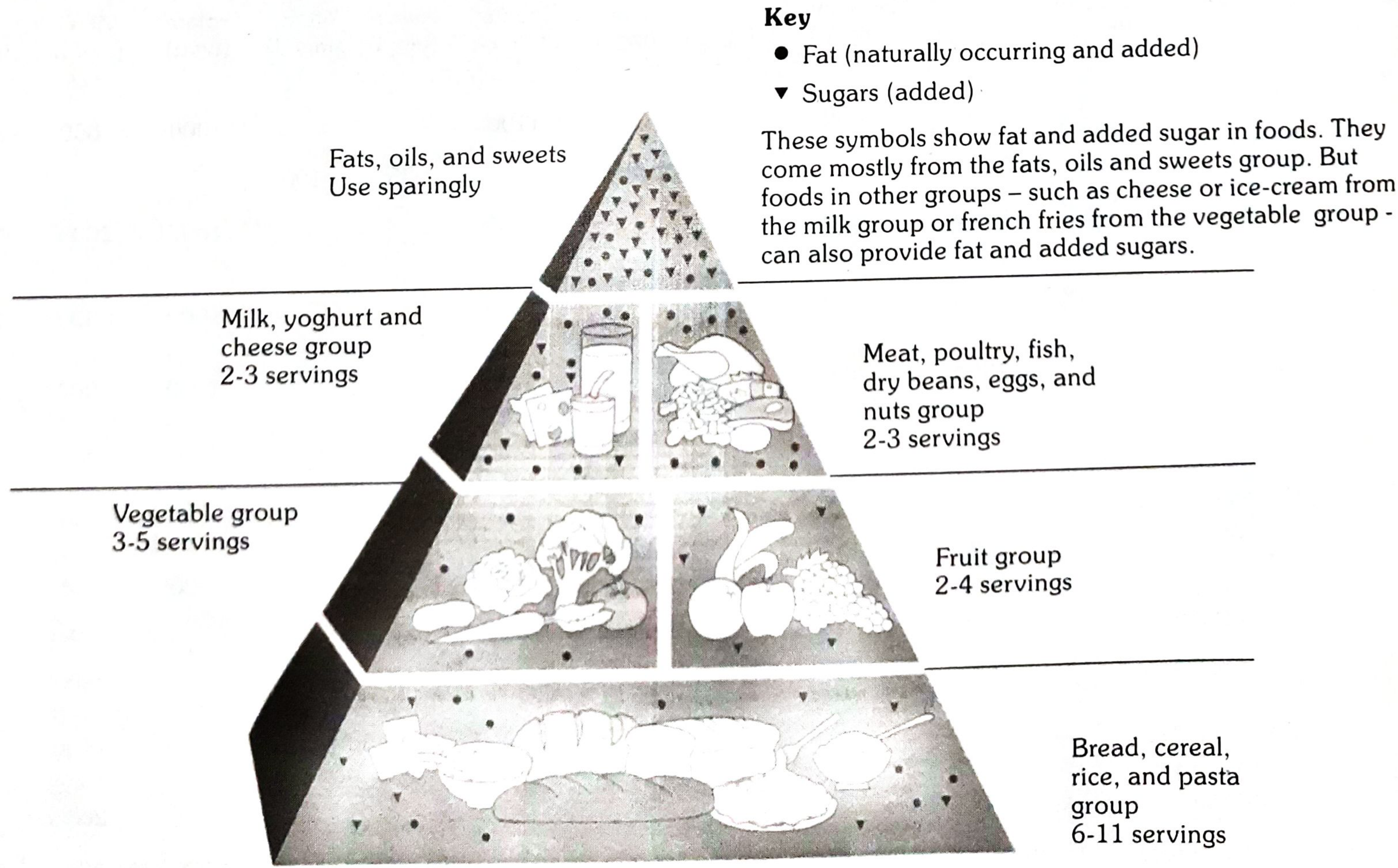
Food Guide Pyramid
The Food Guide Pyramid is a nutritional education guide emphasizing foods from the five major food groups shown in the three lower sections:
- No single food group is more important than another
- Each group provides some, but not all, of the required nutrients
- Foods in one group cannot replace those in another
RDA for Indians - 2020 (Key values for Moderate Work)
| Nutrient | Men (moderate work, 65 kg) | Women (moderate work, 55 kg) |
|---|---|---|
| Protein | 54.0 g/d | 46.0 g/d |
| Calcium | 1000 mg/d | 1000 mg/d |
| Iron | 19 mg/d | 29 mg/d |
| Vitamin A | 1000 µg/d | 840 µg/d |
| Vitamin C | 80 mg/d | 65 mg/d |
| Vitamin D | 600 IU/d | 600 IU/d |
| Folate | 300 µg/d | 220 µg/d |
| Iodine | 150 µg/d | 150 µg/d |
(Source: Park's SPM, Table 28 - RDA for Indians 2020)
2. ANAEMIA MUKT BHARAT STRATEGY
(Park's Textbook of Preventive and Social Medicine, p. 756)
Background
Anaemia Mukt Bharat (AMB) is a universal strategy launched to reduce the burden of anaemia in India. It is implemented through existing delivery platforms as envisaged in the:
- National Iron Plus Initiative (NIPI)
- Weekly Iron Folic Acid Supplementation (WIFS) programme
Six Key Interventions
The Anaemia Mukt Bharat Strategy focuses on 6 interventions:
1. Prophylactic iron and folic acid (IFA) supplementation
2. Deworming
3. Intensified year-round Behaviour Change Communication (BCC) campaign - "Solid Body, Smart Mind" - focusing on four key behaviours:
- (a) Improving compliance to IFA supplementation and deworming
- (b) Appropriate infant and young child feeding practices
- (c) Increase in intake of iron-rich food through diet diversity/quantity/frequency and/or fortified foods, with focus on harnessing locally available resources
- (d) Ensuring delayed cord clamping after delivery (by 3 minutes) in health facilities
4. Testing and treatment of anaemia using digital methods and point of care treatment, with special focus on pregnant women and school-going adolescents
5. Mandatory provision of iron and folic acid fortified foods in government-funded public health programmes
6. Intensifying awareness, screening and treatment of non-nutritional causes of anaemia in endemic pockets, with special focus on:
- Malaria
- Haemoglobinopathies
- Fluorosis
Implementation
The AMB Strategy will be implemented in all villages, blocks, and districts of all states/UTs of India through existing delivery platforms as envisaged in NIPI and WIFS.
3. COMMUNITY NUTRITION PROGRAMMES
(Park's Textbook of Preventive and Social Medicine, p. 756-759)
Overview
The Government of India has initiated several large-scale supplementary feeding programmes and programmes aimed at overcoming specific deficiency diseases through various Ministries to combat malnutrition.
List of Nutrition Programmes in India (Table 38 - Park's)
| Programme | Ministry |
|---|---|
| 1. Vitamin A prophylaxis programme | Ministry of Health and Family Welfare |
| 2. Prophylaxis against nutritional anaemia | Ministry of Health and Family Welfare |
| 3. Iodine deficiency disorders control programme | Ministry of Health and Family Welfare |
| 4. Special nutrition programme | Ministry of Social Welfare |
| 5. Balwadi nutrition programme | Ministry of Social Welfare |
| 6. ICDS programme | Ministry of Social Welfare |
| 7. Mid-day meal programme | Ministry of Education |
| 8. Mid-day meal scheme | Ministry of Human Resource Development |
Details of Each Programme
1. Vitamin A Prophylaxis Programme
- Component of the National Programme for Control of Blindness
- A single massive dose of 200,000 IU of oily preparation of Vitamin A (110 mg retinol palmitate) given orally
- Administered to all pre-school children every 6 months through peripheral health workers
- Launched by MoHFW in 1970 based on technology from National Institute of Nutrition (NIN), Hyderabad
- Evaluation revealed significant reduction in Vitamin A deficiency
2. Prophylaxis Against Nutritional Anaemia
- National programme launched during the Fourth Five Year Plan
- Distribution of iron and folic acid (folifar) tablets to pregnant women and young children (1-12 years)
- Implemented through MCH centres (urban), PHCs (rural), and ICDS projects
- Technology for anaemia control through iron fortification of common salt also developed at NIN, Hyderabad
3. Control of Iodine Deficiency Disorders (IDD)
- National Goitre Control Programme launched in 1962 in the Himalayan goitre belt
- Objective: supply iodized salt in place of common salt
- Surveys showed the problem was more widespread - about 145 million people in known goitre endemic areas
- Major national IDD Control Programme launched in 1986 with objective to replace entire edible salt with iodized salt in a phased manner by 1992
4. Special Nutrition Programme
- Started in 1970
- Target groups: Children below 6 years, pregnant and nursing mothers
- Areas covered: Urban slums, tribal areas, backward rural areas
- Supplement provides: 300 kcal and 10-12 g protein/child/day; mothers get 500 kcal and 25 g protein/day for ~300 days/year
- Gradually being merged into the ICDS programme
5. Balwadi Nutrition Programme
- Started in 1970
- Target group: Children aged 3-6 years in rural areas
- Under the Department of Social Welfare
- Implemented through Balwadis (which also provide pre-primary education)
- Supplement: 300 kcal and 10 g protein/child/day
- Balwadis are being phased out because of universalization of ICDS
6. ICDS Programme (Integrated Child Development Services)
- Started in 1975 in pursuance of the National Policy for Children
- Strong nutrition component: supplementary nutrition, Vitamin A prophylaxis, IFA distribution
- Beneficiaries: Preschool children below 6 years, adolescent girls (11-18 years), pregnant and lactating mothers
- Village-level workers: Anganwadi workers
- Each Anganwadi unit covers population of 400-800; mini anganwadi centres cover 150-400
- Supervised by Mukhyasevikas; CDPO does field supervision
- A network of Mahila Mandals helps Anganwadi workers
7. Mid-day Meal Programme (MDMP)
- Also known as School Lunch Programme
- In operation since 1961 throughout the country
- Major objective: Attract children for school admission and retain them (improve literacy)
- Became part of the Minimum Needs Programme in the Fifth Five Year Plan
8. Mid-day Meal Scheme
- Also known as National Programme of Nutritional Support to Primary Education
- Launched as centrally sponsored scheme on 15th August 1995, revised in 2004
- Objective: Universalization of primary education by increasing enrolment, retention and attendance + improving nutrition
- Extended in Oct 2002 to EGS and Alternative/Innovative Education Centres
- Central assistance: free supply of food grain at 100 g per student per day from FCI godown
- A cooked mid-day meal with minimum 300 Calories and 8-12 g protein per child (Class I-V)
Tips for Nutritious Mid-day Meals (Park's)
- Use whole wheat or broken wheat (dalia)
- Rice should be parboiled or unpolished
- Single-dish meals incorporating pulse, seasonal vegetable/green leafy vegetable, and edible oil
- Cereal-pulse ratio: 3:1 to 5:1
- Sprouted pulses have more nutrients
- Rice water after cooking should never be thrown away - mix with dal
- Minimum 250 feeding days/year for desired impact (as recommended by NIN)
All content sourced from: Park's Textbook of Preventive and Social Medicine, Chapter on Nutrition.
This is a shared conversation. Sign in to Orris to start your own chat.