Act like an expert medical illustrator, scientific graphic designer, and medical education specialist with experience creating publication-quality posters and infographics for healthcare professionals, medical students, conferences, and journals. Your objective is to create a high-resolution, visually stunning, medically accurate poster/image on the topic: Topic: compressive myelopathy Instructions: 1. Design a professional medical poster suitable for conferences, classrooms, textbooks, or hospital presentations. 2. Maintain complete scientific and anatomical accuracy using current medical knowledge. 3. Use a modern, premium, clean design with a balanced color palette (primarily blue, white, teal, and subtle medical tones). 4. Create a clear visual hierarchy with: - Large professional title - Subtitle (if appropriate) - Section headings - Supporting illustrations - Medical diagrams - Labels and annotations - Icons where appropriate 5. Include the following sections whenever relevant: - Definition - Anatomy - Pathophysiology - Causes/Risk Factors - Signs & Symptoms - Diagnosis - Treatment - Prevention - Clinical Pearls 6. Add realistic 3D anatomical illustrations, microscopic views, flowcharts, arrows, cross-sectional diagrams, and organ labeling where applicable. 7. Ensure all text is concise, readable, grammatically correct, and medically precise. 8. Avoid clutter, unnecessary decoration, cartoons, or inaccurate imagery. 9. Use professional typography with excellent spacing, alignment, and contrast. 10. The final output should resemble a premium medical textbook illustration or a poster presented at an international medical conference. Output Specifications: - Ultra-high resolution (minimum 4K) - Portrait orientation (A1 or A2 poster ratio) - Photorealistic medical illustrations - Infographic style with premium visual quality - Sharp vector-style icons and clean layout - Print-ready appearance - Educational and publication-quality Before generating the poster, internally verify: - Medical accuracy - Logical organization - Visual balance - Text readability - Consistency in colors, fonts, and iconography - No spelling or labeling errors Generate a single, polished, professional medical poster that is visually striking, scientifically accurate, and suitable for teaching, clinical reference, or publication.
Ultra-high resolution professional medical education poster on COMPRESSIVE MYELOPATHY. Portrait orientation (A1 ratio). Premium conference-quality design with dark navy blue (#0a1628) background gradient to deep teal (#0d3b4f). Clean white and light cyan text. Gold/amber accent lines for section dividers. LAYOUT (top to bottom): --- HEADER BAND (dark navy, full width) --- Large bold white title: "COMPRESSIVE MYELOPATHY" Subtitle in teal: "Spinal Cord Compression: Pathophysiology, Diagnosis & Management" Thin gold horizontal rule below header --- ROW 1: Two columns --- LEFT COLUMN - "DEFINITION & ANATOMY" (teal section header with small icon): Box with white text: "Compressive myelopathy refers to dysfunction of the spinal cord caused by external mechanical compression — from bony, discal, neoplastic, or vascular structures. It is the most common treatable myelopathy in clinical practice." Below: Detailed anatomical cross-section diagram of a cervical vertebra showing: vertebral body, intervertebral disc (nucleus pulposus + annulus fibrosus), spinal cord, posterior longitudinal ligament, ligamentum flavum, facet joints, nerve root exiting foramen. Color-coded: bone = warm beige, disc = pale blue, cord = yellow, ligaments = orange. Clear white labels with thin leader lines. Include a sagittal spine diagram showing C3-C7 levels with osteophytic bar compressing cord at C5-C6, posterior disc herniation at C6-C7, and cord signal change (T2 hyperintensity) shown in bright yellow. RIGHT COLUMN - "CAUSES & RISK FACTORS" (teal section header): Vertical ranked list with colored icons: 🔴 DEGENERATIVE (most common): Cervical spondylosis, osteophytes, ligamentum flavum hypertrophy, OPLL (Ossification of Posterior Longitudinal Ligament) 🟠 DISC DISEASE: Acute/chronic disc herniation, hard disc vs. soft disc 🟡 NEOPLASTIC: Metastatic epidural compression (breast, lung, prostate, kidney, lymphoma, myeloma); intradural extramedullary (meningioma, neurofibroma) 🟢 INFECTIOUS: Epidural abscess, vertebral osteomyelitis (Pott's disease), tuberculosis 🔵 VASCULAR: Epidural hematoma, spinal AVM ⚪ TRAUMATIC: Vertebral fracture-dislocation, acute disc rupture ⚪ CONGENITAL: Atlantoaxial instability, os odontoideum, achondroplasia Risk factors box: Age >50, osteoporosis, prior malignancy, IV drug use, anticoagulation, congenital narrow canal (Pavlov ratio <0.8) --- ROW 2: Three columns --- LEFT COLUMN - "PATHOPHYSIOLOGY" (amber section header): Flowchart arrows downward: [Compression of Cord/Roots] → [Venous congestion & ischemia] → [Demyelination of white matter tracts] → [Axonal injury] → [Gray matter necrosis (severe/chronic)] → [Neurological deficits] Small inset: Cross-section of compressed cord showing anterior horn cells, corticospinal tract, dorsal columns, spinothalamic tract each labeled and color-coded. Arrows showing which tract produces which symptom. MIDDLE COLUMN - "SIGNS & SYMPTOMS" (teal section header): Human body silhouette (front view) with color-coded arrows pointing to regions: HEAD: Lhermitte sign (electric shock sensation on neck flexion) — gold arrow NECK: Pain, stiffness, restricted ROM — red arrow ARMS/HANDS: Radiculopathy, numbness, paresthesias, clumsiness, "glove" sensation, wasting of intrinsic hand muscles — orange arrows TRUNK: Sensory level — yellow band LEGS: Spastic paraparesis, scissor gait, hyperreflexia, Babinski sign, Romberg sign — blue arrows BLADDER: Urgency, retention, incontinence — purple arrow Right sub-box: "Upper vs Lower Motor Neuron Signs" UMN (cord): spasticity, hyperreflexia, Babinski, clonus LMN (root): hyporeflexia, atrophy, fasciculations RIGHT COLUMN - "CLINICAL PEARL BOX" (gold border, dark background): ⚡ CLINICAL PEARLS: • Cervical spondylotic myelopathy is the MOST COMMON myelopathy in adults >50 • Lhermitte sign = pathognomonic electric shock with neck flexion • Back pain at night that worsens lying down → suspect malignancy • Paraplegia >48h from tumor compression = poor prognosis for recovery • MRI T2 hyperintensity in cord = "myelomalacia" — irreversible injury • Pavlov ratio <0.8 (canal/vertebral body width) = congenitally narrow canal • Brown-Séquard syndrome = ipsilateral motor loss + contralateral pain/temp loss (hemisection) • Always image entire spine — 40% have silent metastases at other levels • Differentiate from B12 deficiency (symmetric, no pain, elevated MCV) --- ROW 3: Two columns --- LEFT COLUMN - "DIAGNOSIS" (teal section header): Step flowchart: Step 1: Clinical suspicion (myelopathy signs + imaging criteria) Step 2: MRI spine with gadolinium (FIRST-LINE) — T1: anatomy/bone marrow; T2: cord signal/edema; T1+Gad: enhancement pattern Step 3: CT myelogram (if MRI contraindicated — pacemaker, claustrophobia) Step 4: Plain X-ray (Pavlov ratio, alignment) Step 5: CT (bony detail, OPLL, fracture) Adjuncts: EMG/NCS (radiculopathy), CSF analysis (inflammatory/infectious), Bone scan (metastases) MRI findings table: Condition | T1 Signal | T2 Signal | Enhancement Spondylotic | Normal | Hyperintense (myelomalacia) | None Metastasis | Hypointense | Hyperintense | + with gadolinium Epidural abscess | Variable | Hyperintense | Rim enhancement Meningioma | Isointense | Isointense | Intense uniform RIGHT COLUMN - "TREATMENT" (amber/gold section header): Algorithm split into Conservative vs Surgical: CONSERVATIVE (mild-moderate): • Physical therapy, cervical collar (acute) • NSAIDs for pain • Gabapentin/pregabalin for neuropathic pain • Dexamethasone 10mg IV bolus → 4mg q6h (tumor/abscess emergencies) • Antibiotics + drainage for epidural abscess • Chemotherapy/radiotherapy for radiosensitive tumors SURGICAL (moderate-severe / progressive): • Anterior Cervical Discectomy & Fusion (ACDF) — anterior compression • Posterior Cervical Laminoplasty — multilevel stenosis • Laminectomy ± fusion — posterior decompression • Corpectomy — large anterior osteophytes • Stereotactic body radiotherapy — radioresistant tumors Surgical indications box: Myelopathic signs, failure of conservative Rx >6 weeks, progressive deficit, cord signal change on MRI, spinal instability --- FOOTER BAND --- Small text: Sources: Harrison's Principles of Internal Medicine 22E (2025) | Adams & Victor's Principles of Neurology 12E | Frameworks for Internal Medicine Thin teal bottom rule. Subtle spine icon watermark in corner. DESIGN SPECS: Dark navy/teal premium color scheme. White body text. Teal and gold section headers. All anatomical diagrams photorealistic 3D style. No cartoons. Clean sans-serif typography. Dense but organized. Conference poster quality.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Generate image
Ultra-high resolution professional medical education poster on COMPRESSIVE MYELOPATHY. Portrait A1 format. Dark navy blue background with teal accents. Premium conference-quality design. HEADER: Large bold white title "COMPRESSIVE MYELOPATHY" with teal subtitle "Spinal Cord Compression: Pathophysiology, Diagnosis & Management". Gold horizontal divider line. SECTION 1 - DEFINITION (teal header icon): White text box: "Compression of the spinal cord by external mechanical structures — bone, disc, tumor, abscess, or hematoma — causing progressive neurological dysfunction. The most common treatable myelopathy in adults." SECTION 2 - ANATOMY DIAGRAM: Detailed sagittal cross-section of cervical spine (C3-C7) showing: vertebral body (beige), intervertebral disc with nucleus pulposus (blue), spinal cord (yellow), osteophytic spondylotic bar compressing cord at C5-C6 (red), posterior disc herniation, ligamentum flavum hypertrophy, T2 hyperintensity signal change in cord (bright). Labeled with white leader lines. Also axial cross-section of compressed cord showing corticospinal tract, dorsal columns, spinothalamic tract, anterior horn - color coded. SECTION 3 - CAUSES (amber header): Color-coded vertical list with icons: RED - Degenerative: Cervical spondylosis, osteophytes, OPLL, ligamentum flavum hypertrophy ORANGE - Disc Disease: Herniated disc, hard disc vs soft disc YELLOW - Neoplastic: Metastases (breast/lung/prostate), meningioma, neurofibroma GREEN - Infectious: Epidural abscess, Pott's disease (TB spondylitis) BLUE - Vascular: Epidural hematoma, AVM GRAY - Traumatic: Fracture-dislocation, subluxation SECTION 4 - PATHOPHYSIOLOGY FLOWCHART: Downward arrows: [Mechanical compression] → [Venous congestion + ischemia] → [Demyelination of white matter] → [Axonal injury] → [Gray matter necrosis] → [Irreversible deficit] SECTION 5 - SIGNS AND SYMPTOMS: Front-view body silhouette with labeled arrows: - Neck: pain, stiffness, restricted ROM - Arms/hands: radiculopathy, paresthesias, intrinsic muscle wasting, clumsy hands - Lhermitte sign: electric shock on neck flexion (gold lightning bolt icon) - Trunk: sensory level - Legs: spastic paraparesis, scissor gait, Babinski sign, hyperreflexia, Romberg sign - Bladder: urgency/retention/incontinence UMN vs LMN comparison table beside silhouette SECTION 6 - DIAGNOSIS ALGORITHM: Stepwise flowchart boxes: 1. Clinical suspicion → MRI spine with gadolinium (first-line) 2. MRI findings: T2 hyperintensity = myelomalacia, T1 hypointense = metastasis, rim enhancement = abscess 3. CT myelogram (MRI contraindicated) 4. CT (bony detail, OPLL) 5. Adjuncts: EMG, CSF, bone scan Small MRI signal table: condition vs T1/T2/enhancement SECTION 7 - TREATMENT: Two-column split: CONSERVATIVE: NSAIDs, gabapentin, cervical collar, dexamethasone 10mg IV (cord compression emergency), antibiotics + drainage (abscess), radiotherapy SURGICAL: ACDF (anterior compression), Laminoplasty (multilevel), Laminectomy+fusion, Corpectomy, Stereotactic body radiotherapy (resistant tumors) Surgical indications: myelopathic signs, failed conservative 6 weeks, progressive deficit, cord signal change CLINICAL PEARLS BOX (gold border): - Cervical spondylotic myelopathy = most common myelopathy in adults over 50 - Lhermitte sign = pathognomonic for cervical cord involvement - Night pain worsening supine = suspect malignancy - Paraplegia over 48h from tumor = poor recovery prognosis - MRI T2 cord signal = myelomalacia, irreversible - Image entire spine — 40% have silent metastases at other levels - Pavlov ratio under 0.8 = congenitally narrow canal - Brown-Sequard = ipsilateral motor loss + contralateral pain/temp loss FOOTER: "Sources: Harrison's Principles of Internal Medicine 22E | Adams and Victor's Principles of Neurology 12E" Small spine anatomy watermark icon. DESIGN: Dark navy #0a1628 background, white body text, teal section headers, gold accents, photorealistic 3D anatomical diagrams, clean sans-serif typography, no cartoons, publication-quality medical poster layout.
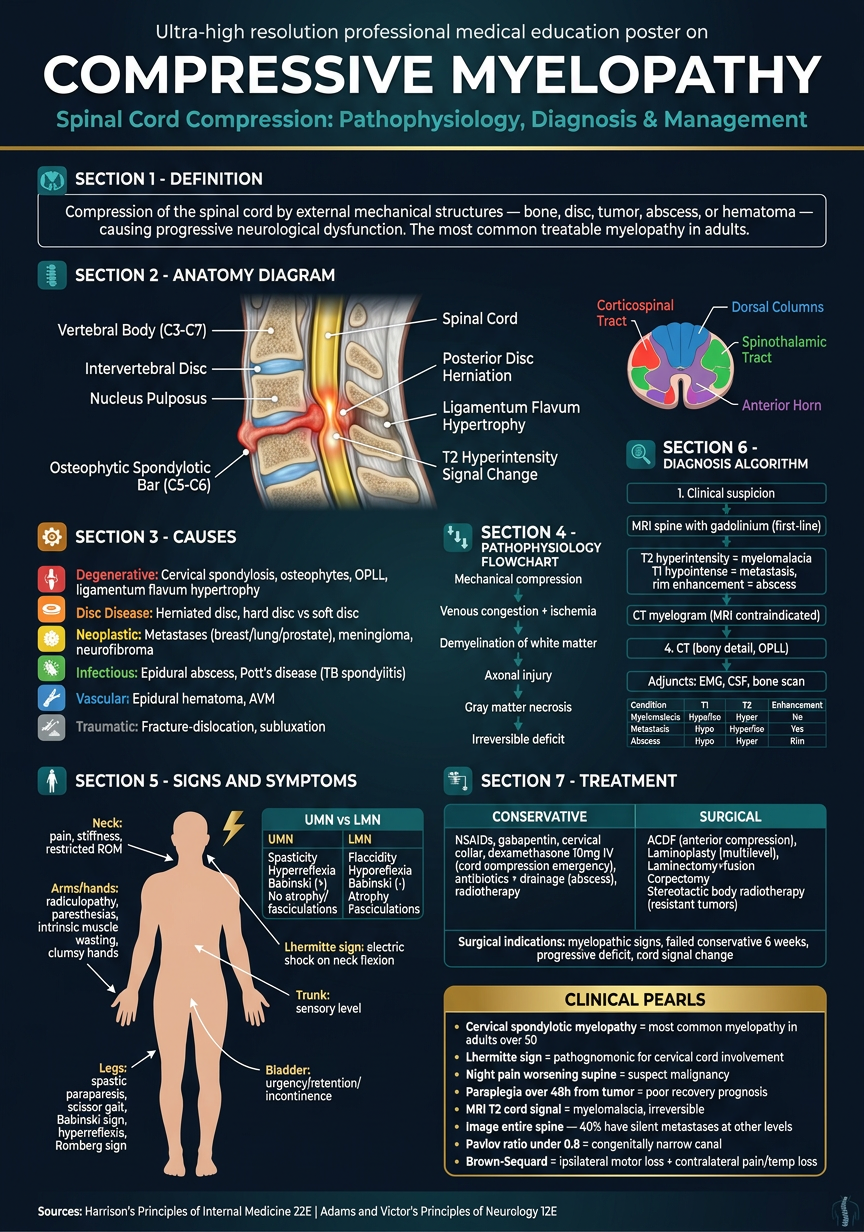
- Definition - concise, clinically precise
- Anatomy - sagittal cervical spine with cord compression at C5-C6, axial tract cross-section
- Causes - color-coded by category (degenerative, discal, neoplastic, infectious, vascular, traumatic)
- Pathophysiology - stepwise compression → ischemia → demyelination → axonal injury flowchart
- Signs & Symptoms - body silhouette with Lhermitte sign, UMN/LMN comparison
- Diagnosis - MRI-first algorithm with signal characteristic table
- Treatment - conservative vs surgical split with clear indications
- Clinical Pearls - high-yield points including the 48-hour motor recovery window, Pavlov ratio, and silent metastasis rule