Randomized control trial
Reading File
Searching the Web
randomized controlled trial design methodology overview 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of Randomized Controlled Trials (RCTs), synthesized from authoritative medical textbooks.
Randomized Controlled Trial (RCT)
Definition
An RCT is an epidemiological experiment and the gold standard method for evaluating therapeutic or preventive interventions. Participants are randomly allocated to an experimental group (receives the intervention) or a control group (receives placebo, standard care, or no treatment), and outcomes are measured prospectively.
"A randomized controlled trial (RCT) is often considered the gold standard for making causal inferences."
- Smith and Tanagho's General Urology
Design Diagram
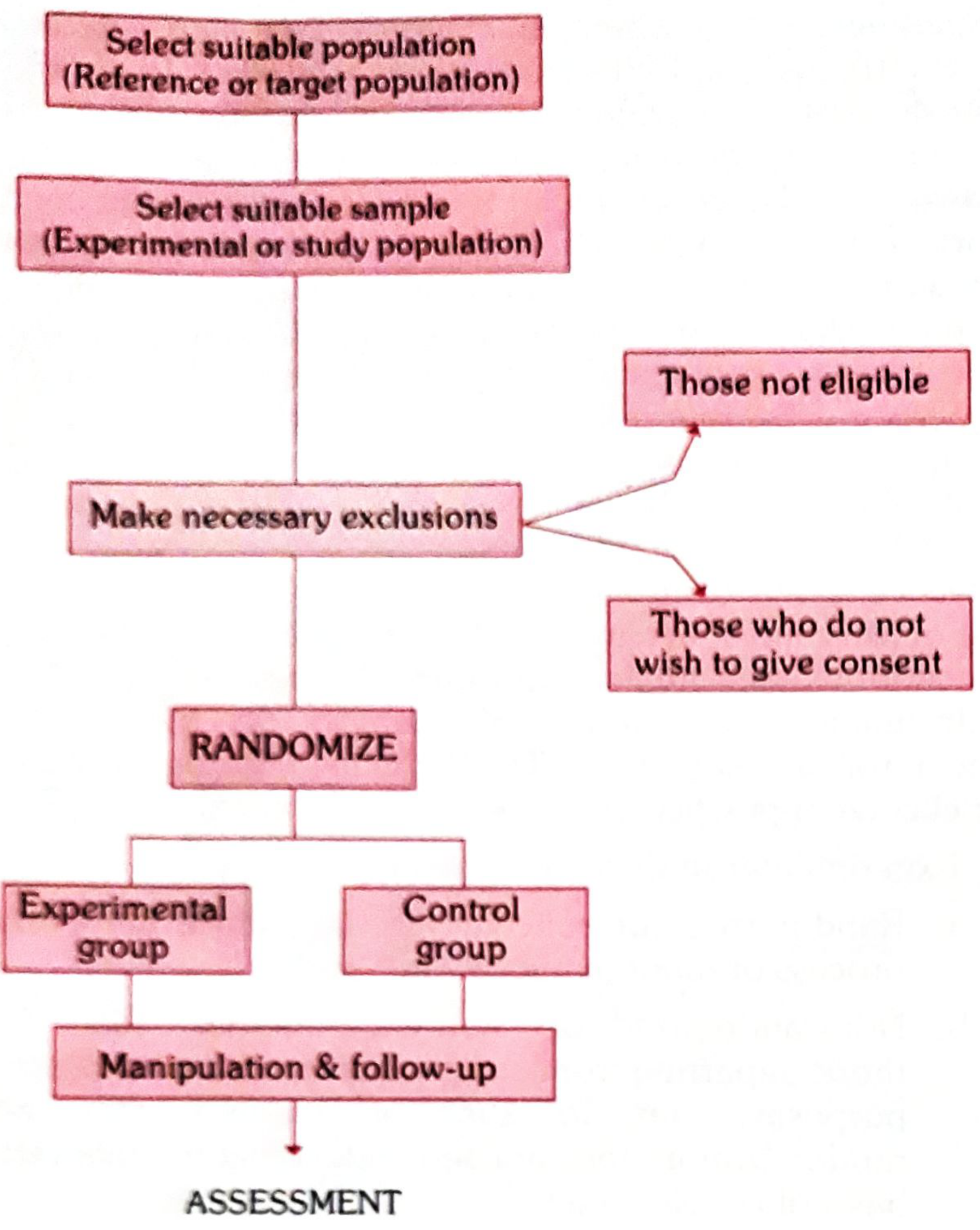
Basic Steps in Conducting an RCT
(Park's Textbook of Preventive and Social Medicine)
| Step | Description |
|---|---|
| 1. Protocol | Specifies aims, eligibility criteria, sample size, intervention procedures, and outcome evaluation. A pilot study may be run first. |
| 2. Selecting populations | Define the reference (target) population and the experimental (study) population - who must give informed consent, be representative, and be eligible. |
| 3. Randomization | Statistical procedure to allocate participants into groups, eliminating selection bias. Every individual has an equal chance of assignment. |
| 4. Intervention | Administer the experimental treatment or placebo/comparator. |
| 5. Follow-up | Prospective monitoring of both groups over the study period. |
| 6. Assessment of outcome | Compare results between groups to determine intervention effect. |
Randomization - The Heart of an RCT
Randomization ensures like is compared with like by distributing both known and unknown confounders equally across groups. It prevents selection bias - the investigator has no control over which group a participant enters.
- Simple randomization - random number tables or computer-generated sequences
- Stratified randomization - population subdivided by key variables (e.g. age, sex) before randomization, ensuring balance on those variables
Blinding
Randomization alone cannot prevent bias in outcome assessment. Blinding addresses this:
| Type | Who is Blinded |
|---|---|
| Single-blind | Participant does not know their group assignment |
| Double-blind | Neither participant nor investigator knows group assignment |
| Triple-blind | Participant, investigator, AND data analyst are all blinded - the ideal, though least common |
Double-blind is the most commonly used method. When the outcome is objective (e.g., death), blinding is less critical.
Three Major Confounding Factors in Drug RCTs
(Katzung's Basic and Clinical Pharmacology)
- Variable natural history of disease - Many diseases fluctuate spontaneously; a crossover design or large enough population over sufficient time guards against misattribution.
- Presence of other diseases and risk factors - Comorbidities, concurrent drugs, and lifestyle factors can influence results. Careful patient selection and accurate histories are required.
- Subject and observer bias - The placebo effect can produce objective physiological changes in 30-40% of subjects. Single- and double-blind designs are used to quantify and minimize this.
Common RCT Designs
| Design | Description |
|---|---|
| Concurrent parallel | Two randomly assigned groups run simultaneously; one receives treatment, the other does not |
| Crossover | Each participant serves as their own control; groups switch interventions after a washout period. More efficient (fewer patients needed) but unsuitable if the treatment cures the disease or effects carry over |
| Adaptive design | Pre-specified rules allow trial modifications (e.g., sample size adjustment) based on interim data |
| Platform trial | Multiple interventions tested simultaneously within a single trial infrastructure |
| Stepped-wedge | All clusters eventually receive the intervention, but in a randomized order over time |
Clinical Trial Phases
(Berek & Novak's Gynecology)
| Phase | Purpose | Participants |
|---|---|---|
| Phase I | Safety, safe dosage range | 20-100 healthy volunteers or patients |
| Phase II | Efficacy, further safety assessment | Up to several hundred patients |
| Phase III | Definitive efficacy, comparison with existing treatments, adverse events | 30-3,000+ participants, often within RCTs |
| Phase IV | Post-marketing surveillance; rare adverse events, optimal use in subgroups | Thousands, in registries and observational studies |
CONSORT Checklist
The Consolidated Standards of Reporting Trials (CONSORT) Statement provides a 25-item checklist and flow diagram for transparent reporting of RCT findings. All published RCTs are expected to:
- Report baseline comparability of groups
- State the randomization method and allocation concealment
- Define outcomes a priori with adequate statistical power
- Register the trial in a public registry before enrollment begins
Strengths and Limitations
Strengths:
- Minimizes confounding via randomization
- Allows causal inference (intervention → outcome)
- Double-blinding controls for placebo effect and observer bias
Limitations:
- Expensive and time-consuming
- Ethical constraints (cannot randomize to harmful exposures)
- Strict eligibility criteria reduce generalizability
- Not always feasible (rare diseases, long latency outcomes)
- A well-run RCT still depends on the right question being asked and the right population being enrolled
Sources: Park's Textbook of Preventive and Social Medicine | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Berek & Novak's Gynecology | Smith and Tanagho's General Urology, 19th Ed.
Randomized control trial
I just covered RCTs in detail in my previous response. Let me know if you'd like me to go deeper on any specific aspect:
- Randomization methods (simple, block, stratified, cluster)
- Blinding techniques (single, double, triple blind)
- RCT designs (parallel, crossover, factorial, adaptive, platform)
- Statistical concepts (power, sample size, p-value, confidence intervals, ITT vs per-protocol analysis)
- Bias types (selection, performance, detection, attrition, reporting)
- CONSORT guidelines and reporting standards
- Ethical considerations (informed consent, equipoise, stopping rules)
- Clinical trial phases (I-IV)
- Advantages and limitations of RCTs vs other study designs
Which area would you like to explore?
Steps in RCT
Reading File
Finding Sources
Searching the Web
steps in conducting a randomized controlled trial protocol to reporting
Finding Sources
Reading File
Reading File
Here is a detailed, step-by-step breakdown of how an RCT is conducted, drawn directly from Park's Textbook of Preventive and Social Medicine.
Steps in Conducting an RCT
Step 1 - Drawing Up a Protocol
The protocol is the master plan of the entire trial. It must be agreed upon by all parties before the study begins and adhered to strictly throughout.
The protocol specifies:
- Aims and objectives of the study
- Research question(s) to be answered
- Inclusion and exclusion criteria for participant selection
- Sample size calculation
- Procedures for allocating subjects to study vs. control groups
- Treatment details - what, when, how, and to whom
- Standardized working procedures and schedules
- Roles and responsibilities of all parties involved
- How outcome will be measured and evaluated
Pilot study / Preliminary test run: Before finalizing the protocol, a short pilot run may be done to check feasibility, detect flaws, or assess acceptability of procedures. The final protocol is only locked after all issues are resolved.
Step 2 - Selecting Reference and Experimental Populations
(a) Reference (Target) Population
The population to which the trial results will be generalized if the intervention proves successful. It can be:
- As broad as all of mankind
- Geographically limited (e.g., a city)
- Defined by age, sex, occupation, or clinical condition (e.g., school children, obstetric population)
(b) Experimental (Study) Population
Derived from the reference population - the actual people who participate. Ideally randomly chosen from the reference population so their characteristics match it.
Three criteria every participant must meet:
| Criterion | Explanation |
|---|---|
| Informed consent | Participant must voluntarily agree after being fully informed of purpose, procedures, and possible risks |
| Representativeness | Must represent the reference population so findings can be generalized |
| Eligibility | Must be susceptible to / affected by the condition under study (e.g., anaemic for an anaemia drug trial; unimmunized for a vaccine trial) |
Note: Persons who volunteer to participate often differ from those who do not - this can affect outcome interpretation.
Step 3 - Randomization
Randomization is the "heart" of a controlled trial. It is the statistical procedure by which participants are allocated into study and control groups.
Why randomize?
- Eliminates selection bias - investigator has no control over group assignment
- Distributes both known AND unknown confounders equally between groups
- Ensures "like is compared with like"
- Every individual gets an equal chance of being in either group
Methods of randomization:
| Method | Description |
|---|---|
| Simple randomization | Random number table or computer-generated sequence |
| Stratified randomization | Population divided into subgroups (e.g., by age, sex) first, then randomized within each subgroup to ensure balance |
| Cluster randomization | Groups (e.g., villages, schools) rather than individuals are randomized |
| Block randomization | Ensures equal group sizes at regular intervals throughout the trial |
Randomization is done only after the participant has entered the study (i.e., after consent and eligibility confirmation), never before.
Step 4 - Manipulation / Intervention
The experimental group receives the intervention (new drug, vaccine, procedure). The control group receives:
- A placebo (inert preparation identical in appearance to the active treatment), OR
- Standard/conventional treatment, OR
- No treatment (where ethically permissible)
Blinding is applied at this stage to prevent bias:
| Type | Who is Blinded |
|---|---|
| Single-blind | Participant only |
| Double-blind | Both participant and investigator |
| Triple-blind | Participant, investigator, AND data analyst |
Why placebo? The placebo effect can produce a positive response in 30-40% of subjects. Using a placebo controls for this psychological response, ensuring any measured benefit is due to the intervention itself.
Step 5 - Follow-Up
Both groups are monitored prospectively over the study period.
Key considerations:
- Follow-up must be equal and complete in both groups
- Losses to follow-up (dropouts) must be minimized - they can introduce bias
- A stable, cooperative population should be selected from the outset to reduce attrition
- In a crossover design, after a washout period (to clear the first treatment from the body), the two groups switch interventions - each participant serves as their own control
Step 6 - Assessment of Outcome
Outcomes are measured and compared between groups.
Key principles:
- Outcomes must be pre-specified (a priori) in the protocol - changing outcomes after seeing data ("outcome switching") is a major source of bias
- Assessment must be objective, ideally by blinded assessors
- The trial must have sufficient statistical power to detect the expected treatment effect (adequate sample size)
Analysis approaches:
| Approach | Description |
|---|---|
| Intention-to-treat (ITT) | All randomized participants analyzed in their original assigned group, regardless of whether they completed the protocol - preserves randomization |
| Per-protocol analysis | Only participants who fully adhered to the protocol are analyzed - can overestimate efficacy |
Summary Flowchart
Protocol Development
↓
Population Selection (Reference → Experimental)
↓
Eligibility Screening + Informed Consent
↓
Randomization
↙ ↘
Experimental Control
Group Group
(Intervention) (Placebo/Standard)
↓
Follow-Up
↓
Outcome Assessment
↓
Statistical Analysis
↓
Reporting (CONSORT)
Source: Park's Textbook of Preventive and Social Medicine
Use of epidemiology
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Use of epidemiology
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.