Prolactin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive content. Let me compile the full answer.
Prolactin (PRL)
Structure and Synthesis
Prolactin is a 198-amino-acid single-chain polypeptide (molecular mass ~21,500 kDa) with 3 internal disulfide bridges. It is weakly homologous to growth hormone (GH) and human placental lactogen (hPL), reflecting duplication and divergence of a common GH-PRL-hPL precursor gene. PRL is synthesized by lactotropes (also called lactotrophs), which constitute approximately 15-20% of anterior pituitary cells. Lactotropes and somatotropes derive from a common precursor cell - this shared origin explains why some pituitary tumors co-secrete both PRL and GH.
A high-molecular-weight variant called macroprolactin ("big prolactin") forms when prolactin aggregates or complexes with IgG via intermolecular disulfide bridges. Despite immunoreactivity in standard assays, macroprolactin typically has decreased biologic activity - an important clinical consideration when interpreting elevated PRL levels.
- Harrison's Principles of Internal Medicine 22E, p. 3032
- Goldman-Cecil Medicine, p. 2407
- Costanzo Physiology 7th Ed., p. 416
Normal Secretion
| Parameter | Value |
|---|---|
| Normal serum PRL (women) | ~10-25 µg/L |
| Normal serum PRL (men) | ~10-20 µg/L |
| Peak levels (sleep) | up to 30 µg/L (4:00-6:00 AM) |
| Circulating half-life | ~50 minutes |
PRL secretion is pulsatile, with the highest peaks occurring during non-REM sleep. Levels transiently rise after exercise, meals, sexual intercourse, minor surgical procedures, general anesthesia, chest wall injury, acute myocardial infarction, and other acute stressors.
During pregnancy, PRL increases approximately 10-fold; levels decline rapidly within 2 weeks of parturition unless breast-feeding is initiated. Suckling activates afferent neural pathways in the hypothalamus that induce PRL release for ~30-45 minutes per episode.
- Harrison's, p. 3032
Regulation of Secretion
PRL is unique among pituitary hormones: its predominant hypothalamic control is inhibitory, not stimulatory. This is clinically important because any process that disrupts the hypothalamic-pituitary stalk (trauma, compression) will disinhibit prolactin and cause hyperprolactinemia.
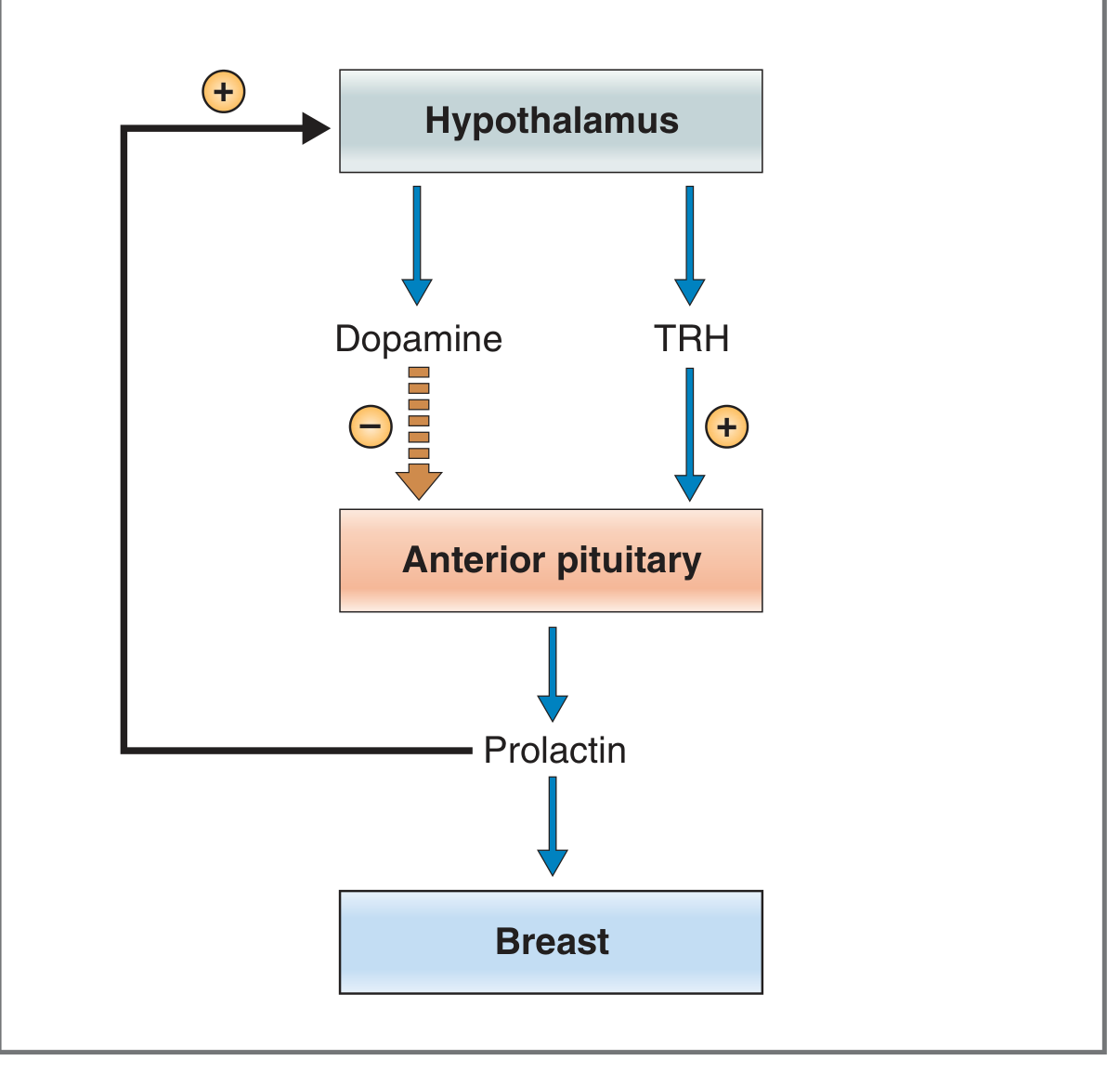
Fig. 9.12 from Costanzo Physiology - Regulation of prolactin secretion
Inhibitory pathway
- Dopamine is the principal prolactin-inhibiting factor (PIF). It is a catecholamine (unique among hypothalamic regulatory hormones, which are otherwise peptides).
- Acts via D2 receptors on lactotropes, decreasing cAMP and suppressing PRL gene transcription.
- Three sources of dopamine reach the anterior pituitary: (1) tuberoinfundibular dopaminergic neurons secreting into the median eminence portal system (main route), (2) dopaminergic neurons of the posterior pituitary via short portal veins, and (3) non-lactotroph anterior pituitary cells via paracrine diffusion.
- Prolactin exerts negative feedback on its own secretion by stimulating hypothalamic dopamine synthesis.
Stimulatory pathway
- TRH (a hypothalamic tripeptide) stimulates PRL release within 15-30 minutes of IV injection; physiologic relevance is debated but explains why hypothyroidism raises PRL levels (elevated TRH).
- Serotonin also promotes PRL release via pathways that are reciprocal to dopamine (relevant to antidepressant/antipsychotic effects on PRL).
Summary of factors affecting PRL secretion
| Stimulatory | Inhibitory |
|---|---|
| Pregnancy (estrogen) | Dopamine |
| Breast-feeding / suckling | Bromocriptine (dopamine agonist) |
| Sleep | Somatostatin |
| Stress | Prolactin (negative feedback) |
| TRH | |
| Dopamine antagonists (e.g., antipsychotics) |
- Costanzo Physiology, p. 417
- Harrison's, p. 3032
Receptor and Signal Transduction
The PRL receptor is a member of the type I cytokine receptor family (which also includes GH and IL-6 receptors). Ligand binding induces receptor dimerization and intracellular signaling via JAK2 (Janus kinase 2), which activates STAT transcription factors and downstream gene expression. The PRL receptor is expressed in a wide variety of tissues beyond the breast, including gonads, liver, kidney, adrenal gland, and immune cells.
- Harrison's, p. 3032
- Goldman-Cecil Medicine, p. 2407
Actions of Prolactin
1. Breast Development
- At puberty: with estrogen and progesterone, stimulates proliferation and branching of mammary ducts.
- During pregnancy: with estrogen and progesterone, drives growth and development of mammary alveoli.
- Number of lactotropes increases during pregnancy and early lactation to meet demand.
2. Lactogenesis (Milk Production)
- The primary physiologic action: stimulates synthesis of lactose, casein, and lipids in mammary alveolar cells.
- Mechanism: PRL binds membrane receptor → via JAK2 → induces gene transcription for biosynthetic enzymes.
- Key point: Although PRL is high throughout pregnancy, lactation is blocked until parturition by high estrogen and progesterone, which down-regulate PRL receptors in the breast. The post-partum drop in these hormones disinhibits PRL action.
3. Inhibition of Reproductive Function
PRL inhibits the hypothalamic-pituitary-gonadal axis:
- Suppresses hypothalamic GnRH secretion and pituitary gonadotropin (FSH/LH) secretion.
- In females: blocks folliculogenesis, inhibits granulosa cell aromatase (→ hypoestrogenism and anovulation), and has a luteolytic effect (shortened luteal phase).
- In males: suppresses LH → low testosterone → decreased spermatogenesis.
- Net effect: decreased libido and reduced fertility (the basis of lactational amenorrhea).
4. Maternal Behavior
PRL participates in regulation of behavioral aspects of reproduction and infant care, including estrogen-dependent sexual receptivity.
- Harrison's, p. 3032
- Costanzo Physiology, p. 417-418
Hyperprolactinemia
Causes
| Category | Examples | Mechanism | PRL Level |
|---|---|---|---|
| Drug-induced | Antipsychotics (haloperidol, risperidone, paliperidone) | D2 receptor blockade | 20-70 ng/mL |
| Antiemetics (metoclopramide, domperidone) | D2 receptor blockade | 20-70 ng/mL | |
| Cyclic antidepressants (clomipramine) | Unknown | 20-70 ng/mL | |
| Narcotics (methadone, morphine) | Opioid µ-receptor activation (indirect) | 20-70 ng/mL | |
| Estrogens / OCP | Stimulates PRL transcription | 20-70 ng/mL | |
| Hypothyroidism | Primary hypothyroidism | Elevated TRH | Moderate, <100 |
| Pituitary tumor | Prolactinoma (microadenoma) | Autonomous secretion | 20-250 ng/mL |
| Prolactinoma (macroadenoma) | Autonomous secretion | 200 - >10,000 ng/mL | |
| Stalk disruption | Non-secreting pituitary adenoma, head trauma, mass lesions | Reduced dopamine delivery | Usually <100 ng/mL |
| Pregnancy | Normal | Estrogen effect | 20-500 ng/mL |
| Renal failure / cirrhosis | Chronic kidney disease | Decreased clearance + central effect | Moderate, <100 |
| Stress | Chest wall injury, nipple stimulation | Hypothalamic | 20-70 ng/mL |
Clinical note: A very large PRL level (>200 ng/mL) almost always indicates a prolactinoma rather than stalk compression or drug effect. For markedly elevated levels (>1000 µg/L), diluted samples must be measured to avoid assay hook-effect artifacts.
- Goldman-Cecil Medicine, Table 205-8, p. 2407
Clinical Features of Hyperprolactinemia
- Women: amenorrhea/oligomenorrhea, galactorrhea, infertility, decreased libido, hypoestrogenism, reduced bone mineral density.
- Men: decreased libido, erectile dysfunction, infertility (low testosterone, decreased spermatogenesis), and less commonly gynecomastia/galactorrhea.
Galactorrhea
Inappropriate breast milk discharge persisting >6 months after childbirth or stopping breastfeeding. Associated with hyperprolactinemia of any cause. Bloody discharge from a single nipple warrants mammography to exclude breast cancer.
Prolactinoma
The most common functioning pituitary tumor - accounts for ~50% of all functioning pituitary adenomas.
- Population prevalence: ~10/100,000 in men, ~30/100,000 in women.
- Microadenoma: <1 cm; usually localized.
- Macroadenoma: ≥1 cm; may be locally invasive, impinge on optic chiasm, or cause mass effects.
Treatment of Hyperprolactinemia
General Principle
Goal: normalize PRL levels, alleviate gonadal suppression, halt galactorrhea, preserve bone mineral density.
Dopamine Agonists (First-Line for Prolactinoma and Most Cases)
- Cabergoline (0.5 mg once or twice weekly): preferred due to fewer side effects, better tolerability, and effectiveness even in bromocriptine-resistant cases. With prolonged use, the prolactinoma may shrink enough to allow drug discontinuation.
- Bromocriptine (2.5-7.5 mg/day in divided doses): the original dopamine agonist; start at low dose (0.625-1.25 mg at bedtime with a snack) and titrate gradually to minimize nausea.
Other Causes
- Drug-induced: withdraw offending agent if possible; for patients requiring antipsychotics, supervised dose titration or addition of a dopamine agonist (note: may worsen psychiatric condition); aripiprazole (a partial D2 agonist) is sometimes used adjunctively.
- Hypothyroidism: PRL normalizes with adequate thyroid hormone replacement.
- Renal failure: PRL typically normalizes after renal transplantation.
- Stalk compression by non-secreting mass: surgical resection reverses hyperprolactinemia.
- Spontaneous resolution: occurs in up to 30% of patients with hyperprolactinemia without visible microadenoma.
Surgery
Transsphenoidal surgery is reserved for cases with insufficient response to dopamine agonists, intolerable side effects, or vision-threatening macroadenomas unresponsive to medical therapy.
- Harrison's, p. 3032-3033
- Goldman-Cecil Medicine, p. 2407
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Bradley and Daroff's Neurology in Clinical Practice
Prolactin Deficiency
- Caused by destruction of the entire anterior pituitary or selective lactotroph destruction.
- Clinical result: failure to lactate (inability to breastfeed after parturition).
- Part of panhypopituitarism when the entire gland is involved (e.g., Sheehan syndrome).
Key Clinical Pearls
- Stalk section paradox: Unlike all other anterior pituitary hormones (which fall with stalk damage), PRL rises - because dopamine inhibition is removed.
- Antipsychotic-induced hyperprolactinemia: D2 blockers disinhibit lactotropes; second-generation antipsychotics (especially risperidone, paliperidone) are notable offenders; clozapine and quetiapine cause minimal prolactin elevation.
- Pregnancy and lactation: PRL rises 10-fold in pregnancy but doesn't cause lactation because estrogen/progesterone block PRL receptors; only after delivery does lactation begin.
- Hook effect: In very large prolactinomas with PRL >1000 µg/L, undiluted samples may give falsely low readings - always dilute to avoid missing a giant prolactinoma.
- Macroprolactin: High-molecular-weight PRL that is immunoreactive but biologically inactive; must be considered before treating an elevated PRL level.
This is a shared conversation. Sign in to Orris to start your own chat.