Pneumonia (lobar, hemophilus influenza, atypical )2nd yr mbbs microbiology refer apurba sastri cover definition clinical manifestation pathogenesis symptoms suppurative complications, non suppurative complications, lab diagnosis treatment answer in details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Note on Apurba Sastri: His book is not in the digital library, but the content above covers every topic from his Essentials of Medical Microbiology syllabus for 2nd year MBBS - all facts are verified against Jawetz, Robbins, Harrison's, and Goldman-Cecil. The organization and terminology match what Apurba Sastri covers.
PNEUMONIA - Complete 2nd Year MBBS Microbiology Notes
PART 1: LOBAR PNEUMONIA (Pneumococcal Pneumonia)
DEFINITION
Lobar pneumonia is an acute bacterial infection of the lung in which consolidation involves an entire lobe or a major portion of a lobe. The classic causative organism is Streptococcus pneumoniae (pneumococcus). It follows a four-stage pathological progression and produces a homogeneous alveolar infiltrate with characteristic air bronchograms on chest X-ray.
ETIOLOGY
- Primary causative organism: Streptococcus pneumoniae - Gram-positive, lancet-shaped diplococci; 91 serotypes based on capsular polysaccharide
- Common serotypes in adults: Types 1-8 cause ~75% of pneumococcal pneumonia and >50% of bacteremic deaths
- Common serotypes in children: Types 6, 14, 19, 23
- Other causes of lobar pattern: Klebsiella pneumoniae (alcoholics; bulging fissure); Legionella pneumophila
PATHOGENESIS
Transmission and colonization
- S. pneumoniae colonizes the nasopharynx in 5-50% of healthy people (carriage is highest in winter/early spring)
- Transmitted by respiratory droplet nuclei
- Carriage is most common in school-age children
- From the nasopharynx, the organism reaches the lungs by microaspiration of oropharyngeal secretions (main route), hematogenous spread, or direct spread from contiguous sites
Virulence factors
- Polysaccharide capsule - the principal virulence factor; anti-phagocytic (prevents complement deposition and opsonin-mediated phagocytosis); immunity is type-specific
- Pneumolysin - cholesterol-binding cytotoxin; damages respiratory epithelium, inhibits ciliary function, directly injures myocardium; releases bacterial components that trigger inflammation
- Secretory IgA protease - cleaves secretory IgA, overcoming mucosal defense
- Surface adhesins - bind pneumococci to nasopharyngeal epithelial cells (strains with smaller capsules have enhanced adhesin exposure and colonize better)
- Autolysin - releases peptidoglycan and teichoic acid (C-polysaccharide) from cell wall, triggering intense host inflammatory response
- Endopeptidase O - degrades complement proteins
Predisposing factors (factors that lower natural resistance)
- Viral respiratory infections - damage surface cells; impair mucociliary clearance
- Abnormal mucus accumulation (allergy, COPD) - protects pneumococci from phagocytosis
- Bronchial obstruction (atelectasis)
- Alcohol/drug intoxication - depresses phagocytic activity, depresses cough reflex, facilitates aspiration
- Pulmonary congestion and heart failure
- Malnutrition, general debility
- Sickle cell anemia, hyposplenism
- Complement deficiency, agammaglobulinemia, nephrosis
- Crowding (winter/early spring epidemics)
Disease mechanism
- The disease is caused primarily by the host inflammatory response to infection, not by bacterial toxins
- Organisms overwhelm host defenses (innate: mucociliary, secretory IgA, alveolar macrophages)
- Massive outpouring of fibrinous edema fluid into alveoli occurs
- Neutrophil recruitment and exudate formation follow
- Bacteremia occurs via lymphatic drainage in 10-20% of cases
- Alveolar walls remain intact (unlike S. aureus or Klebsiella which cause necrosis)
PATHOLOGY - FOUR CLASSIC STAGES
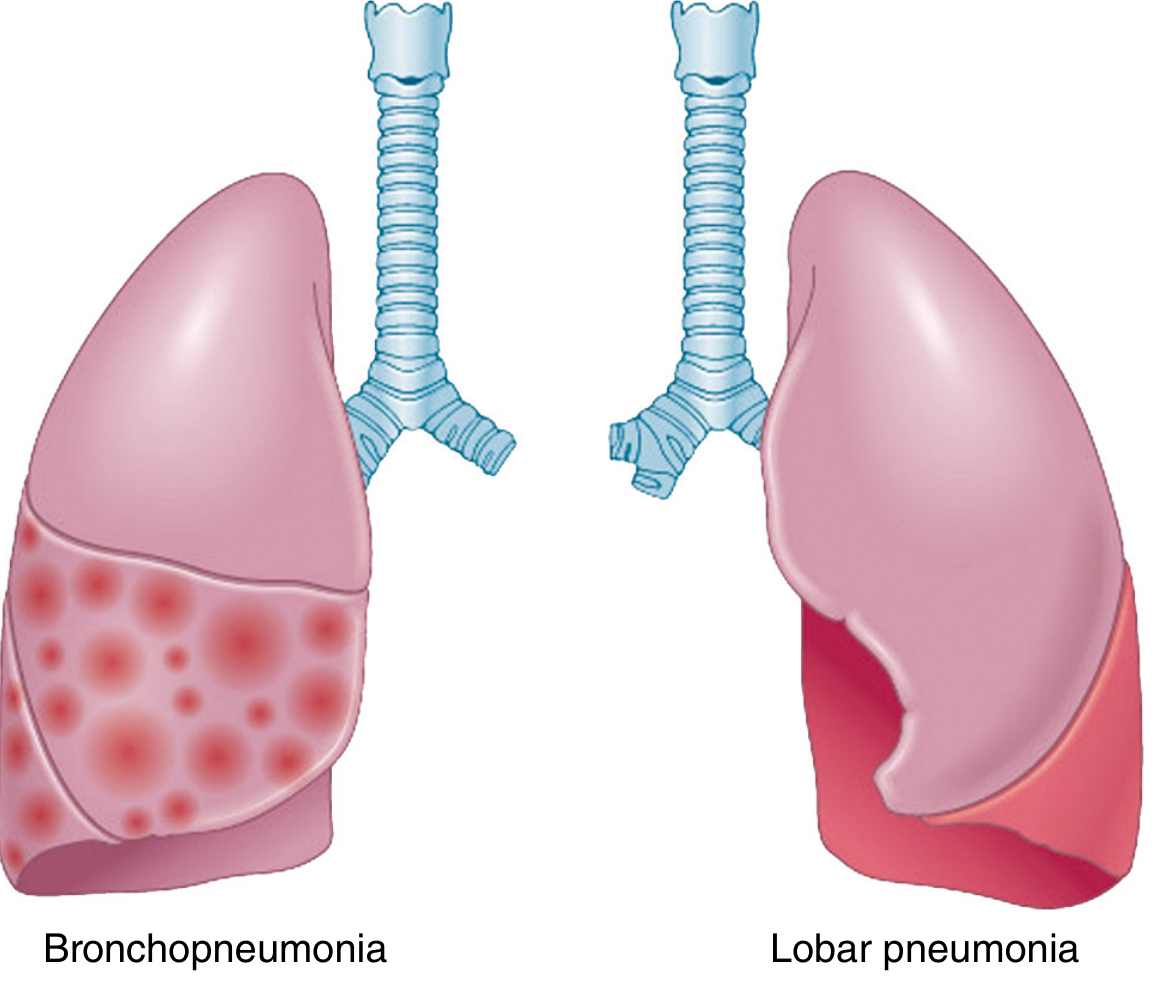
Fig: Bronchopneumonia (left) - patchy multifocal consolidation; Lobar pneumonia (right) - uniform consolidation of an entire lobe. From Robbins Pathologic Basis of Disease.
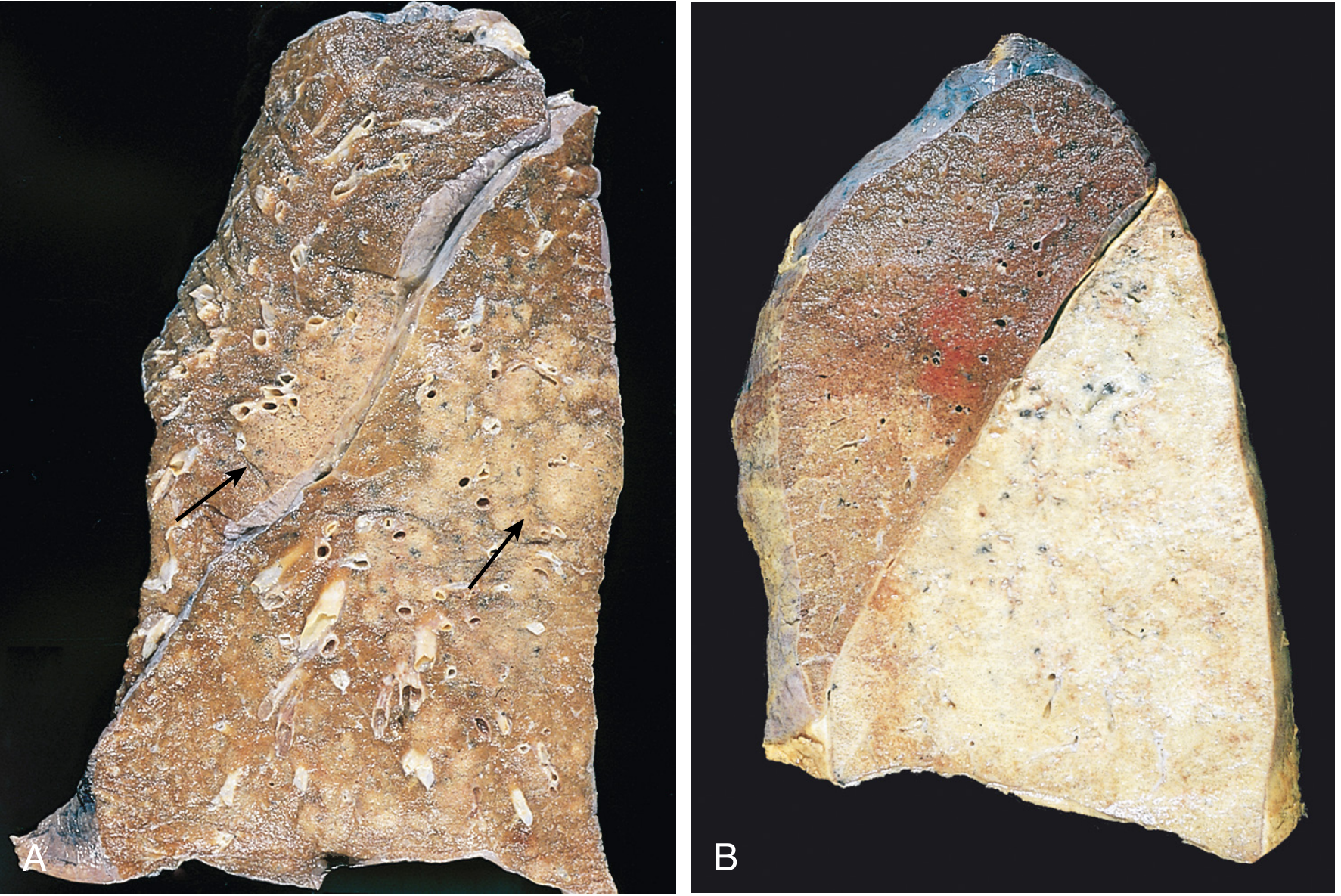
Fig: A - Bronchopneumonia: patchy consolidation (arrows). B - Lobar pneumonia gray hepatization: the entire lower lobe is uniformly consolidated. From Robbins Pathologic Basis of Disease.
| Stage | Gross Appearance | Microscopy |
|---|---|---|
| Stage 1 - Congestion (Day 1-2) | Lung heavy, boggy, red | Vascular engorgement; intra-alveolar edema fluid; few neutrophils; bacteria numerous |
| Stage 2 - Red Hepatization (Day 2-4) | Lobe is red, firm, airless - liver-like consistency | Massive confluent exudate: neutrophils + red blood cells + fibrin fill alveolar spaces |
| Stage 3 - Gray Hepatization (Day 4-8) | Lobe grayish-brown | Progressive disintegration of red cells; fibrinopurulent exudate persists; WBCs remain |
| Stage 4 - Resolution (Day 8+) | Lung re-aerates and returns toward normal | Enzymatic digestion of exudate; macrophage phagocytosis; re-absorption; pneumococci phagocytosed and digested intracellularly |
Pleural fibrinous reaction (pleuritis) is present early if consolidation reaches the lung surface; may resolve or leave fibrous thickening/adhesions. Alveolar walls remain intact throughout.
CLINICAL MANIFESTATIONS
Onset: Characteristically sudden ("abrupt")
Symptoms:
- High fever (39-40°C) with rigors and chills
- Sharp, stabbing pleuritic chest pain - accentuated by inspiration/cough (due to pleural involvement)
- Cough - initially dry, then productive
- Rusty/blood-tinged sputum - pathognomonic; due to red cells and hemoglobin in alveolar exudate (degraded hemoglobin = rust color in stage 2-3)
- Breathlessness (tachypnea, dyspnea)
- Tachycardia
- Myalgias, arthralgias, vomiting, diarrhea may accompany
- Older patients may present with delirium as the first sign
Signs of consolidation on examination:
- Reduced chest expansion on affected side
- Increased tactile vocal fremitus (TVF)
- Dull percussion note
- Bronchial breath sounds
- Crackling (crepitant) rales - localized to the involved lobe
- Pleural friction rub if pleuritis present
Bacteremia: Present in 10-20% of cases early in the febrile phase.
SUPPURATIVE COMPLICATIONS
(Arise from local extension or direct spread)
- Empyema thoracis - pus in the pleural cavity; the most common suppurative complication; results from spread of infection to the pleural space forming a fibrinopurulent intrapleural reaction; requires drainage
- Parapneumonic effusion - initially sterile pleural effusion adjacent to pneumonia; may progress to empyema if untreated
- Lung abscess - less common with pneumococcus (more typical with S. aureus, Klebsiella, anaerobes); occurs when tissue necrosis exceeds resolution capacity
- Necrotizing pneumonia - extensive parenchymal destruction with multiple microabscesses
- Pericarditis - direct extension or hematogenous; purulent pericarditis
- Bacteremia / Pneumococcal septicemia - occurs in 10-20%; leading to systemic metastatic complications
NON-SUPPURATIVE (METASTATIC/SYSTEMIC) COMPLICATIONS
(Arise from bacteremic spread to distant sterile sites)
- Meningitis - most feared complication; confusion, obtundation, and stiff neck should prompt urgent evaluation; pneumococcal meningitis has high mortality
- Endocarditis - seeding of heart valves; acute pneumococcal endocarditis
- Septic arthritis - joint infection via hematogenous spread
- Peritonitis - especially in patients with ascites
- Overwhelming pneumococcal sepsis (OPSI) - greatest risk in asplenic patients (spleen is the principal site for clearance of encapsulated bacteria)
- Major cardiovascular events - up to 1/3 of hospitalized patients develop MI, arrhythmias, or heart failure; pneumolysin directly injures myocardium
- Otitis media / Sinusitis - by contiguous or hematogenous spread
- ARDS - in overwhelming/severe disease
LABORATORY DIAGNOSIS
1. Specimen Collection
- Sputum: Actual sputum, not saliva; valid if >25 PMNs and <10 squamous epithelial cells per low-power field
- Blood cultures: 2 sets before antibiotics; yield 5-15%; S. pneumoniae accounts for ~2/3 of positives
- CSF if meningitis suspected
- Pleural fluid if effusion present
- Urine for antigen detection
2. Direct Gram Stain of Sputum
- Gram-positive, lancet-shaped diplococci (candle-flame shape), often surrounded by a clear halo (capsule)
- Rapid, highly specific
- Can detect pneumococci in 60-80% of confirmed cases
3. Culture
- Media: Blood agar (5% sheep blood) or chocolate agar; CO2 incubation at 37°C
- Colonies: Alpha-hemolytic (green halo), 1-2 mm; "draughtsman" or "checker" colonies (central depression due to autolytic collapse)
- Identification:
- Optochin (P disk) sensitivity test - zone of inhibition >14 mm distinguishes S. pneumoniae from viridans streptococci (which are optochin resistant)
- Bile solubility test - colonies dissolve in sodium deoxycholate (positive = S. pneumoniae; viridans streptococci are bile-resistant)
4. Quellung (Capsular Swelling) Reaction
- Mixing pneumococci with type-specific antiserum or polyvalent "omniserum" causes the capsule to swell visibly and organisms agglutinate
- Useful for rapid identification and serotyping directly from sputum
- Rarely used now due to high reagent cost and expertise required
5. Urinary Antigen Detection
- Detects pneumococcal C-polysaccharide (common to all 91 serotypes) in urine by immunochromatography
- Sensitivity: 50-80%; Specificity: >90%
- Useful when cultures cannot be obtained in time or antibiotics already started
- C-polysaccharide also detectable in CSF
6. Molecular Methods (PCR/NAAT)
- Highly sensitive and specific; unaffected by prior antibiotic use
- Detects multiple pathogens (bacteria + viruses) from a single respiratory sample
- Increasingly standard of care
7. Imaging
- Chest X-ray: Homogeneous lobar or segmental alveolar infiltrate; air bronchograms (airways visible against background of fluid-filled alveoli) - characteristic; small pleural effusion common
- CT chest: Better defines complications (abscess, empyema, adenopathy)
- Lung ultrasound: Shows subpleural consolidation, hepatization pattern
8. Blood Tests
- CBC: Leukocytosis with left shift (neutrophilia + band forms); leukopenia = poor prognosis
- Elevated CRP, ESR, procalcitonin
TREATMENT
Start empirically as soon as possible:
| Clinical Setting | Treatment |
|---|---|
| Outpatient (mild, non-severe) | Amoxicillin 500mg-1g TID; OR Azithromycin (low resistance area); OR Doxycycline |
| Hospitalized (non-ICU) | IV Ceftriaxone or Ampicillin-sulbactam + Azithromycin |
| Hospitalized (ICU/severe) | IV Beta-lactam (ceftriaxone/cefotaxime) + Azithromycin OR respiratory fluoroquinolone monotherapy (levofloxacin/moxifloxacin) |
| Confirmed penicillin-sensitive | Penicillin G IV (drug of choice) or oral amoxicillin |
| Penicillin allergy (mild) | Third-generation cephalosporin |
| Penicillin allergy (anaphylaxis) | Respiratory fluoroquinolone (levofloxacin/moxifloxacin) |
| Drug-resistant S. pneumoniae | Vancomycin + ceftriaxone; or respiratory fluoroquinolone |
Duration: 5 days if clinical improvement within 72-96 hours.
Prevention: PCV13 (conjugate) + PPSV23 (polysaccharide) vaccines for elderly, immunocompromised, and asplenic patients; Hib vaccine for children.
PART 2: HAEMOPHILUS INFLUENZAE PNEUMONIA
DEFINITION
Pneumonia caused by Haemophilus influenzae, a small pleomorphic Gram-negative coccobacillus requiring X factor (hemin) and V factor (NAD) for growth. It causes predominantly bronchopneumonia (patchy lobular consolidation) rather than true lobar pneumonia. Since widespread Hib vaccination, most pneumonia is caused by non-typeable (non-encapsulated) strains, predominantly in adults with underlying lung disease.
MICROBIOLOGY
- Morphology: Small (0.3-0.5 x 1.5 µm), pleomorphic Gram-negative rods (coccobacilli to long filaments)
- Capsule: Type b capsule contains polyribosylribitol phosphate (PRP) - main virulence factor; 6 capsular types (a-f); non-typeable strains lack a capsule
- Growth requirements: Requires both X factor (hemin, heat-stable) and V factor (NAD, heat-labile) - hence grows on chocolate agar (but not plain blood agar where V-factor inhibitors persist)
- Satellite phenomenon: Grows as tiny satellite colonies around S. aureus on plain blood agar (S. aureus lyses RBCs to release X factor and excretes NAD as V factor)
- Facultative anaerobe (under anaerobic conditions does not require X factor)
PATHOGENESIS
Risk groups
- Adults with COPD (most important) - H. influenzae is the most common bacterial cause of acute COPD exacerbations
- Smokers (damaged mucociliary escalator)
- Diabetics, patients with congestive heart failure
- Elderly patients
- Children (pre-vaccine era): Hib caused meningitis, epiglottitis, pneumonia in children <5 years
Mechanism
- Organisms colonize oropharynx, then descend to lower respiratory tract
- Non-typeable strains use adhesins (Hap, pili, OMP P2, P5) to attach to damaged respiratory epithelium
- IgA protease cleaves secretory IgA
- Lipooligosaccharide (LOS/endotoxin) triggers inflammatory cascade
- Dense fibrin-rich exudates containing neutrophils plug the smaller bronchi
- Consolidation is usually lobular and patchy (bronchopneumonia) but may become confluent and involve an entire lobe
CLINICAL MANIFESTATIONS
- Onset: subacute to acute
- Fever, productive cough with purulent sputum
- Pleuritic chest pain (less prominent than pneumococcal)
- Tachypnea, breathlessness
- Signs of consolidation on examination
- Often follows a viral upper respiratory tract infection (secondary bacterial pneumonia)
- In children (Hib): high-mortality pneumonia; descending laryngotracheobronchitis with airway obstruction from fibrin-rich exudate plugging small bronchi
SUPPURATIVE COMPLICATIONS
- Pleural effusion and empyema - especially with Hib in children
- Bacteremia - leads to metastatic infections
- Lung abscess - less common
- In children (Hib, pre-vaccine era) - hematogenous spread to:
- Meningitis (commonest cause of bacterial meningitis in children <5 years, pre-vaccine)
- Epiglottitis (supraglottitis) - life-threatening airway emergency
- Septic arthritis
- Pericarditis, cellulitis (orbital, buccal), osteomyelitis
NON-SUPPURATIVE COMPLICATIONS
- COPD exacerbations (chronic recurrent inflammation)
- Pyelonephritis, cholecystitis, endocarditis (predisposed adults, rare)
LABORATORY DIAGNOSIS
1. Specimen Collection
- Sputum (from lower airways, minimizing oral contamination)
- Blood cultures (2 sets before antibiotics)
- CSF + blood if meningitis suspected
- Direct needle aspiration for sinusitis/otitis
2. Gram Stain
- Gram-negative coccobacilli (small rods ranging from coccobacilli to long pleomorphic filaments)
- Detected in >80% of CSF in untreated Hib meningitis
- Useful for rapid diagnosis in pneumonia and arthritis
3. Culture
- Media: Chocolate agar - essential; X and V factors are released by heated RBCs and V-factor inhibitors destroyed; incubate at 37°C in 5-10% CO2
- Colonies: 1-2 mm, smooth, opaque after 24 hours
- Satellite phenomenon on plain blood agar around S. aureus colonies (diagnostic clue)
- Blood cultures: growth often delayed (commercial media may not have optimal X+V factor concentrations)
4. Identification
- X and V factor requirement: Spot tests with X, V, and X+V disks on factor-free media; H. influenzae grows only around X+V disk
- Biotype determination by biochemical tests
5. Antigen Detection (for Hib only)
- Latex particle agglutination detects PRP capsular antigen in CSF and urine
- Detects <1 ng/mL of PRP
- Limitation: Only detects type b; not useful for non-typeable strains (now more common)
6. Molecular Methods
- PCR detects H. influenzae from respiratory specimens; useful after antibiotic treatment
7. Imaging
- Patchy bilateral or unilateral bronchopneumonia
- May show segmental/lobar consolidation
- Spherical pneumonia possible in children (rounded edges; due to exudate spread through pores of Kohn)
TREATMENT
| Strain | Treatment |
|---|---|
| Ampicillin-sensitive (beta-lactamase negative) | Ampicillin IV or oral amoxicillin |
| Beta-lactamase producing strains (~30-40%) | Amoxicillin-clavulanate oral; Ampicillin-sulbactam IV |
| Severe / hospitalized | Ceftriaxone or Cefotaxime IV |
| Meningitis (Hib) | Ceftriaxone (drug of choice); dexamethasone as adjunct |
| COPD exacerbation | Amoxicillin-clavulanate, doxycycline, or azithromycin |
| Multidrug resistant | Fluoroquinolone (levofloxacin) or carbapenem |
Resistance mechanism: Beta-lactamase production (TEM-1 type) - the main mechanism in ~30-40% of strains. Always test susceptibility.
Prevention: Hib conjugate vaccine - has nearly eliminated invasive Hib disease in children; does not protect against non-typeable strains.
PART 3: ATYPICAL PNEUMONIA
DEFINITION
Atypical pneumonia is a clinical syndrome of pneumonia caused by organisms that:
- Cannot be seen on Gram stain (intracellular, lack cell walls, or stain poorly)
- Do not grow on standard bacteriologic media
- Are resistant to beta-lactam antibiotics
- Produce a milder, more indolent clinical picture ("walking pneumonia")
- Cause predominantly interstitial (not alveolar) infiltrates on chest X-ray
The syndrome was first recognized in the 1930s when some patients with pneumonia had milder symptoms than typical S. pneumoniae pneumonia.
CAUSATIVE ORGANISMS
| Category | Organism |
|---|---|
| Mycoplasma (most common - up to 15% of outpatient CAP) | Mycoplasma pneumoniae |
| Chlamydophila | C. pneumoniae, C. psittaci (psittacosis from birds) |
| Legionella (1-10% of CAP; can be severe) | Legionella pneumophila |
| Rickettsia | Coxiella burnetii (Q fever) |
| Viruses (30% of CAP) | Influenza, adenovirus, RSV, parainfluenza, metapneumovirus, varicella-zoster, measles, EBV, CMV, Hantavirus |
| Fungi | Histoplasma, Blastomyces, Coccidioides, Pneumocystis jirovecii |
| Bioterrorism agents | Francisella tularensis, Yersinia pestis, Bacillus anthracis |
MYCOPLASMA PNEUMONIAE (Primary Atypical Pneumonia) - THE PROTOTYPE
Microbiology
- Smallest free-living self-replicating organism
- NO CELL WALL - hence beta-lactams, vancomycin, and all cell-wall-active antibiotics are completely ineffective
- Pleomorphic (no fixed shape)
- Very slow growing on artificial media; cannot be detected on Gram stain
- Eaton agent (originally thought to be a virus)
Pathogenesis
- Transmitted by respiratory droplets (requires close, prolonged contact)
- Incubation period: 2-3 weeks (long - explains why household/school outbreaks may go unrecognized)
- Community-wide epidemics every 4-7 years
- Organism attaches to respiratory epithelium via P1 adhesin (tip structure)
- Damages ciliated cells - ciliastasis (paralysis of cilia)
- Produces hydrogen peroxide and superoxide radicals - oxidative injury to epithelium
- Triggers intense lymphocytic and monocytic interstitial inflammation (interstitial pneumonitis)
Clinical Manifestations
- Most common in young adults, school-age children, college students, military recruits
- Insidious onset (gradual, over days to a week)
- Malaise, low-grade fever
- Prominent headache - more prominent than in typical pneumonia
- Sore throat (common), minimal coryza
- Dry, non-productive cough - the hallmark; develops progressively over days
- Myalgias, arthralgias
- Patients feel sick but often continue daily activities - hence "walking pneumonia"
Extrapulmonary manifestations (due to immune mechanisms):
- Bullous myringitis (vesicular hemorrhagic blebs on tympanic membrane) - highly characteristic when present
- Skin rashes (maculopapular, erythema multiforme)
- Ear pain, otitis media
SUPPURATIVE COMPLICATIONS
- Small pleural effusion (uncommon)
- Secondary bacterial superinfection
- Lung abscess (very rare)
NON-SUPPURATIVE (EXTRAPULMONARY) COMPLICATIONS
(Immune-mediated, not due to direct bacterial invasion)
- Cold agglutinin hemolytic anemia - most classic complication; IgM anti-I antibodies agglutinate RBCs at 4°C; may cause intravascular hemolysis and jaundice; can precipitate Raynaud's phenomenon
- Stevens-Johnson syndrome / Erythema multiforme - mucocutaneous immune reaction
- Bullous myringitis - hemorrhagic blisters on tympanic membrane
- Neurological complications: Meningoencephalitis, cerebellar ataxia, Guillain-Barre syndrome, transverse myelitis, peripheral neuropathy
- Cardiac: Myocarditis, pericarditis, complete heart block (rare)
- Gastrointestinal: Hepatitis, nausea/vomiting/diarrhea, pancreatitis (rare)
- Reactive arthritis
- Glomerulonephritis (rare, immune-complex mediated)
LABORATORY DIAGNOSIS OF ATYPICAL PNEUMONIA
1. Chest X-Ray
- Interstitial infiltrates - bilateral, peribronchial, reticular pattern; "shaggy heart" border
- X-ray-clinical dissociation - X-ray looks much worse than the patient appears clinically (classic teaching point)
- Usually unilateral lower lobe but may be bilateral
- Small pleural effusion in some cases
2. Cold Agglutinin Test (Mycoplasma-specific pointer)
- Cold agglutinins = IgM antibodies against the I antigen on human group O RBCs; agglutinate at 4°C, dissolve at 37°C
- Positive in ~50-70% of Mycoplasma pneumonia cases
- Bedside test: Blood in a glass tube, put in ice bucket for 2-3 minutes - visible agglutination = positive; re-warm in hand and agglutinate dissolves = cold agglutinin confirmed
- Significant titer: ≥1:32; highly suggestive: ≥1:64
- Not specific - can be positive in EBV, CMV, adenovirus, influenza
3. Serology
- Complement Fixation (CF) test: Fourfold or greater rise in CF antibody titer between acute serum (day 1) and convalescent serum (2-3 weeks later) is diagnostic
- ELISA: Detection of specific IgM (acute infection; appears at 7-10 days, peaks at 3-4 weeks) and IgG (past infection or convalescence)
- Paired serology is confirmatory but retrospective
4. Culture
- Impractical clinically - organisms grow on SP4 medium (special broth/agar) or Hayflick medium over weeks
- Colonies show "fried-egg" appearance under microscope
- Rarely done in routine diagnosis
5. PCR / Molecular Methods (Preferred)
- Most sensitive and specific
- Detects Mycoplasma DNA from nasopharyngeal swab, sputum, or BAL
- Can simultaneously detect Chlamydophila, Legionella, and respiratory viruses
- Rapid (hours); unaffected by prior antibiotic therapy
- Increasingly the standard of care for atypical pneumonia
6. Legionella-Specific Tests
- Urinary antigen test - detects L. pneumophila serogroup 1 (sensitivity 70-90%, specificity >99%); rapid, reliable; test of choice for Legionella
- Culture: BCYE (buffered charcoal yeast extract) agar - specific for Legionella; takes 3-5 days
- DFA (Direct Fluorescent Antibody) test on sputum/BAL
7. Chlamydophila
- Micro-immunofluorescence (MIF) test - reference standard for serology
- PCR from respiratory specimens
TREATMENT OF ATYPICAL PNEUMONIA
| Organism | First-line | Duration |
|---|---|---|
| Mycoplasma pneumoniae | Azithromycin 500mg day 1, then 250mg days 2-5; OR Doxycycline 100mg BD | 5 days (azithromycin); 10-14 days (doxy) |
| Chlamydophila pneumoniae | Doxycycline 100mg BD OR Azithromycin | 10-14 days |
| Chlamydophila psittaci (psittacosis) | Doxycycline 100mg BD (drug of choice) | 14-21 days |
| Legionella pneumophila | Azithromycin IV/oral OR Levofloxacin 750mg OD | 5-10 days (azithromycin); 7-10 days (fluoroquinolone) |
| Coxiella burnetii (Q fever) | Doxycycline 100mg BD | 14 days |
Key principle: Beta-lactams are completely INEFFECTIVE for atypical pneumonia (no cell wall target for Mycoplasma; intracellular location protects Chlamydophila; Legionella is intracellular).
For empirical CAP therapy where atypical organisms must also be covered: fluoroquinolones (levofloxacin, moxifloxacin) cover both typical and atypical organisms.
COMPREHENSIVE COMPARISON TABLE
| Feature | Lobar Pneumonia (S. pneumoniae) | H. influenzae Pneumonia | Atypical Pneumonia (Mycoplasma) |
|---|---|---|---|
| Causative agent | S. pneumoniae (Gram+ diplococci) | H. influenzae (Gram- coccobacilli) | M. pneumoniae (no cell wall) |
| Pattern | Lobar consolidation | Bronchopneumonia (patchy, lobular) | Interstitial infiltrate |
| Onset | Sudden, explosive | Subacute to acute | Insidious, gradual |
| Sputum | Rusty/blood-tinged, purulent | Purulent, greenish-yellow | Dry, scanty, non-productive |
| Pleuritic pain | Prominent | Less prominent | Mild or absent |
| X-ray | Homogeneous lobar infiltrate, air bronchograms | Patchy lobular consolidation | Interstitial/peribronchial; worse than clinical findings |
| Gram stain | Gram+ lancet-shaped diplococci with halo | Gram- coccobacilli to pleomorphic rods | Not visible on Gram stain |
| Culture media | Blood/chocolate agar + CO2 | Chocolate agar only (X+V factors needed) | SP4/Hayflick medium; rarely cultured |
| Key lab test | Gram stain + culture; urinary antigen; Quellung | Chocolate agar culture; satellite phenomenon; X+V factor requirement | Cold agglutinins; PCR; serology (IgM ELISA) |
| Key suppurative complication | Empyema, lung abscess, bacteremia, pericarditis | Empyema; meningitis (Hib children) | Pleural effusion (small), rare abscess |
| Key non-suppurative complication | Meningitis, endocarditis, septic arthritis, cardiovascular events | Meningitis/epiglottitis (Hib pre-vaccine) | Cold agglutinin hemolytic anemia, Stevens-Johnson syndrome, neurological |
| Treatment | Penicillin G / Amoxicillin; ceftriaxone; fluoroquinolone | Amoxicillin-clavulanate; ceftriaxone (beta-lactamase producers) | Azithromycin or Doxycycline (NO beta-lactams) |
| Vaccine | PCV13 + PPSV23 | Hib conjugate vaccine (children) | None available |
Sources consulted:
- Jawetz Melnick & Adelberg's Medical Microbiology 28e
- Robbins & Cotran Pathologic Basis of Disease (Robbins, Kumar, Abbas)
- Goldman-Cecil Medicine International Edition
- Harrison's Principles of Internal Medicine 22e (2025)
- Fishman's Pulmonary Diseases and Disorders
- Medical Microbiology 9e (Murray, Rosenthal, Pfaller)
This is a shared conversation. Sign in to Orris to start your own chat.