Enlist types of refractive surgery with its merits and demerits in details and steps of each surgery
types of refractive surgery LASIK LASEK PRK SMILE steps merits demerits 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC12755589
Types of Refractive Surgery - Complete Guide
Overview of Types
| Category | Procedures |
|---|---|
| Surface Ablation | PRK, LASEK, Epi-LASIK, Trans-PRK |
| Flap-based Laser | LASIK (microkeratome or FS-LASIK) |
| Flapless Stromal Extraction | SMILE |
| Phakic IOL Implantation | Iris-claw (Artisan/Verisyse), Posterior chamber phakic IOL (ICL/EVO ICL) |
| Lens-based | Clear Lens Exchange (CLE / Refractive Lens Exchange) |
| Incisional (older) | Radial Keratotomy (RK), Astigmatic Keratotomy (AK) |
1. PRK (Photorefractive Keratectomy)
Steps
- Preoperative assessment - Corneal topography, pachymetry, refraction, pupil size measurement; contact lenses discontinued 1-2 weeks prior.
- Instill topical anesthetic - e.g., proparacaine 0.5%.
- Epithelial removal - Using a sponge, automated brush (Amoils scrubber), blunt blade, alcohol (20% ethanol), or the excimer laser itself (Trans-PRK = single-step transepithelial).
- Corneal drying - The Bowman layer and anterior stroma are dried and exposed.
- Excimer laser ablation - Argon-fluoride excimer laser at 193 nm reshapes the anterior stroma (typically 30-60 seconds). Modern systems have eye-tracking and pupil centration.
- Mitomycin-C (MMC) application - 0.02% MMC sponge applied for 15-30 seconds in higher corrections to reduce haze risk; then washed off.
- Soft contact lens placement - Bandage contact lens placed for epithelial protection and comfort (typically removed at day 5-7 after re-epithelialization).
- Postoperative drops - Topical antibiotics + steroids; lubricants for 3-6 months.
Refractive Range
- Myopia: up to -8.0 D | Hypermetropia: up to +3.0 D | Astigmatism: up to 3.0 D
Merits
- No stromal flap - eliminates flap-related complications (dislocation, striae, keratitis)
- Best choice for thin corneas
- Preferred for patients at high risk of eye trauma (athletes, military, contact sports)
- Suitable for epithelial basement membrane disease
- No risk of late flap displacement
- Better long-term corneal biomechanical stability than LASIK
- Lowest risk of corneal ectasia among laser procedures
Demerits
- Significant postoperative pain (3-5 days) until re-epithelialization
- Slower visual recovery (1-4 weeks for functional vision)
- Higher risk of subepithelial haze - especially in >-5D corrections without MMC
- Bandage contact lens required
- Steroid drops needed for months (risk of steroid-induced glaucoma and cataract)
- Lower correctable refractive range compared to LASIK
2. LASEK (Laser-Assisted Sub-Epithelial Keratectomy)
Steps
- Preoperative preparation same as PRK.
- Alcohol application - A trephine well is placed on the cornea; 20% absolute alcohol is applied for ~25-30 seconds to chemically loosen the epithelium.
- Epithelial flap lifting - The softened epithelium is gently lifted as a hinged flap and folded to one side (usually 6 o'clock hinge).
- Excimer laser ablation - Same as PRK.
- MMC application if needed.
- Epithelial flap replacement - The epithelial flap is repositioned centrally to act as a biological bandage.
- Bandage contact lens placed.
- Postoperative care as with PRK.
Refractive Range
- Same as PRK: Myopia -8.0 D, Hypermetropia +3.0 D, Astigmatism up to 3.0 D
Merits
- No stromal flap - avoids LASIK flap complications
- The preserved epithelial flap may reduce postoperative discomfort compared to PRK
- Suitable for thin corneas
- Good option for epithelial pathology cases
Demerits
- The alcohol step can damage epithelial cells, reducing the benefit of preservation
- Postoperative pain similar to (sometimes worse than) PRK
- Slower visual recovery than LASIK
- Risk of subepithelial haze similar to PRK
- Alcohol toxicity to Bowman layer possible
- Epithelial flap can disintegrate, making it functionally equivalent to PRK
3. Epi-LASIK
Steps
- Preoperative assessment as standard.
- Epi-keratome application - A specialized blunt blade oscillating separator cleaves the epithelium at the basement membrane level (avoiding alcohol toxicity).
- Epithelial flap folded to the side.
- Excimer laser ablation.
- Epithelial flap repositioned (epi-on) or discarded (epi-off) based on surgeon preference.
- Bandage contact lens + postoperative drops.
Refractive Range
- Same as PRK/LASEK range.
Merits
- Avoids alcohol toxicity compared to LASEK
- Mechanical separation is more reproducible
- No stromal flap complications
- Suitable for thin corneas
Demerits
- Not ideal with significant anterior corneal scarring or glaucoma
- Recovery profile similar to PRK/LASEK - prolonged pain and slow visual recovery
- Subepithelial haze risk persists
- Less commonly performed today given SMILE's emergence
4. LASIK (Laser-Assisted In Situ Keratomileusis)
Steps
- Preoperative workup - Corneal topography (Pentacam/Orbscan), pachymetry (central corneal thickness must be >500 µm), refraction, dry eye assessment, dilated fundus exam.
- Preoperative preparation - Topical antibiotic eye drops day before; anesthetic drops on table. Patient positioned supine under laser.
- Suction ring application - A suction ring stabilizes the eye, raises IOP to ~65 mmHg.
- Flap creation:
- Microkeratome LASIK: Oscillating steel blade cuts a hinged flap (~100-160 µm thick, 8-9 mm diameter).
- FS-LASIK (All-laser LASIK): Femtosecond laser (1053 nm infrared) creates a more precise, thinner flap (~90-110 µm). Safer, more predictable, preferred currently.
- Flap lifting - The hinged flap is gently folded back, exposing the stromal bed.
- Excimer laser ablation - 193 nm argon-fluoride laser ablates the stroma to reshape the corneal curvature. Eye tracking compensates for involuntary movements. Duration: 20-60 seconds.
- Irrigation - The stromal bed is irrigated with BSS (balanced salt solution).
- Flap replacement - The flap is carefully repositioned over the ablated bed; alignment marks confirm correct orientation.
- Drying and sealing - A dry sponge gently dries the flap edges; the flap adheres by suction within minutes.
- Postoperative regimen - Topical antibiotic + steroid drops for 1-2 weeks; artificial tears for 3-6 months; protective shield at night for one week.
Refractive Range
- Myopia: up to -10.0 D | Hypermetropia: up to +3.0 D | Astigmatism: up to 3.0 D
Merits
- Rapid visual recovery - functional vision within 24 hours, excellent by 1 week
- Minimal postoperative pain (the flap acts as a natural bandage)
- Minimal stromal haze
- Broadest refractive correction range among corneal procedures
- High patient satisfaction
- Wavefront-guided and topography-guided variants treat higher-order aberrations
- Reversibility - the stromal bed is accessible for re-treatment/enhancement
Demerits
- Flap complications (1-2%): dislocation (can be lifelong), striae, free cap, incomplete or irregular flap
- Dry eye - most common complication; due to severed corneal nerves; can persist 6-12 months
- Diffuse lamellar keratitis (DLK) - "sands of Sahara" - inflammatory reaction at flap interface; needs intensive steroids
- Epithelial ingrowth under the flap (1-2%)
- Corneal ectasia (0.2-0.6%) - progressive corneal thinning; more likely with thin corneas, forme fruste keratoconus, insufficient residual stromal bed
- Not ideal for thin corneas (<500 µm), epithelial dystrophies, severe dry eyes, contact sport athletes
- The flap creates a permanent structural weakness
- Bacterial keratitis (rare but serious)
- Pressure-induced stromal keratitis (PISK) with steroid use
5. SMILE (Small Incision Lenticule Extraction)
Steps
- Preoperative assessment - Same as LASIK; refraction must be stable.
- Topical anesthesia - Proparacaine drops; anxiolytics may be given.
- Docking - The patient fixates on a target light; suction is applied to dock the eye to the femtosecond laser delivery system.
- Femtosecond laser lenticule creation - The VisuMax femtosecond laser creates two curved intrastromal cuts defining a disc-shaped lenticule of stroma (the refractive lenticule) whose shape and thickness correspond to the refractive correction needed. A small 2-3 mm peripheral side-cut incision is simultaneously made.
- Lenticule dissection - The surgeon inserts a spatula through the small incision and bluntly dissects the anterior plane of the lenticule, then the posterior plane, separating it from surrounding stroma.
- Lenticule extraction - The freed disc of stroma is grasped with forceps and extracted through the 2-3 mm incision.
- Irrigation - The intrastromal pocket is irrigated.
- Postoperative drops - Topical antibiotics and steroids for 1-2 weeks; lubricants for dry eye.
Refractive Range
- Myopia: -1.0 D to -10.0 D | Myopic astigmatism up to 3.0 D
- Note: Currently approved only for myopia/myopic astigmatism in the US; not for hypermetropia
Merits
- No flap - eliminates all flap-related complications (dislocation, DLK, striae)
- Better corneal biomechanical stability than LASIK (peripheral anterior stromal collagen networks preserved, contributing ~60% of corneal tensile strength)
- Significantly less dry eye than LASIK due to fewer severed corneal nerves
- Higher patient satisfaction scores than LASIK in head-to-head studies
- Smaller incision reduces infection risk
- Minimal pain postoperatively
- Suitable for patients with mildly thin corneas unsuitable for LASIK
- Preferred for large-pupil patients prone to glare/halos with LASIK
Demerits
- Approved only for myopia/myopic astigmatism - cannot correct hypermetropia
- Steep learning curve for surgeons; initial cases have higher complication rates
- No eye-tracking system during lenticule creation (unlike excimer laser platforms)
- No cyclotorsion compensation - limits precision in high astigmatism
- Slower visual recovery at 1 month compared to LASIK (equalizes by 3 months)
- Lenticule extraction can be technically difficult; incomplete extraction possible
- Enhancement/re-treatment is complex - often requires conversion to PRK
- Higher intraoperative discomfort during tissue manipulation than flap lifting
- Back-scatter and light sensitivity more common at 1 month postop
- Limited customization (no wavefront-guided or topography-guided treatment currently)
6. Phakic Intraocular Lens (pIOL) Implantation
Two main types:
- Anterior chamber iris-claw (Artisan/Verisyse): Clipped to the anterior surface of the iris
- Posterior chamber phakic IOL (ICL / EVO ICL - Implantable Collamer Lens): Placed in the posterior chamber between the iris and the natural crystalline lens
Steps (ICL - most commonly performed today)
- Preoperative assessment - Anterior chamber depth measurement (must be >2.8 mm), endothelial cell count, white-to-white corneal diameter, refraction.
- Laser peripheral iridotomy (LPI) - Created 1-2 weeks before surgery (for non-KS-aquaport designs) to prevent pupillary block glaucoma. Newer EVO ICL has a central aquaport - LPI may be optional.
- Anesthesia - Topical + optional intracameral lidocaine.
- Small corneal incision (2.4-3.2 mm) created at limbus.
- Viscoelastic injection into anterior chamber.
- ICL loading into cartridge injector.
- ICL injection through the incision into the anterior chamber.
- Lens positioning - The ICL is rotated and placed behind the iris in the ciliary sulcus.
- Viscoelastic removal - Thorough aspiration to prevent IOP spike.
- Incision sealed (self-sealing or with suture).
- Postoperative - IOP check at 2 hours; antibiotics + steroids for 4 weeks.
Merits
- Corrects very high myopia (-8 D to -20 D) or hypermetropia - beyond range of laser
- Excellent optical quality; no ablation = no higher-order aberrations from stroma
- Reversible - the lens can be removed or exchanged
- Natural lens is preserved - accommodation maintained
- No corneal tissue removed - useful when cornea is thin or abnormal
- Rapid visual recovery
- No dry eye (corneal nerves untouched)
- EVO ICL: no need for peripheral iridotomy
Demerits
- Intraocular procedure - carries risks of endophthalmitis, cataract, retinal detachment
- Elevated IOP / acute angle closure glaucoma (if undersized vault)
- Endothelial cell loss over time (especially anterior chamber designs)
- Requires adequate anterior chamber depth
- Cataract formation (~3% per patient year for early models, lower with EVO ICL)
- More expensive
- Requires LPI (for older designs)
- Not suitable for patients with shallow anterior chambers, glaucoma, or compromised endothelium
7. Clear Lens Exchange (CLE) / Refractive Lens Exchange (RLE)
Steps
- Identical to standard phacoemulsification cataract surgery (steps as per cataract surgery)
- Corneal incision → viscoelastic → continuous curvilinear capsulorhexis → hydrodissection → phacoemulsification → cortex aspiration → IOL implantation → wound sealing
Merits
- Corrects very high refractive errors (e.g., >+5 D or < -12 D)
- Also corrects presbyopia (with multifocal/EDOF IOLs)
- No future cataract surgery needed
- Stable long-term result
Demerits
- Highest surgical risk among refractive options
- Retinal detachment risk - especially in high myopia (vitreous changes after lens removal)
- Endophthalmitis risk
- Loss of accommodation (if monofocal IOL)
- Dysphotopsia with multifocal IOLs
- Irreversible - natural lens cannot be replaced once removed
8. Radial Keratotomy (RK) / Astigmatic Keratotomy (AK) - Historical
Steps (RK)
- Corneal marking of radial incision pattern
- Diamond blade set to 90-95% corneal depth
- 4-16 radial cuts from optical zone edge to limbus
- Intraoperative pachymetry guidance
Merits
- No laser equipment needed
- Inexpensive
- Effective for mild myopia
Demerits
- Hyperopic shift over time (progressive flattening)
- Diurnal fluctuation in vision (morning myopic, afternoon hyperopic)
- Unpredictable results
- Weak corneal scars - risk of rupture with minor trauma
- Risk of infection, perforation, irregular astigmatism
- Largely abandoned in favor of laser procedures
Comparison Summary Table
| Feature | PRK/LASEK | LASIK | SMILE | pIOL |
|---|---|---|---|---|
| Flap required | No | Yes | No | No |
| Pain | Moderate | Minimal | Minimal | Minimal |
| Visual recovery | 1-4 weeks | 24-48 hrs | 1-2 weeks | 24-48 hrs |
| Corneal thickness | Thin OK | Must be adequate | Moderate | Not required |
| Correction range | Up to -8D / +3D | Up to -10D / +3D | Up to -10D (myopia only) | Up to -20D |
| Dry eye risk | Moderate | High | Low | None |
| Biomechanical stability | Best | Lower | Intermediate | Unchanged |
| Reversibility | No | Limited | No | Yes |
| Enhancements | Simple | Simple | Complex | Possible |
Key Contraindications (All Laser Procedures)
- Unstable refractive error
- Keratoconus or forme fruste keratoconus
- Severe dry eye syndrome
- Active anterior segment disease (herpes simplex, blepharitis)
- Systemic diseases (SLE, rheumatoid arthritis, immunosuppression)
- Corneal thickness insufficient for planned ablation
- High expectations / unrealistic patients (requires thorough counseling)
- Glaucoma (relative - LASIK contraindicated; some surface ablation acceptable)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Ch. 8 (Corneal and Refractive Surgery), pp. 284-303
- The Wills Eye Manual, 8th ed., Section 4.29 (Corneal Refractive Surgery Complications), p. 292
- PMC comparison of LASIK, Trans-PRK, and SMILE - 2025
- StatPearls: SMILE - NIH Bookshelf - Updated Feb 2024
Write a systematic Notes on Lasers in ophthalmology to write in PG exams
lasers in ophthalmology types mechanisms clinical applications PG exam notes 2024
https://www.ncbi.nlm.nih.gov/books/NBK582153
LASERS IN OPHTHALMOLOGY
Systematic Notes for PG Examinations
I. DEFINITION AND BASIC PHYSICS
- Monochromatic - single wavelength
- Coherent - all photons in phase (space and time)
- Collimated - parallel rays with minimal divergence
- High intensity - energy concentrated in a tiny spot
Components of a Laser System
- Active (gain) medium - gas, solid, liquid, or semiconductor
- Energy pump - electrical discharge, flash lamp, chemical reaction
- Optical resonant cavity - two mirrors (one fully reflective, one partially transmissive) that amplify light by repeated pass-through of the medium
Key Parameters
| Parameter | Significance |
|---|---|
| Wavelength (nm) | Determines tissue absorption |
| Power (mW/W) | Energy per unit time |
| Spot size (µm) | Inversely proportional to energy density |
| Exposure time (ms-s) | Determines depth of effect |
| Power density (W/cm²) | Determines tissue interaction type |
| Pulse mode | CW (continuous wave) vs pulsed vs Q-switched |
II. MECHANISMS OF LASER-TISSUE INTERACTION
1. Photochemical Interaction (Photoactivation)
- Mechanism: Low power density + long exposure → photons activate a photosensitive dye → generates reactive oxygen species (ROS) / cytotoxic singlet oxygen
- Temperature rise: Negligible (<1°C)
- Example Lasers: Diode (689 nm), Red light
- Clinical Applications:
- Photodynamic Therapy (PDT) with verteporfin (AMD, CSCR)
- Corneal collagen cross-linking (CXL) with riboflavin + UV-A (380 nm)
2. Photothermal Interaction (Photocoagulation)
- Mechanism: Laser energy absorbed by chromophores (melanin, hemoglobin, xanthophyll) → converted to heat → protein denaturation and tissue coagulation (60-65°C)
- Key Chromophores:
- Melanin: peak absorption at 400-700 nm (green, blue-green, yellow)
- Hemoglobin: peak absorption <600 nm
- Xanthophyll: absorbs blue light (important - avoid blue wavelengths at macula)
- Temperature range: 60-100°C → coagulation; >100°C → vaporization
- Example Lasers: Argon (514 nm green), Frequency-doubled Nd:YAG (532 nm), Diode (810 nm), Krypton (647 nm red)
- Clinical Applications: PRP, focal laser, trabeculoplasty, iridoplasty, cyclophotocoagulation
3. Photoablation
- Mechanism: Ultraviolet photons (high energy) break intramolecular bonds (C-C, C-N) directly → molecular fragmentation and ejection from surface ("cold laser" - no thermal damage to adjacent tissue)
- Characteristic: Extremely precise, 0.25 µm per pulse tissue removal
- Example Laser: Excimer laser (ArF, 193 nm UV)
- Clinical Applications: PRK, LASIK, LASEK, SMILE ablation component, PTK
4. Photodisruption (Plasma-induced Ablation / Ionization)
- Mechanism: Extremely high power density (nanosecond or picosecond pulses) → electric field strips electrons from atoms → plasma formation → shockwave and cavitation bubbles → mechanical tissue rupture
- No thermal damage to adjacent tissue (plasma confines the effect)
- Example Laser: Q-switched Nd:YAG (1064 nm), Femtosecond laser (1053 nm)
- Clinical Applications: Posterior capsulotomy, laser iridotomy, anterior vitreous face disruption, LASIK flap creation
5. Photovaporization
- Mechanism: Mid-infrared wavelengths absorbed by water → rapid vaporization of intracellular fluid → tissue cutting/ablation
- Example Laser: CO₂ laser (10,600 nm), Ho:YAG (2100 nm)
- Clinical Applications: Lid lesion ablation, scleroplasty (Holmium YAG)
III. TYPES OF LASERS USED IN OPHTHALMOLOGY
| Laser | Wavelength | Medium | Mode | Primary Mechanism |
|---|---|---|---|---|
| Argon | 488 nm (blue) / 514 nm (green) | Gas (Argon) | CW | Photothermal |
| Frequency-doubled Nd:YAG | 532 nm (green) | Solid | Pulsed | Photothermal |
| Krypton | 647 nm (red) | Gas | CW | Photothermal |
| Diode | 810 nm (infrared) | Semiconductor | CW | Photothermal |
| Nd:YAG | 1064 nm (infrared) | Solid (Nd:YAG crystal) | Q-switched pulsed | Photodisruption |
| Femtosecond (FS) | 1053 nm (infrared) | Solid (Nd:glass) | Ultrashort pulsed | Photodisruption |
| Excimer (ArF) | 193 nm (UV) | Gas (Ar + F₂) | Pulsed | Photoablation |
| Diode (PDT) | 689 nm (red) | Semiconductor | CW | Photochemical |
| UV-A (CXL) | 365-380 nm | Solid/LED | CW | Photochemical |
| CO₂ | 10,600 nm (IR) | Gas | CW/pulsed | Photovaporization |
IV. LASER DELIVERY SYSTEMS
- Slit-lamp delivery - Most common; power, spot size, and exposure time easily modulated; used for anterior segment and posterior segment (with fundus contact lens)
- Indirect ophthalmoscope delivery - Fiber optic cable delivers diode or argon laser to the peripheral retina; spot size depends on condensing lens power (e.g., 20D, 28D); used for retinal breaks, ROP
- Endophotocoagulation - Fiber optic probe introduced through pars plana during vitrectomy; delivers argon green or diode laser intraoperatively for PDR, ROP
- Transscleral delivery - For cyclophotocoagulation; probe applied to sclera overlying ciliary body; used in refractory glaucoma
V. CLINICAL APPLICATIONS - ANTERIOR SEGMENT
A. CORNEA
1. Excimer Laser (Refractive Surgery) - 193 nm
| Procedure | Full Name | Epithelium Handling |
|---|---|---|
| PRK | Photorefractive Keratectomy | Removed entirely |
| LASEK | Laser-Assisted Sub-Epithelial Keratectomy | Chemical flap (alcohol) |
| Epi-LASIK | Epithelial LASIK | Mechanical flap (epi-keratome) |
| LASIK | Laser-Assisted In Situ Keratomileusis | Stromal flap (microkeratome or FS laser) |
| SMILE | Small Incision Lenticule Extraction | No flap; intrastromal lenticule extracted via 2-3 mm incision |
| Trans-PRK | Transepithelial PRK | Single-step: epithelium + stroma ablated together |
2. PTK (Phototherapeutic Keratectomy) - Excimer 193 nm
- Indication: Corneal dystrophies (Reis-Bucklers, granular, lattice), recurrent corneal erosion, superficial corneal scars, band keratopathy
- Mechanism: Photoablation smooths irregular corneal surface
- Note: Can induce hyperopic shift (ablating central stroma more than periphery)
3. Corneal Collagen Cross-linking (CXL) - UV-A 365 nm + Riboflavin
- Indication: Keratoconus (progressive), post-LASIK ectasia
- Mechanism: UV-A activates riboflavin → ROS → covalent cross-links between collagen fibrils → stiffens corneal stroma
- Standard (Dresden) Protocol: Riboflavin 0.1% drops for 30 min + UV-A 3 mW/cm² for 30 min (total fluence 5.4 J/cm²)
- Goal: Halt progression (not to reverse keratoconus)
B. GLAUCOMA LASERS
1. Laser Peripheral Iridotomy (LPI)
- Laser: Nd:YAG (1064 nm) - primary; Argon pre-treatment to thin iris first
- Mechanism: Photodisruption creates a full-thickness hole in peripheral iris
- Indication: Acute angle-closure glaucoma, chronic angle-closure, occludable angles, phacomorphic glaucoma, pigment dispersion syndrome (controversial)
- Technique:
- Pretreat with pilocarpine 2% (constricts iris, stretches it thin)
- Use Abraham or Wise lens (66D button for Nd:YAG)
- Superior peripheral iris (covered by upper lid - prevents monocular diplopia)
- Nd:YAG: 1-3 pulses, 4-8 mJ; Argon first if thick/dark iris: 200-400 mW, 200 ms, 50 µm
- Endpoint: visible perforation with "gush" of pigment into anterior chamber
- Complications: IOP spike (give apraclonidine pre/post), lens damage, corneal endothelial burns, monocular diplopia, hyphema, re-closure
2. Laser Trabeculoplasty
- Laser: Argon 514 nm
- Parameters: 50 µm spot, 100 mW, 100 ms; 50 spots over 180° (at anterior TM junction)
- Mechanism: Thermal burns → scarring → mechanical stretching of TM spaces + biological stimulation of outflow
- IOP reduction: 25-30%
- Limitation: TM sustains thermal damage - repeat treatment of limited benefit
- Complications: PAS formation, IOP spike (acute), CME, anterior uveitis
- Laser: Frequency-doubled Q-switched Nd:YAG (532 nm)
- Parameters: 400 µm spot (larger than ALT), 0.3-1.0 mJ, 3 ns pulse; 100 spots over 360° or 50 spots over 180°
- Mechanism: Selectively targets melanin-rich TM cells only (non-pigmented structures unharmed); stimulates macrophage recruitment, TM cell division, extracellular matrix remodeling
- LiGHT Trial (2019): SLT as first-line = superior to drops in preventing progression at 6 years; 80% drop-free at 3 years
- IOP reduction: 10-40%; 25% typical; repeatable (no thermal damage to TM)
- Advantages over ALT: Repeatable, less PAS, equivalent IOP reduction
- Complications: Transient anterior uveitis, IOP spike (avoid overtreating heavily pigmented angles), rare corneal endothelial damage, herpes simplex reactivation
- Uses ultrashort pulses; no visible tissue reaction; comparable results; newer modality
3. Cyclophotocoagulation (CPC)
- Laser: Diode (810 nm) - preferred; Nd:YAG (1064 nm) also used
- Mechanism: Photothermal coagulation of ciliary body epithelium → reduces aqueous production
- Indication: Refractory glaucoma (neovascular, uveitic, traumatic, congenital); last resort
- Approaches:
- Trans-scleral CPC (TSCP): Probe placed 1.5 mm posterior to limbus; 2000 mW, 2-3 sec; 16-18 spots over 270°
- Endoscopic CPC (ECP): Direct visualization via endoscope during vitrectomy/cataract
- Micropulse trans-scleral CPC: Less destructive; subthreshold pulses; emerging
- Complications: Hypotony, phthisis bulbi, sympathetic ophthalmia (rare with diode), pain, uveitis
4. Laser Iridoplasty (Peripheral Iridoplasty / GPAC laser)
- Laser: Argon 514 nm
- Mechanism: Thermal burns to peripheral iris → contraction → pulls iris away from angle
- Indication: Plateau iris syndrome, appositional angle closure unresponsive to LPI, prior to ALT
- Parameters: Large spot (500 µm), low power (200-400 mW), long duration (0.5 sec); 20-24 spots per eye
5. Laser Suture Lysis
- Laser: Argon
- Post-trabeculectomy - selectively lyses tight scleral flap sutures to increase aqueous filtration
VI. CLINICAL APPLICATIONS - POSTERIOR SEGMENT
A. DIABETIC RETINOPATHY
1. Panretinal Photocoagulation (PRP) / Scatter Laser
- Laser: Argon green (514 nm) or diode (810 nm)
- Indication: Proliferative diabetic retinopathy (PDR), severe NPDR (high-risk features per DRS)
- DRS High-Risk Characteristics (treat immediately with PRP):
- NVD > 1/3-1/4 disc area
- NVD any size + vitreous/preretinal hemorrhage
- NVE ≥ 1/2 disc area + vitreous/preretinal hemorrhage
- Mechanism: Ablates hypoxic peripheral retina → reduces VEGF production → regression of neovascularization
- Parameters: 500 µm spot size (200-500), 0.1 sec, 200-300 mW; 1200-1600 spots placed 1 burn-width apart; 2-3 sessions
- DRCR.net Protocol S / CLARITY: Intravitreal anti-VEGF (ranibizumab/aflibercept) as effective as PRP at 5 years - now a valid alternative
- Complications: Visual field loss (may affect driving), night vision impairment, reduced color vision, exacerbation of macular edema (fractionate over 2-3 sessions to reduce risk), reduced accommodation
2. Focal/Grid Laser for Diabetic Macular Edema (DME)
- Laser: Argon green or yellow (577 nm) or diode
- ETDRS guidelines: Treat "clinically significant macular edema" (CSME)
- Focal: Direct burns to leaking microaneurysms (50-100 µm spot, 0.1 sec)
- Grid: Pattern of mild burns to areas of diffuse leakage/non-perfusion (avoiding FAZ)
- Note: Anti-VEGF injections are now first-line for center-involving DME (DRCR.net Protocol T); focal/grid laser reserved for non-center-involving CSME or as adjunct
- Micropulse/Subthreshold Laser: Emerging as effective as conventional laser with no tissue damage (Kanski 10th ed); onset of action slower but avoids thermal scars
B. RETINAL BREAKS AND DETACHMENT
1. Laser Barricade / Retinopexy
- Laser: Argon green or diode (via slit-lamp or indirect ophthalmoscope)
- Indication: Symptomatic retinal tears, horseshoe tears, lattice degeneration with breaks; prophylaxis before retinal detachment occurs
- Mechanism: Photothermal burns create chorioretinal adhesion (inflammatory reaction matures in 10-14 days)
- Technique: 2-3 rows of confluent burns surrounding the tear; treat fellow eye if symptomatic
- Cannot treat: Established retinal detachment (needs surgery)
C. RETINAL VEIN OCCLUSIONS (BRVO / CRVO)
- Branch RVO (BRVO): Grid laser to areas of macular edema (BVOS); sector PRP if NVE present; anti-VEGF now preferred first-line for macular edema
- Central RVO (CRVO): PRP if iris neovascularization (rubeosis) or NVA/NVG develops (to reduce VEGF); anti-VEGF for macular edema
D. AGE-RELATED MACULAR DEGENERATION (AMD)
1. Photodynamic Therapy (PDT) with Verteporfin
- Laser: Diode 689 nm (red light)
- Drug: Verteporfin (benzoporphyrin derivative) - photosensitizer
- Mechanism: IV verteporfin (6 mg/m²) accumulates in rapidly dividing CNV endothelium → activated by 689 nm laser (50 J/cm², 83 sec) → singlet oxygen → selective thrombosis of CNV without damaging adjacent retina
- Indication: Classic subfoveal CNV in AMD, pathological myopia, angioid streaks, POHS; largely replaced by anti-VEGF but still used in CSCR (half-fluence PDT)
- Note: Patient must avoid sunlight for 48 hours after injection (risk of skin phototoxicity)
2. Thermal Laser - rarely used now; confined to extrafoveal/juxtafoveal classic CNV
E. CENTRAL SEROUS CHORIORETINOPATHY (CSCR)
- Focal laser: Direct treatment of leaking point when outside FAZ (argon green/yellow)
- Half-fluence PDT (689 nm, 25 J/cm²): Preferred for chronic CSCR; reduces choroidal hyperpermeability with lower risk of RPE damage
F. RETINOPATHY OF PREMATURITY (ROP)
- Laser: Diode (810 nm) via indirect ophthalmoscope
- Indication: Type 1 ROP (Zone I any stage with plus, Zone I Stage 3, Zone II Stage 2-3 with plus)
- Treatment: Near-confluent laser spots to entire avascular peripheral retina (anterior to ridge)
- Preferred over cryotherapy (lower rate of anterior segment complications, unfavorable structural outcomes)
- Administer within 48-72 hours of threshold ROP diagnosis
- Bevacizumab/ranibizumab alternative for Zone I and posterior Zone II ROP
G. TRANSPUPILLARY THERMOTHERAPY (TTT)
- Laser: Diode 810 nm, large spot (0.8-3 mm), low power, long duration (60 sec)
- Mechanism: Subthreshold heating of RPE and choroid
- Indication: Choroidal melanoma (adjunct/definitive for small tumors), some CNV
- Now largely replaced by anti-VEGF and plaque brachytherapy for melanoma
VII. DIAGNOSTIC LASER APPLICATIONS
| Modality | Laser Type | Application |
|---|---|---|
| OCT (Optical Coherence Tomography) | Near-infrared 840 nm | Retinal, corneal, optic nerve imaging; gold standard for macular diseases |
| SLO (Scanning Laser Ophthalmoscope) | He-Ne 632 nm or diode | Fundus imaging, microperimetry, fluorescein angiography |
| HRT (Heidelberg Retinal Tomograph) | Diode 670 nm | Optic nerve head 3D imaging; glaucoma monitoring |
| Confocal Microscopy | He-Ne 543 nm / 488 nm | Corneal layer imaging (endothelium, epithelium) |
| Laser Interferometry | Near-IR | Biometry (IOL power calculation - e.g., IOLMaster) |
VIII. LASER IN CATARACT SURGERY
Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Laser: Femtosecond laser (1053 nm)
- Steps replaced by laser:
- Corneal incisions (main + side port)
- Anterior capsulotomy (capsulorhexis) - more precise than manual
- Lens fragmentation (softens nucleus - reduces phacoemulsification ultrasound energy)
- Limbal relaxing incisions for astigmatism correction
- Advantage: Greater precision in capsulotomy, reduced cumulative dispersed energy (CDE), better IOL centration
- Disadvantage: Higher cost, longer setup time, not proven to improve final visual outcomes over manual phaco in RCTs
Nd:YAG Posterior Capsulotomy
- Laser: Q-switched Nd:YAG 1064 nm
- Indication: Posterior capsule opacification (PCO) - most common late complication of cataract surgery; occurs in 5-10% of cases (Bailey & Love)
- Mechanism: Photodisruption creates central opening in opacified posterior capsule
- Parameters: 1-3 mJ per pulse; aim for minimum energy; 3 o'clock pattern or + pattern
- Technique: Focus posterior to capsule (creates forward shockwave); use Abraham lens
- IOP: Give apraclonidine pre/post; measure IOP at 1 hour
- Complications: IOP spike (most common), pitting/cracking of IOL, CME, retinal detachment (0.08-3.6%), hyphema, vitreous prolapse, endophthalmitis (very rare)
- Contraindication: Active uveitis, silicone IOL (Nd:YAG causes permanent pitting)
IX. LASER SAFETY
Wavelength and Ocular Hazard Zones
| Wavelength Range | Primary Ocular Hazard |
|---|---|
| UV (<400 nm) | Corneal/conjunctival damage (photokeratitis) |
| Visible (400-780 nm) | Retinal damage (photochemical + thermal) |
| Near-IR (780-1400 nm) | Retinal damage (transmitted to retina) |
| Mid-IR (1400-3000 nm) | Lens + corneal damage |
| Far-IR (>3000 nm) | Corneal damage only |
Safety Measures
- Appropriate protective goggles (wavelength-specific optical density)
- Warning signs on laser room doors
- Laser power meter calibration before each session
- Minimal effective power principle
- Anti-reflection coatings on optics
- Topical anesthesia and patient fixation to avoid movement
- Laser classification system (Class I-IV; ophthalmic lasers are Class IIIb or IV)
Laser Complications (General)
- Inadvertent foveal burn (catastrophic)
- IOP spike (especially Nd:YAG, SLT)
- Corneal endothelial damage
- Lens damage (crystalline or IOL)
- Uveitis
- CME
- Retinal detachment (post Nd:YAG capsulotomy)
X. HIGH-YIELD EXAM SUMMARY
| Laser | Wavelength | Mechanism | Key Use |
|---|---|---|---|
| Argon | 514 nm (green) | Photothermal | PRP, ALT, iridoplasty, barricade |
| Freq-doubled Nd:YAG | 532 nm | Photothermal | SLT (first-line glaucoma) |
| Diode | 810 nm | Photothermal | CPC, ROP, PDT activation (689 nm variant) |
| Nd:YAG (Q-switched) | 1064 nm | Photodisruption | Capsulotomy, LPI, vitreolysis |
| Femtosecond | 1053 nm | Photodisruption | LASIK flap, SMILE, FLACS |
| Excimer (ArF) | 193 nm | Photoablation | PRK, LASIK, PTK |
| Diode (689 nm) | 689 nm | Photochemical | PDT (verteporfin, AMD/CSCR) |
| UV-A + riboflavin | 365 nm | Photochemical | CXL for keratoconus |
Must-Know One-Liners for Viva / Short Notes
- LASER = Light Amplification by Stimulated Emission of Radiation
- LiGHT trial: SLT > drops as first-line in POAG/OHT (2019)
- Nd:YAG capsulotomy: Q-switched, 1064 nm, photodisruption; complication = IOP spike + retinal detachment
- SLT: 532 nm, selectively targets melanin in TM, repeatable (no thermal damage)
- PRP: 1200-1600 burns, ablates hypoxic retina, reduces VEGF, mainstay of PDR
- PDT: Verteporfin (IV) + 689 nm diode; avoid sunlight 48 hrs post-treatment
- CXL: UV-A 365 nm + riboflavin → corneal collagen cross-links → halts keratoconus
- Excimer 193 nm: "Cold laser" - photoablation, no thermal spread, 0.25 µm/pulse precision
- ROP laser: Diode via BIO, within 48-72 hrs of threshold, avascular retina ablated
- Micropulse/subthreshold laser: No visible burn, RPE stimulation only - emerging for DME, CSCR, SLT
- FLACS: Femtosecond laser for capsulotomy + nucleus fragmentation + incisions in cataract surgery
- Contraindication to Nd:YAG capsulotomy: Silicone IOL (pits permanently), active uveitis
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. - Chapters 8, 11, 13
- The Wills Eye Manual, 8th ed. - Sections 4.29, 8.2, Chapter 11
- Bailey & Love's Short Practice of Surgery, 28th ed. - Chapter on Lasers in Ophthalmology
- StatPearls: Laser Principles in Ophthalmology - NIH Bookshelf
- eOphtha: Lasers in Ophthalmology - A Concise Guide for Postgraduates
Classification of laser for ophthalmology on basis of its use on different anatomical structure from antrior I.e cornea to posterior i.e retina
CLASSIFICATION OF LASERS IN OPHTHALMOLOGY
Based on Anatomical Site (Anterior → Posterior)
OVERVIEW CLASSIFICATION TABLE
| Anatomical Site | Laser Procedure | Laser Type | Wavelength | Mechanism |
|---|---|---|---|---|
| Cornea | PRK, LASEK, LASIK | Excimer (ArF) | 193 nm | Photoablation |
| Cornea | PTK | Excimer (ArF) | 193 nm | Photoablation |
| Cornea | CXL | UV-A | 365-380 nm | Photochemical |
| Cornea | LASIK flap / SMILE | Femtosecond | 1053 nm | Photodisruption |
| Iris | Peripheral Iridotomy | Nd:YAG / Argon | 1064 / 514 nm | Photodisruption / Photothermal |
| Iris | Iridoplasty | Argon | 514 nm | Photothermal |
| Iris | Pupilloplasty | Argon | 514 nm | Photothermal |
| Trabecular meshwork | ALT / SLT / MLT | Argon / 532 nm Nd:YAG | 514 / 532 nm | Photothermal |
| Sclera | Laser suture lysis | Argon | 514 nm | Photothermal |
| Sclera | Laser scleroplasty | Holmium:YAG | 2100 nm | Photovaporization |
| Ciliary body | Cyclophotocoagulation | Diode / Nd:YAG | 810 / 1064 nm | Photothermal |
| Anterior vitreous | Laser vitreolysis | Nd:YAG | 1064 nm | Photodisruption |
| Lens/Capsule | Posterior capsulotomy | Nd:YAG | 1064 nm | Photodisruption |
| Lens (cataract surgery) | FLACS | Femtosecond | 1053 nm | Photodisruption |
| Retina | PRP (PDR) | Argon / Diode | 514 / 810 nm | Photothermal |
| Retina | Focal/Grid laser (DME) | Argon / Yellow | 514 / 577 nm | Photothermal |
| Retina | Laser barricade (tears) | Argon / Diode | 514 / 810 nm | Photothermal |
| Retina | ROP laser | Diode (BIO) | 810 nm | Photothermal |
| Retina/Choroid | PDT (AMD/CSCR) | Diode | 689 nm | Photochemical |
| Retina | TTT | Diode | 810 nm | Photothermal |
| Retina | Micropulse/Subthreshold | Diode | 810 nm | Photothermal (subthreshold) |
1. CORNEA
A. Refractive Laser Procedures
| Procedure | What is done | Key Feature |
|---|---|---|
| PRK (Photorefractive Keratectomy) | Epithelium removed → stroma ablated | No flap; best for thin corneas |
| LASEK | Epithelial flap (alcohol) → stroma ablated → flap replaced | Epithelium preserved as biological bandage |
| Epi-LASIK | Epithelial flap (epi-keratome) → stroma ablated | Mechanical separation; avoids alcohol toxicity |
| LASIK | Stromal flap (microkeratome) → stroma ablated → flap replaced | Fastest recovery; most performed worldwide |
| Trans-PRK | Single-step: epithelium + stroma ablated together | No mechanical epithelial removal; latest evolution |
- FS-LASIK: Femtosecond laser replaces microkeratome for LASIK flap creation - more precise, thinner, predictable flap
- SMILE: Femtosecond creates intrastromal refractive lenticule → extracted via 2-3 mm incision; no flap at all; better corneal biomechanical stability; less dry eye
B. PTK (Phototherapeutic Keratectomy)
- Indications:
- Corneal dystrophies - Reis-Bucklers, granular, lattice, Fuchs (superficial)
- Recurrent corneal erosion syndrome (RCES)
- Superficial corneal scars and opacities
- Band keratopathy
- Goal: Smooth irregular anterior corneal surface
- Note: Can induce hyperopic shift (ablates central stroma) - plan with refraction
C. Corneal Collagen Cross-linking (CXL)
- Indications: Progressive keratoconus, post-LASIK ectasia, pellucid marginal degeneration
- Dresden Protocol:
- Epithelial debridement (epi-off) - 9 mm zone
- Riboflavin 0.1% drops every 3 min × 30 min (soaks stroma)
- UV-A at 3 mW/cm² × 30 min = total fluence 5.4 J/cm²
- Mechanism: UV-A activates riboflavin → singlet oxygen → covalent cross-links between collagen fibrils → stiffens and strengthens corneal stroma
- Goal: Halt progression (not reverse); demarcation line at ~300 µm depth on OCT confirms adequate treatment
- Epi-on CXL (transepithelial): Less effective; riboflavin penetration suboptimal; under study
2. CONJUNCTIVA / SCLERA
A. Laser Suture Lysis
- Post-trabeculectomy - selectively burns tight scleral flap sutures to increase aqueous drainage through the bleb
- Done through conjunctiva using Hoskins or Zeiss lens
- Performed in early postoperative period (before sutures become encapsulated)
B. Laser Scleroplasty
- Indication: Primary open-angle glaucoma (POAG) - alternative drainage procedure
- Creates channels through sclera for aqueous drainage
3. IRIS
A. Laser Peripheral Iridotomy (LPI)
- Indications:
- Acute angle-closure glaucoma (both eyes treated)
- Chronic angle closure
- Occludable angles (prophylactic)
- Phacomorphic glaucoma
- Iris bombé
- Fellow eye in acute ACG
- Technique:
- Pilocarpine 2% instilled 1 hour before (thins iris, opens angle)
- Abraham lens (66D button amplifies beam)
- Site: Superior peripheral iris at 11 or 1 o'clock (covered by upper lid)
- If thick/dark iris: Argon pre-treatment (500 µm, 200-400 mW, 0.2 sec) to thin the stroma first, then Nd:YAG (1-3 pulses, 4-8 mJ) to perforate
- Endpoint: Visible gush of pigment + aqueous jet ("champagne bubbles")
- Complications: IOP spike (give apraclonidine 1% before + after), hyphema, lens damage, corneal burn, monocular diplopia (if placed in visual axis), re-closure
B. Laser Iridoplasty (Peripheral/Gonioscopic Laser Iridoplasty)
- Indications:
- Plateau iris syndrome (most important indication)
- Appositional angle closure unresponsive to LPI
- Pupillary block unresponsive to LPI
- Prior to argon laser trabeculoplasty (to widen angle)
- Mechanism: Thermal contraction burns to far peripheral iris → iris stroma contracts → physically pulls iris away from angle
- Parameters: Large spot (500 µm), long duration (0.5 sec), low power (200-400 mW); ~20-24 spots per eye
C. Laser Pupilloplasty
- Indications:
- Break peripheral anterior synechiae (PAS)
- Relieve appositional angle closure
- Reposition a decentred or distorted pupil post-surgery
- Mechanism: Thermal burns to iris sphincter or stroma → contraction repositions pupil
4. TRABECULAR MESHWORK (Angle / Drainage)
A. Argon Laser Trabeculoplasty (ALT)
- Indications: POAG refractory to medical therapy, pseudoexfoliation glaucoma, pigmentary glaucoma
- Parameters: 50 µm spot, 100 ms, 100-120 mW; 50 spots over 180° (at junction of anterior and posterior TM)
- IOP reduction: 25-30% acutely; declines over years
- Mechanism: Thermal burns → mechanical stretching of TM spaces + biological stimulation
- Limitation: Non-repeatable (thermal damage to TM); concern about adverse effect on subsequent filtration surgery
- Complications: PAS, IOP spike, CME, anterior uveitis
B. Selective Laser Trabeculoplasty (SLT) ⭐ First-line per LiGHT Trial
- Indications: POAG (now recommended as first-line), ocular hypertension, pseudoexfoliation, pigmentary glaucoma
- Parameters: Large spot (400 µm), very short pulse (3 nanoseconds), low energy (0.3-1.0 mJ); 100 spots over 360° or 50 over 180°
- Key difference from ALT: Selectively targets melanin-pigmented TM cells only; non-pigmented cells and surrounding structures unharmed
- LiGHT Trial (2019): SLT as first-line treatment - 80% drop-free at 3 years; less disease progression than drops at 6 years
- Advantage: Repeatable (no thermal damage); can be re-treated
- IOP reduction: 10-40%; ~25% typical
- Mechanism (incompletely understood): TM cell division stimulation, macrophage recruitment, extracellular matrix remodeling
- Complications: Transient uveitis, IOP spike (avoid over-treating heavily pigmented angles - risk of endothelial damage), herpes simplex reactivation, rare CME
C. Micropulse Laser Trabeculoplasty (MLT)
- Short bursts of energy; no visible tissue reaction; targets smaller area than SLT
- Emerging modality; comparable IOP reduction; benign safety profile; potential to replace ALT/SLT
5. CILIARY BODY
Cyclophotocoagulation (CPC)
- Indications: Refractory glaucoma (last resort after failed medical + surgical treatment):
- Neovascular glaucoma (NVG)
- Uveitic glaucoma
- Traumatic glaucoma
- Congenital/developmental glaucoma (failed trabeculotomy)
- Blind painful eye
- Mechanism: Laser energy absorbed by pigmented ciliary epithelium → coagulation → reduced aqueous humor production
- Approaches:
- Trans-scleral CPC (TSCP): Most common; contact probe placed 1.2-1.5 mm posterior to limbus; 2000 mW, 2 sec; ~18 spots over 270° (sparing 3 and 9 o'clock - to protect long posterior ciliary vessels); G-probe or MicroPulse probe
- Endoscopic CPC (ECP): Direct visualization via endoscope (during combined cataract/vitreous surgery); most precise; lowest risk of hypotony
- Micropulse TSCP: Subthreshold repeated pulses; less destructive; emerging as preferred modality
- Complications: Hypotony (most feared), phthisis bulbi, pain, uveitis, sympathetic ophthalmia (rare with diode), hyphema, visual loss
6. ANTERIOR VITREOUS FACE
Laser Vitreolysis / Anterior Hyaloid Disruption
- Indication: Malignant glaucoma (aqueous misdirection syndrome) - to release aqueous trapped behind vitreous face
- Also: Laser vitreolysis for symptomatic floaters (Nd:YAG disrupts vitreous strands)
- Mechanism: Photodisruption breaks anterior hyaloid face → releases aqueous from vitreous compartment
7. CRYSTALLINE LENS / POSTERIOR CAPSULE
A. Nd:YAG Posterior Capsulotomy
- Indication: Posterior capsule opacification (PCO) - most common late complication of cataract surgery; incidence 5-10% (Bailey & Love)
- Clinical features of PCO: Gradual painless visual deterioration, glare, reduced contrast months to years after cataract surgery
- Technique:
- Dilate pupil (tropicamide 1%)
- Apraclonidine 1% instilled before (prevents IOP spike)
- Abraham/capsulotomy lens applied
- Focus just posterior to the capsule (shockwave propagates forward)
- Minimum energy used: start at 1 mJ; titrate up
- Create central opening: plus (+) pattern or circular pattern; ~3-4 mm diameter
- Avoid: Focusing on IOL surface (pits the optic permanently - especially silicone IOLs)
- Post-procedure: IOP check at 1 hour; apraclonidine continued; anti-inflammatory drops
- Complications (in order of frequency):
- IOP spike (most common - usually transient)
- IOL pitting/damage (especially silicone IOLs - absolute contraindication with silicone)
- Cystoid macular edema (CME)
- Retinal detachment (0.08-3.6% - higher in myopes, vitrectomized eyes)
- Hyphema
- Vitreous prolapse into anterior chamber
- Endophthalmitis (very rare)
- Contraindications: Active uveitis, silicone IOL, inadequate pupil dilation, patient non-compliance
B. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Roles in cataract surgery:
- Capsulorhexis (anterior capsulotomy): More precise, circular, reproducible than manual; better IOL centration
- Lens/nucleus fragmentation: Softens nucleus → less phacoemulsification ultrasound energy needed → less endothelial damage
- Corneal incisions (main wound + side ports)
- Limbal relaxing incisions (LRI) for astigmatism
- Advantages: Precision, reproducibility, reduced CDE (cumulative dispersed energy)
- Limitation: Higher cost; no proven superior final visual outcome over manual phaco in RCTs; adds time; suction-related IOP elevation
8. RETINA AND VITREORETINAL
A. Panretinal Photocoagulation (PRP) / Scatter Laser
- Indications:
- PDR (Proliferative Diabetic Retinopathy) - DRS high-risk characteristics
- Proliferative sickle cell retinopathy
- Proliferative retinopathy of BRVO/CRVO with NVI/NVA
- Severe NPDR (prior to high-risk PDR in some cases)
- DRS High-Risk Characteristics (treat immediately):
- NVD ≥ 1/3-1/4 disc area
- NVD of any size + vitreous or preretinal hemorrhage
- NVE ≥ 1/2 disc area + vitreous or preretinal hemorrhage
- Mechanism: Ablates hypoxic ischemic peripheral retina → reduces VEGF secretion → regression of neovascularization
- Parameters: 500 µm spot, 100-200 ms, 200-300 mW (gray-white burn); 1200-1600 spots, 1 burn-width apart; spare 2 disc diameters around optic disc and 2 DD temporal to fovea; administered over 2-3 sessions
- Diode (810 nm) advantage: Better penetration through media opacity and hemorrhage; less macular edema induction
- Complications: Visual field constriction (may affect driving), night blindness, reduced color vision, exacerbation of macular edema, transient myopia, choroidal detachment, decreased accommodation
B. Focal / Grid Laser for Diabetic Macular Edema (DME)
- ETDRS Indication: Clinically Significant Macular Edema (CSME):
- Thickening ≥ 500 µm from center of fovea
- Hard exudates ≥ 500 µm from center + adjacent thickening
- Thickening ≥ 1 disc area, any portion within 1 DD of fovea
- Focal laser: Direct burns to leaking microaneurysms (50-100 µm spot, 100 ms)
- Grid laser: Scattered pattern over areas of diffuse non-focal leakage; avoids FAZ (500 µm from foveal center); creates mild burns
- Current role: Anti-VEGF (ranibizumab, aflibercept, faricimab) is now first-line for center-involving DME (DRCR.net Protocol T); focal/grid reserved for non-center-involving CSME
- Yellow 577 nm advantage: Not absorbed by xanthophyll pigment at macula → safer for perifoveal treatment
- Micropulse/Subthreshold laser (810 nm diode): No visible burn; RPE stimulated without thermal coagulation; as effective as conventional laser with no tissue damage (Kanski 10th ed)
C. Laser Barricade (Prophylactic Retinopexy)
- Indications:
- Symptomatic horseshoe (flap) tears
- Symptomatic operculated holes
- Lattice degeneration with breaks
- Atrophic holes in symptomatic eyes
- Prophylaxis post-trauma or in highly myopic eyes
- Mechanism: Photothermal burns → inflammatory reaction → chorioretinal adhesion matures in 10-14 days (critical period - activity restriction)
- Technique: 2-3 rows of confluent white burns surrounding and encircling the tear (do not treat bridging vessel - risk of hemorrhage)
- Cannot treat: Established retinal detachment with subretinal fluid (needs surgery)
D. ROP Laser Treatment
- Indication: Type 1 ROP:
- Zone I: Any stage with plus disease
- Zone I: Stage 3 without plus disease
- Zone II: Stage 2 or 3 with plus disease
- Treatment: Near-confluent laser spots covering entire avascular peripheral retina anterior to the ridge
- Timing: Within 48-72 hours of diagnosis of threshold/Type 1 ROP
- Preferred over cryotherapy: Fewer anterior segment complications, better structural outcomes
- Delivery via indirect ophthalmoscope: Spot size depends on condensing lens power (20D, 28D, or 2.2 Volk)
- Adjunct/Alternative: Anti-VEGF (bevacizumab, ranibizumab) for Zone I and posterior Zone II ROP - faster regression; but risk of recurrence and systemic effects
E. Laser for Retinal Vein Occlusions
- BVOS criteria: Grid laser to sectors of macular edema persisting >3 months if VA ≤ 20/40 (now largely replaced by anti-VEGF - BRAVO trial)
- Sector PRP: If NVE/NVD develops in sector of BRVO
- PRP: Indicated when iris neovascularization (rubeosis iridis) / NVA / NVG develops (to prevent NVG)
- Macular grid: Limited efficacy (CVOS); anti-VEGF now preferred
F. Photodynamic Therapy (PDT)
- Mechanism:
- IV verteporfin (6 mg/m² over 10 min) → accumulates preferentially in rapidly proliferating CNV endothelium
- 15 min after injection: 689 nm diode laser applied over CNV (50 J/cm² at 600 mW/cm² for 83 seconds)
- Activated verteporfin → singlet oxygen → selective thrombosis and occlusion of CNV without RPE/retinal damage
- Indications:
- Classic subfoveal CNV in AMD (now largely superseded by anti-VEGF)
- Myopic CNV
- Angioid streaks with CNV
- Presumed Ocular Histoplasmosis Syndrome (POHS)
- Half-fluence PDT (25 J/cm²): Standard treatment for chronic CSCR (reduces choroidal hyperpermeability)
- Post-procedure precaution: Avoid sunlight and bright indoor light for 48 hours (risk of severe skin phototoxicity)
- Complications: Visual disturbance, photosensitivity, infusion-related back pain, subretinal hemorrhage
G. Transpupillary Thermotherapy (TTT)
- Parameters: Very large spot (0.8-3.0 mm), low power (100-800 mW), long duration (60 sec) → subthreshold temperature rise (10°C)
- Indications: Small choroidal melanoma (adjunct to brachytherapy), occult CNV in AMD, some retinal tumors
- Mechanism: Mild hyperthermia → apoptosis of tumor cells / CNV endothelium without overt coagulation
- Largely replaced by anti-VEGF for CNV and plaque brachytherapy for melanoma
DIAGNOSTIC LASER APPLICATIONS (Bonus - Anterior to Posterior)
| Structure | Modality | Laser | Purpose |
|---|---|---|---|
| Cornea | Confocal microscopy | He-Ne 543 nm | Layer-by-layer corneal imaging |
| Anterior segment | OCT (AS-OCT) | Near-IR 840 nm | Angle, cornea, lens imaging |
| Lens | Laser biometry (IOLMaster) | Near-IR 780 nm | Axial length for IOL power |
| Optic nerve | HRT (Heidelberg Retinal Tomograph) | Diode 670 nm | Optic disc 3D mapping for glaucoma |
| Retina | OCT | Near-IR 840 nm | Macular, RNFL imaging; gold standard |
| Retina | SLO (Scanning Laser Ophthalmoscope) | He-Ne 632 nm | Fundus imaging, angiography |
| Retina | FFA / ICGA delivery | Blue 488 nm / IR 795 nm | Fluorescein / ICG angiography via SLO |
QUICK REVISION CARD
CORNEA → Excimer (193 nm) = PRK/LASIK/PTK [photoablation]
FS laser (1053 nm) = SMILE/FS-LASIK flap [photodisruption]
UV-A (365 nm) + Riboflavin = CXL [photochemical]
IRIS → Nd:YAG (1064 nm) = LPI [photodisruption]
Argon (514 nm) = Iridoplasty, Pupilloplasty [photothermal]
ANGLE (TM) → SLT (532 nm) = First-line POAG [selective photothermal]
ALT (514 nm) = POAG [photothermal]
SCLERA → Argon = Suture lysis [photothermal]
CILIARY BODY → Diode (810 nm) = CPC [photothermal] - refractory glaucoma
ANT. VITREOUS → Nd:YAG (1064 nm) = Vitreolysis / malignant glaucoma
LENS/CAPSULE → Nd:YAG (1064 nm) = YAG capsulotomy [photodisruption]
FS laser (1053 nm) = FLACS [photodisruption]
RETINA → Argon/Diode = PRP (PDR), Focal/Grid (DME), Barricade (tears)
Diode BIO (810 nm) = ROP [photothermal]
Diode (689 nm) + Verteporfin = PDT (AMD/CSCR) [photochemical]
Diode (810 nm) TTT = Choroidal melanoma [sub-photothermal]
- Nd:YAG (1064 nm) CW low power → photothermal coagulation of ciliary body (CPC)
- Nd:YAG (1064 nm) Q-switched high peak power → photodisruption (capsulotomy, LPI)
- Diode (810 nm) continuous → photothermal (PRP, CPC)
- Diode (689 nm) → photochemical activation of verteporfin (PDT)
Sign of keratoconus on torch light, slit lamp, retinoscopy, OCT
keratoconus signs torch light slit lamp retinoscopy OCT clinical examination PG exam
https://eyewiki.org/Keratoconus
SIGNS OF KERATOCONUS
Systematic Examination Notes for PG Exams
Definition: Keratoconus is a progressive, non-inflammatory ectasia characterized by central or paracentral corneal thinning and protrusion, producing irregular myopic astigmatism. Prevalence: 0.1-0.2%; onset in teens-twenties; bilateral but asymmetric.
I. SIGNS ON TORCH LIGHT / NAKED EYE EXAMINATION
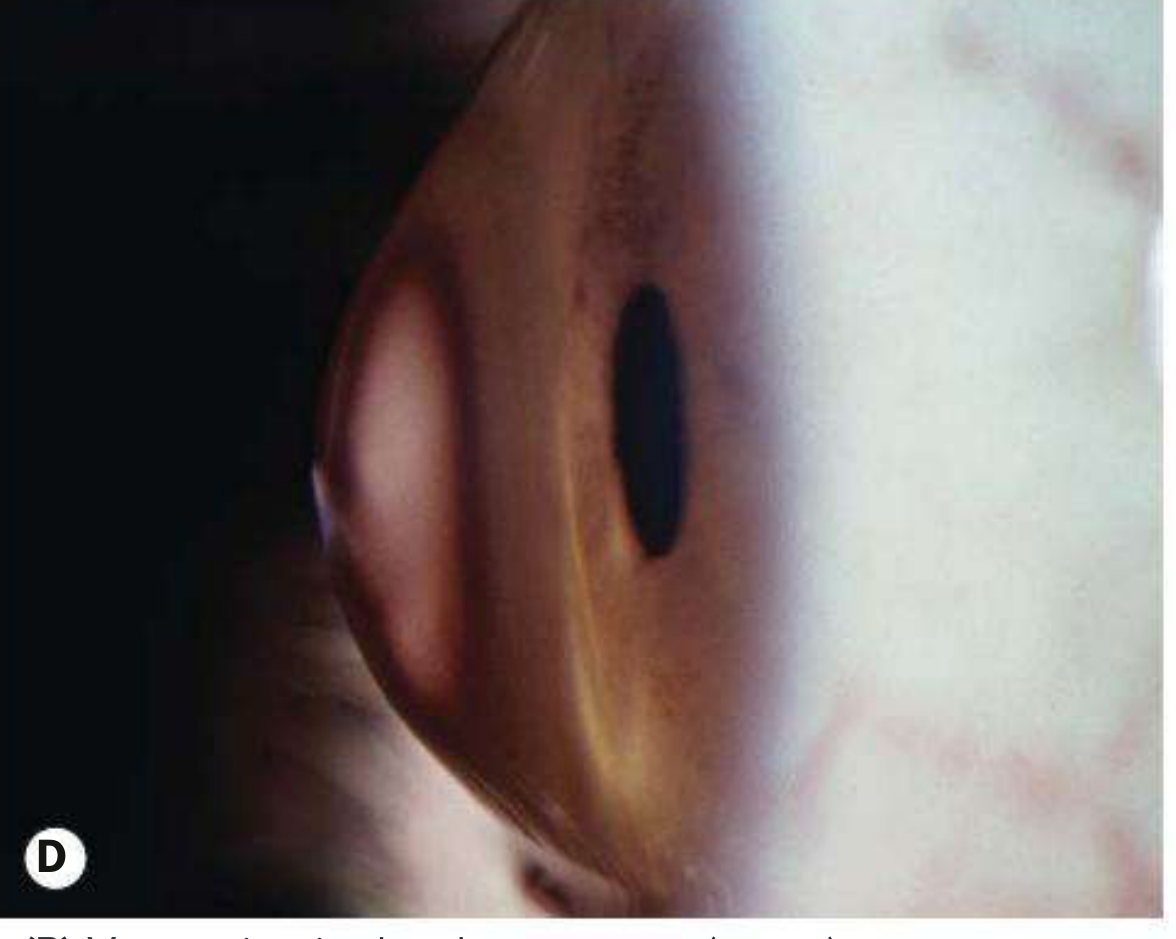
1. Munson's Sign ⭐ (Most Classic Torch/External Sign)
- What it is: V-shaped or angular bulging/indentation of the lower eyelid when the patient looks downward
- Mechanism: The protruding corneal cone pushes against the lower lid, creating a V-shaped deformity of the lower lid margin in downgaze
- Significance: Sign of moderate to advanced keratoconus; indicates significant corneal protrusion
- How to elicit: Ask the patient to look down; observe the lower eyelid margin from the front

2. Rizzuti's Sign
- What it is: A sharply focused beam of light (conical reflection) seen near the nasal limbus when a penlight/torch is shone from the temporal side across the cornea
- Mechanism: The steepened cone acts as a converging lens and focuses the temporal light beam as a sharp triangular or conical reflection on the nasal limbus
- Significance: Present in moderate-advanced keratoconus; relatively specific
- How to elicit: Direct torch light from the temporal side - look at the nasal limbus for the focused cone of light
3. Visible Conical Protrusion of Cornea
- In advanced disease, the forward protrusion of the cone is visible to naked eye on lateral inspection (profile view of eye)
- The cornea appears conical/tent-shaped rather than smoothly spherical
4. Charleux Sign (Placido Disc Reflection)
- Irregular, distorted reflection of Placido disc rings (or any circular light source)
- Oval or pear-shaped distortion of the reflected rings indicates irregular corneal surface
Summary Table - Torch / External Signs
| Sign | Description | Stage |
|---|---|---|
| Munson's sign | V-shaped lower lid deformity on downgaze | Moderate-advanced |
| Rizzuti's sign | Nasal limbal cone reflex on temporal illumination | Moderate-advanced |
| Conical protrusion | Visible cone on lateral inspection | Advanced |
| Charleux sign | Distorted Placido disc reflection | Early-moderate |
II. SIGNS ON RETINOSCOPY
1. Scissors Reflex (Scissoring Reflex) ⭐⭐ THE KEY SIGN
- What it is: The retinoscopy reflex appears as two separate bands moving toward and away from each other, like the blades of a pair of scissors opening and closing
- Mechanism: The irregular, steepened corneal surface in keratoconus creates different zones of refraction - the central cone has very high myopic power while the peripheral cornea has less power. This refractive inhomogeneity splits the retinoscopy light reflex into two bands moving in opposite directions
- Appearance: On "with" movement in one meridian and "against" movement in the perpendicular meridian - but in keratoconus these don't align into clean axis-specific reflexes; they form an irregular scissoring pattern
- Clinical note: Even early keratoconus (before visible slit-lamp signs) can show subtle scissoring
- Stage: Present from early to advanced stages; more dramatic in advanced disease
2. Oil Droplet Reflex (Charleux Sign on Retinoscopy)
- What it is: On direct ophthalmoscopy or distant direct ophthalmoscopy from 0.5 metres, the red reflex shows a well-demarcated, central dark shadow surrounded by the orange-red reflex - resembling an oil droplet in water
- Mechanism: The steep cone creates a zone of very high myopia centrally that reflects the light differently from the surrounding less-myopic peripheral cornea - resulting in a dark central shadow in the red reflex
- Best seen: With a direct ophthalmoscope at ~0.5 m using the +1 or +2 lens

3. Irregular Refraction / Inability to Neutralize
- The reflex cannot be neutralized with a single lens at retinoscopy - different parts of the pupil neutralize at different points
- Progressive myopia with irregular astigmatism that cannot be fully corrected with spectacles
- Repeated change in prescription with poor best spectacle-corrected visual acuity (BSCVA)
Summary Table - Retinoscopy Signs
| Sign | Description | Stage |
|---|---|---|
| Scissors reflex | Two reflex bands moving like scissor blades | Early onwards |
| Oil droplet / Charleux sign | Central dark shadow in red reflex at 0.5 m | Moderate-advanced |
| Irregular reflex | Cannot neutralize uniformly across pupil | Any stage |
| Progressive myopia | Increasing myopic astigmatism on manifest refraction | Early |
III. SIGNS ON SLIT-LAMP BIOMICROSCOPY
A. EPITHELIAL SIGNS
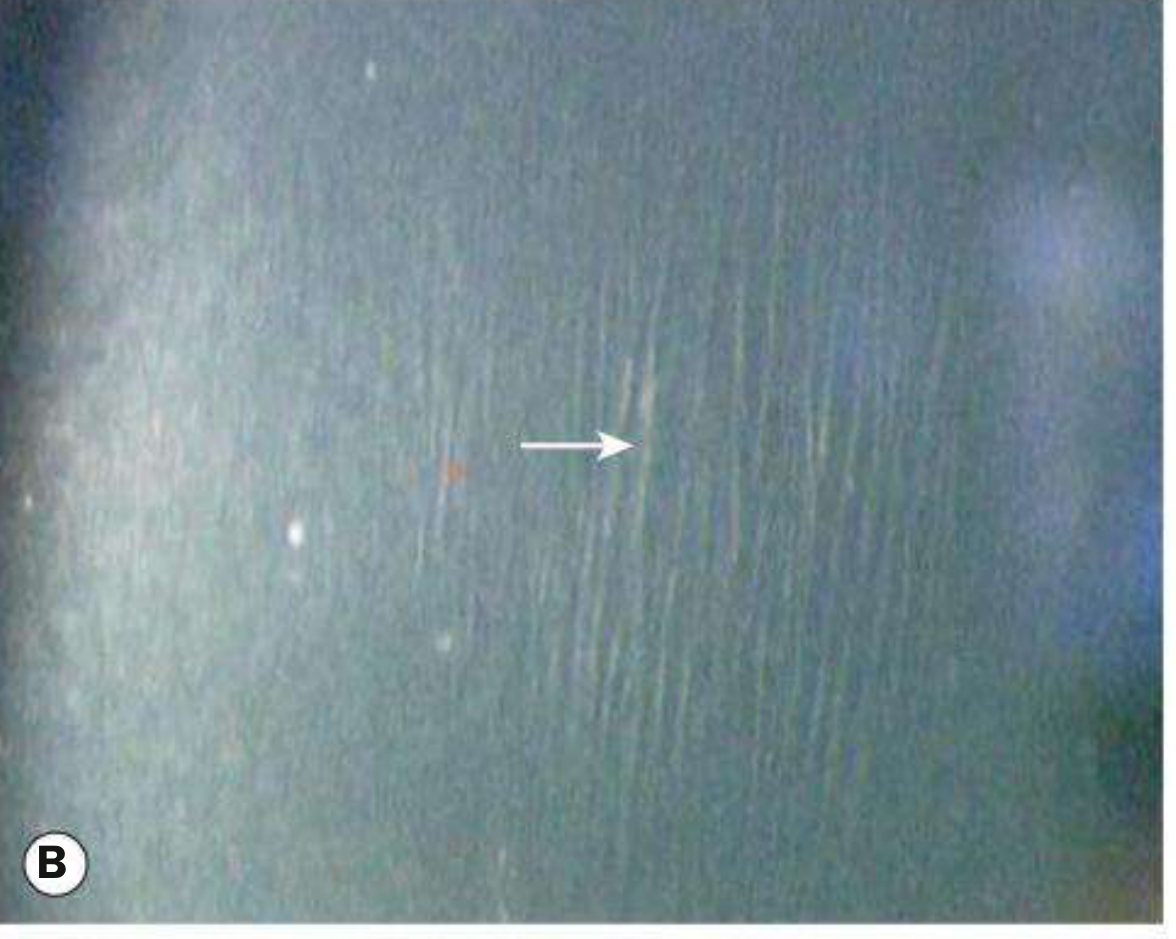
1. Fleischer Ring ⭐⭐
- What it is: A yellowish-brown or grey ring of iron (hemosiderin) deposits in the basal epithelium encircling the base of the cone
- Location: At the cone base (not at the apex); usually incomplete ring
- Best seen with: Cobalt blue filter on slit lamp - appears as a blue/grey ring; can also be seen with broad tangential illumination
- Mechanism: Tear stasis and altered epithelial metabolism at the cone base leads to iron deposition (similar to Hudson-Stahli line mechanism)
- Prevalence: Present in ~50% of keratoconus cases
- Significance: Pathognomonic of keratoconus when present; presence indicates active ectasia
2. Apical Epithelial Thinning
- Epithelium overlying the cone apex is thinned
- In advanced disease: apical scarring (Bowman layer break) - superficial corneal scar at cone apex
- Recurrent corneal erosions possible at apex
B. STROMAL SIGNS
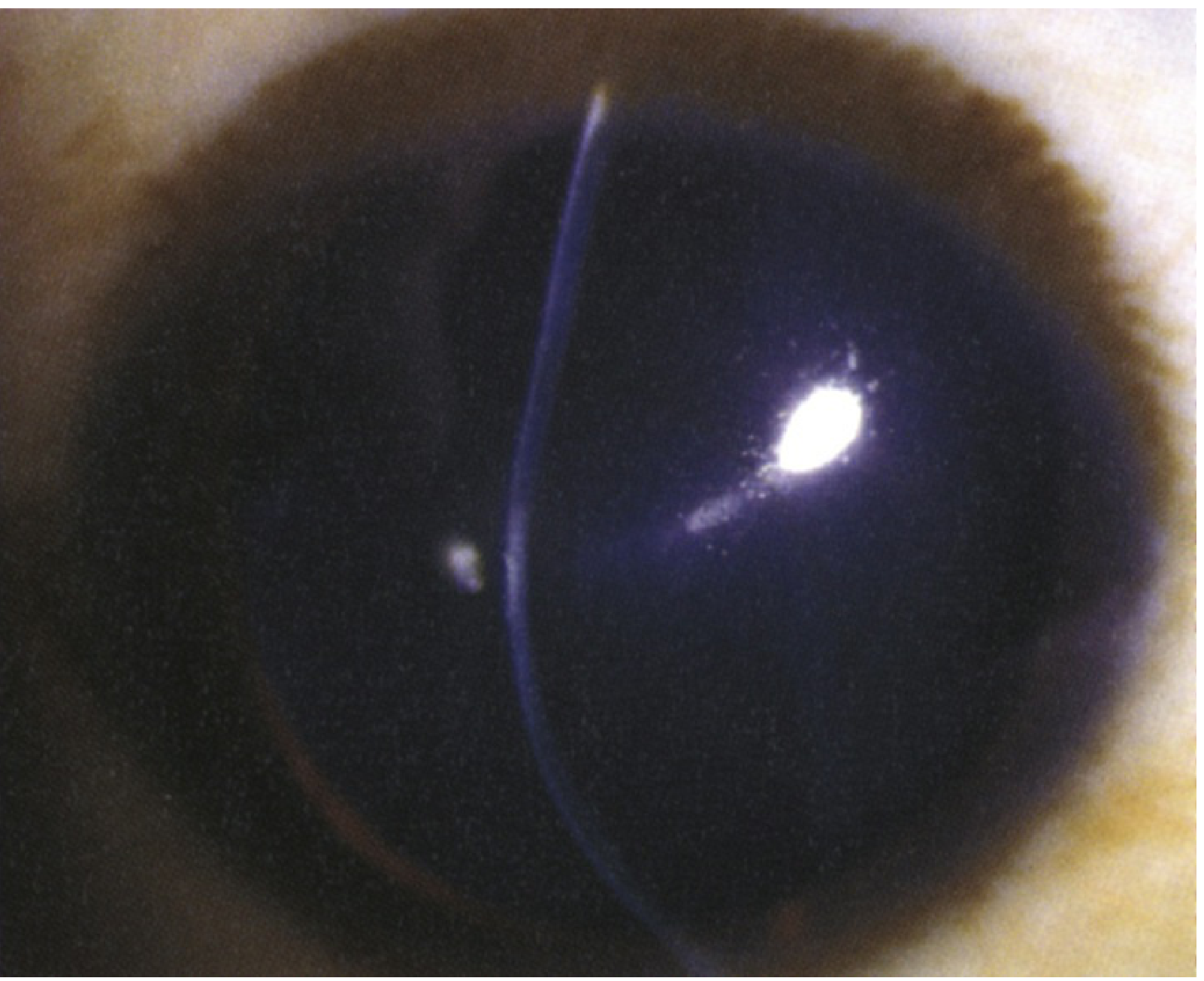
3. Vogt's Striae ⭐⭐
- What it is: Very fine, vertical (or obliquely oriented), bright stress lines in the deep stroma (at the level of the posterior stroma / Descemet membrane junction)
- Appearance: Thin, parallel, white/grey lines running in the same direction as the corneal stretch - usually vertical or slightly oblique
- Characteristic feature: Disappear with gentle pressure on the globe (digital pressure through the eyelid) - this transiently equalizes the corneal tension; this disappearance is pathognomonic of keratoconus
- Best illumination: Retroillumination or specular reflection on slit-lamp
- Mechanism: Represent tension and compression stress lines in the stretched posterior corneal stroma - analogous to Langer's lines in skin
4. Corneal Thinning
- Central or paracentral (usually inferotemporal) thinning of the corneal stroma - maximal at the apex of the cone
- Normal central corneal thickness ~550 µm; in KC reduced to <500 µm (may be 300-400 µm at apex in severe cases)
- The area of maximal thinning on pachymetry is displaced inferiorly from center
- Best quantified by optical pachymetry (slit-lamp) or ultrasound pachymetry
5. Corneal Protrusion / Conical Shape
- On optical section (slit-lamp) the corneal profile shows anterior protrusion of the cone - tenting of the normal curved corneal profile
- The slit-beam shows thinning and forward displacement of the central/inferior cornea
- Best appreciated with broad beam tangential illumination or optical section
6. Subepithelial / Anterior Stromal Scarring
- Bowman layer ruptures and scarring at the apex of the cone in advanced disease
- Appears as white anterior stromal opacification at the cone apex
- Causes permanent visual deterioration not correctable with contact lenses
C. DESCEMET MEMBRANE / ENDOTHELIAL SIGN
7. Acute Corneal Hydrops
- What it is: Sudden, dramatic episode of corneal edema due to rupture of Descemet membrane at the stretched cone apex
- Symptoms: Acute severe pain, photophobia, profuse tearing, sudden dramatic drop in vision
- Slit-lamp appearance:
- Sudden corneal stromal and epithelial edema (whitish, opaque cornea)
- Microcysts and bullae in the epithelium
- The Descemet break may be visible as a scroll/edge
- Absence of keratic precipitates (non-inflammatory)
- Natural history: Break usually heals in 6-10 weeks; residual stromal scar forms - occasionally this flattens the cornea and paradoxically may improve vision
- Management: Cycloplegia, hypertonic saline 5% ointment, bandage contact lens; intracameral gas injection accelerates resolution
Summary Table - Slit-Lamp Signs
| Sign | Layer | Appearance | Special Feature |
|---|---|---|---|
| Fleischer ring | Basal epithelium | Iron deposits at cone base | Best with cobalt blue filter |
| Vogt striae | Deep stroma | Vertical bright stress lines | Disappear with globe pressure |
| Corneal thinning | Stroma | Central/inferocentral thinning | Maximal at apex |
| Conical protrusion | Full thickness | Forward tenting on optical section | Visible on tangential beam |
| Apical scarring | Epithelium/Bowman | Anterior stromal opacity | Advanced disease |
| Acute hydrops | Descemet rupture | Sudden diffuse stromal edema | Emergency presentation |
| Prominent corneal nerves | Stroma | Fine white lines from limbus | Elongated, visible stromal nerves |
IV. SIGNS ON KERATOMETRY
- Irregular mires: The circular mire reflection becomes egg-shaped or distorted instead of round
- Steep keratometry readings: K readings >47 D (normal ~43-44 D); graded as mild <48 D, moderate 48-54 D, severe >54 D
- Inability to align mires: The mire alignment cannot be achieved simultaneously in two meridians due to irregular astigmatism
- Progressive steepening on serial keratometry = confirms progression
V. SIGNS ON CORNEAL TOPOGRAPHY AND TOMOGRAPHY (OCT / PENTACAM)
A. ANTERIOR SURFACE TOPOGRAPHY (Placido-based / Videokeratography)
Characteristic Patterns:
- Inferior steepening - inferotemporal zone of higher curvature (warm colors = orange/red on axial power map)
- Asymmetric bow-tie pattern - in early KC, the normal symmetric bow-tie of "with-the-rule" astigmatism becomes asymmetric, with one arm of the bow-tie (usually inferior) being larger/steeper
- Progression to skewed bow-tie - axis of steepest curvature tilts from vertical
- Isolated inferior cone - in moderate KC, isolated inferotemporal island of high curvature (the cone) separated from the upper hemisphere (asymmetric bow-tie pattern breaks into a "claw")
- I-S asymmetry (Inferior-Superior ratio): Inferior corneal power minus Superior corneal power >1.4 D = suspicious; >1.9 D = diagnostic (Rabinowitz criteria)
- KISA% index: Combines K (central keratometry), I-S value, SRAX (skewed radial axes), and AST (astigmatism); >100% = keratoconus; 60-100% = suspect
B. POSTERIOR SURFACE / TOMOGRAPHY (Scheimpflug - Pentacam, Galilei)
Key Findings:
- Posterior surface elevation - elevation above best-fit sphere (BFS):
- Suspicious: >15 µm at thinnest point on posterior elevation map
- Diagnostic: >16 µm posterior elevation (on 8 mm BFS) at the thinnest point
- Inferocentral posterior elevation island - the posterior surface bulges forward in the inferior-central zone (shown as warm colors on posterior elevation map)
- Anterior surface elevation - generally less sensitive; elevation >12 µm on 8 mm BFS at thinnest point is suspicious
- Asymmetric elevation - superior-inferior asymmetry of posterior surface
C. PACHYMETRY MAP (Corneal Thickness)
- Focal inferior thinning - thinnest point displaced inferiorly from visual axis/center
- Thinnest point <500 µm - normal is ~550 µm centrally
- Thinnest point - apex displacement - distance from corneal apex to thinnest point >0 = diagnostic; in normal cornea these coincide
- Pachymetric progression index - rate of thinning from periphery to center: in KC the progression is steeper than normal
- Percentage Thickness Increase (PTI) - rate of thickness increase from thinnest point to periphery is abnormally steep
- Asymmetry between fellow eyes - >100 µm difference between fellow eyes is suspicious
D. BELIN-AMBROSIO ENHANCED ECTASIA DISPLAY (BAD / BAD-D)
- Pentacam software combining anterior elevation, posterior elevation, pachymetry, pachymetric progression, and best corrected VA
- BAD-D score ≥1.6: Suspicious; ≥2.69: Diagnostic of keratoconus
- Currently the most sensitive screening tool for subclinical/forme fruste keratoconus
E. AS-OCT (Anterior Segment OCT) Specific Findings
Structural / Cross-sectional B-scan:
- Anterior corneal thinning - focal reduction in corneal thickness inferiorly/centrally on meridional cross-section
- Posterior corneal surface protrusion - posterior surface curves more anteriorly at the cone site than expected
- Asymmetric thickness distribution - cross-sectional image shows wedge-shaped thinning
- Bowman layer irregularities - focal breaks, thinning, or absence of Bowman layer at apex in advanced cases (high-resolution OCT)
- Epithelial thickness mapping (epithelial OCT):
- In normal cornea: epithelium is thicker inferiorly
- In keratoconus: epithelium undergoes compensatory remodeling - becomes thinner over the cone apex (to maintain optical surface) and thicker in the ring around the cone (doughnut pattern)
- "Doughnut sign" on epithelial thickness map: Thicker annulus surrounding a thin central/paracentral zone - a highly sensitive early marker
- This epithelial remodeling precedes topographic changes in some cases
Quantitative OCT Parameters:
| Parameter | Normal | Keratoconus |
|---|---|---|
| Minimum corneal thickness (thinnest point) | ≥500 µm | <500 µm; often 300-400 in severe |
| Location of thinnest point | At/near center | Displaced inferiorly |
| Posterior elevation at thinnest | <15 µm | >16 µm |
| Anterior elevation at thinnest | <12 µm | >12 µm |
| Epithelium over cone | Normal | Thinned (doughnut sign) |
| Epithelium around cone | Normal | Thickened |
VI. ADDITIONAL INVESTIGATIONS (PG Awareness)
| Investigation | Keratoconus Finding |
|---|---|
| Placido disc | Distorted, irregular oval rings |
| Keratometry | Steep, irregular, non-alignable mires; K >47 D |
| Ultrasound pachymetry | Focal thinning; thinnest point displaced inferiorly |
| Specular microscopy | Elongated, polymegethous endothelial cells |
| Confocal microscopy | Elongated/bright corneal nerves; Bowman breaks; spindle-shaped keratocytes |
VII. HIGH-YIELD EXAM SUMMARY
TORCH LIGHT
├── Munson's sign → V-shaped lower lid on downgaze (moderate-advanced)
├── Rizzuti's sign → Nasal limbal cone on temporal torch illumination
└── Visible cone → Forward protrusion visible on lateral inspection
RETINOSCOPY
├── Scissors reflex → 2 bands moving like scissor blades (KEY SIGN, early-advanced)
├── Oil droplet reflex → Central dark shadow in red reflex on direct ophthalmoscopy
└── Irregular reflex → Cannot neutralize uniformly; poor BSCVA
SLIT LAMP
├── Fleischer ring → Iron deposits at cone base; cobalt blue filter; base NOT apex
├── Vogt striae → Deep stromal stress lines; DISAPPEAR on globe pressure
├── Corneal thinning → Inferocentral; maximal at apex
├── Conical protrusion → Visible on optical section
├── Apical scarring → Bowman break; advanced
└── Acute hydrops → Descemet rupture; sudden edema; 6-10 weeks to resolve
OCT / TOPOGRAPHY / PENTACAM
├── Inferior steepening → Inferotemporal cone on axial map
├── Posterior elevation → >16 µm above BFS at thinnest point (EARLIEST change)
├── Pachymetry → Thinnest point <500 µm, displaced inferiorly
├── Doughnut sign (OCT) → Thin epithelium over cone, thick ring around it
├── Asymmetric bow-tie → On anterior topography
└── BAD-D score ≥2.69 → Most sensitive screening tool
- Vogt striae disappear on globe pressure - pathognomonic of keratoconus
- Fleischer ring = iron deposits at base (not apex) of cone; seen with cobalt blue filter
- Munson sign = V-shaped lower lid deformity in downgaze
- Rizzuti sign = nasal limbal reflex on temporal torch illumination
- Oil droplet reflex = dark central shadow in red reflex on distant direct ophthalmoscopy
- Scissors reflex = irregular astigmatism on retinoscopy; sensitivity 97.7%
- Posterior elevation map is more sensitive than anterior for early KC
- Epithelial thinning over cone + thickening around = doughnut sign on AS-OCT epithelial mapping
- Acute hydrops = Descemet membrane rupture; heals in 6-10 weeks; intracameral gas accelerates healing

The pigmented spot has history of 12- 15 month back, first erupt on scalp the slowly gradually progressed to Back, shoulder and chest and abdominal area. Patient has no any sign symptoms, body build is normal with familial hypercholesterolemic the age of patient is 60 years.
eruptive seborrheic keratosis Leser-Trelat sign familial hypercholesterolemia differential diagnosis pigmented spots scalp
Clinical Analysis
- 60-year-old male
- Lesions started 12-15 months ago on scalp, then progressively spread to back, shoulders, chest, abdomen
- No symptoms (asymptomatic)
- Familial hypercholesterolemia
- Normal body build
PRIMARY DIAGNOSIS
Seborrheic Keratoses (SK) - Eruptive Type
CLINICAL REASONING
What the image shows:
Key features supporting SK:
| Feature | This Patient |
|---|---|
| Age | 60 years - typical age of SK (4th-6th decade) |
| Morphology | Multiple dark pigmented papules, "stuck-on" |
| Distribution | Scalp, face, trunk - classic SK distribution |
| Asymptomatic | SK usually asymptomatic (or mildly pruritic) |
| Progression | Gradual spread over months - consistent |
| No ulceration/bleeding | Benign behavior |
THE CRITICAL ALERT: SIGN OF LESER-TRÉLAT
Sign of Leser-Trélat = Sudden/rapid eruption of multiple seborrheic keratoses in an adult as a cutaneous paraneoplastic marker of internal malignancy
Criteria (Andrews' Diseases of the Skin):
- Keratoses begin at approximately the same time as development of cancer
- Rapid onset of multiple lesions
- Run a parallel course in regard to growth and remission
- Often pruritic (can be asymptomatic too)
- May be accompanied by acanthosis nigricans or tripe palms
This patient meets:
- Rapid eruption: started ~12-15 months ago and spread widely
- Multiple lesions: scalp → trunk (widespread distribution)
- Age: 60 (age when both SK and malignancy are more common)
- Asymptomatic: not against the diagnosis
Associated malignancies (Fitzpatrick's Dermatology):
- 60% are adenocarcinomas, primarily GI tract (colon most common)
- Lymphoma / lymphoproliferative disease
- Breast carcinoma
- Lung SCC
- Gastric, renal, hepatic, pancreatic carcinoma
ROLE OF FAMILIAL HYPERCHOLESTEROLEMIA (FH)
-
Xanthomas in FH typically present as yellowish papules/nodules over tendons (tendon xanthomas - Achilles, extensor tendons of hands), xanthelasma palpebrarum, and corneal arcus - morphologically distinct from what is seen here (these are dark pigmented papules, not yellow lipid deposits)
-
The lesions in the image are clearly NOT xanthomas - xanthomas are yellowish, soft, and have a characteristic lipid deposit histology
-
FH does not cause seborrheic keratoses - it is likely a coincidental comorbidity here
-
However, importantly: statin use (very likely in FH patient) has been associated with eruptive seborrheic keratoses in some reports
DIFFERENTIAL DIAGNOSIS
| Condition | Features | Why Less Likely Here |
|---|---|---|
| Seborrheic keratoses ✅ | Multiple dark stuck-on papules, scalp/trunk, asymptomatic | PRIMARY DIAGNOSIS |
| Dermatosis papulosa nigra | Small dark papules, typically darker-skinned individuals, periorbital/malar | Possible variant - face distribution overlaps, but this patient has widespread truncal lesions |
| Actinic lentigines (solar spots) | Flat brown macules, sun-exposed areas | Usually flat, sun-damaged skin; these appear more elevated |
| Flat melanocytic nevi | Pigmented nevi | Fewer in number, earlier onset |
| Acanthosis nigricans | Velvety, hyperpigmented, intertriginous | Different morphology (velvety, not discrete papules) |
| Melanoma (in situ / lentigo maligna) | Irregular pigmentation, scalp, sun-exposed | Must exclude - biopsy atypical lesions |
| Xanthoma | Yellowish papules/plaques - in FH | Yellow color, different sites (tendons/eyelids), not pigmented |
| Eruptive xanthomas | Yellow-orange papules on extensor surfaces | Only in severe hypertriglyceridemia; yellow color |
INVESTIGATION PLAN
Skin Investigations:
- Dermoscopy - of representative lesions: SK shows comedo-like openings, milia-like cysts, fissures and ridges ("cerebriform" pattern); no atypical vascular patterns
- Skin biopsy - of the most atypical or rapidly changing lesion - histology: acanthosis, papillomatosis, pseudo-horn cysts, hyperkeratosis, no cytologic atypia
Systemic Workup (to rule out Leser-Trélat / occult malignancy):
| Investigation | Rationale |
|---|---|
| Colonoscopy | Most common associated malignancy - adenocarcinoma colon |
| CECT abdomen and pelvis | Screen for GI, renal, hepatic, pancreatic malignancy |
| CECT chest | Lung SCC, lymphoma |
| Upper GI endoscopy | Gastric adenocarcinoma |
| Fecal occult blood test | Colorectal cancer screening |
| CBC + peripheral smear | Lymphoproliferative disease |
| LFT, RFT | Baseline, hepatic malignancy |
| CEA, CA 19-9, CA 125 | Tumor markers as appropriate |
| PSA | Prostate carcinoma (60-year-old male) |
| Lipid profile | Monitor FH (likely already on statins) |
MANAGEMENT
Skin Lesions:
- No treatment required if SK is confirmed and patient is asymptomatic
- If symptomatic/cosmetically bothersome:
- Cryotherapy with liquid nitrogen (first-line, no scarring)
- Curettage (with or without liquid nitrogen)
- Electrodesiccation (fulguration)
- Shave removal
- Topical hydrogen peroxide 40% (Eskata) - approved for SK
- Treating the underlying malignancy (if found) resolves ~50% of SK lesions
Monitoring:
- Periodic skin examination for atypical/changing lesions
- Biopsy any lesion with ABCDE changes
- Annual systemic cancer surveillance
SUMMARY BOX
60M | Eruptive pigmented papules | Scalp → Trunk | 12-15 months | Asymptomatic
PRIMARY DX: Seborrheic Keratoses (Eruptive Pattern)
ALARM: Consider Sign of Leser-Trélat → Rule out internal malignancy
MOST COMMON MALIGNANCY: GI adenocarcinoma (colon)
FH RELEVANCE: Not causative; xanthomas morphologically distinct
NEXT STEP: Dermoscopy + Skin biopsy (atypical lesion) + Colonoscopy + CECT thorax-abdomen-pelvis
⚠️ Clinical Alert: The rapid eruptive onset (12-15 months) with spread from scalp to widespread truncal distribution in a 60-year-old is the key red flag. Even though seborrheic keratoses are common in this age group, the sudden eruption of multiple new lesions - especially spreading cranio-caudally - warrants systemic malignancy workup before reassuring the patient this is benign. The familial hypercholesterolemia history is contextual but does not explain this eruption.
Write a notes on imaging modalities available for Optic disc evaluation to write in PG EXAM