Lasers used in ophthalmology
Reading File
Finding Sources
Searching the Web
lasers used in ophthalmology types applications 2024
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
laser photocoagulation retina diabetic retinopathy ophthalmology
I now have comprehensive data from Kanski's Clinical Ophthalmology, Bailey & Love's, Wills Eye Manual, and supporting sources. Here is the full synthesis:
Lasers in Ophthalmology
Physics & Tissue Interactions
The word LASER stands for Light Amplification by Stimulated Emission of Radiation. In ophthalmology, lasers exploit three main tissue interactions:
| Interaction | Mechanism | Example |
|---|---|---|
| Photocoagulation | Thermal absorption → protein coagulation | Argon, diode laser on retina |
| Photodisruption | Plasma formation → mechanical disruption | Nd:YAG on posterior capsule/iris |
| Photoablation | Bond breaking (UV photons) → precise tissue removal | Excimer laser on cornea |
Visible and infrared (IR) lasers work primarily by heating tissue; UV lasers (excimer) work by photodissociation of molecular bonds.
Classification of Ophthalmic Lasers
1. Argon Laser (488 nm / 514 nm – blue-green)
- Mechanism: Thermal photocoagulation
- Applications:
- Panretinal photocoagulation (PRP): First-line for proliferative diabetic retinopathy — ablates ischaemic peripheral retina, reducing VEGF drive
- Focal/grid laser: For diabetic macular oedema (focal leaky microaneurysms or grid for diffuse oedema); largely superseded by anti-VEGF but still used
- Retinal tears/breaks: Seals tears before progression to detachment
- Argon laser trabeculoplasty (ALT): Burns to trabecular meshwork in open-angle glaucoma; thermal damage limits repeatability
2. Diode Laser (810 nm – near-infrared)
- Mechanism: Thermal photocoagulation; better choroidal penetration
- Applications:
- Retinal photocoagulation (alternative to argon)
- Trans-scleral cyclophotocoagulation (TSCPC): Targets ciliary body through the sclera to reduce aqueous production in refractory/secondary glaucoma with uncontrolled IOP — used when trabeculectomy has failed or is contraindicated
- Endocyclophotocoagulation (ECP): Intraocular delivery via endoscope during vitreoretinal surgery
3. Nd:YAG Laser (1064 nm; frequency-doubled 532 nm)
- Mechanism: Photodisruption (plasma-mediated)
- Applications:
- Posterior capsulotomy (PCO): Photodisrupts the opacified posterior capsule ("after-cataract") — this occurs in 5–10% of cases after cataract surgery and is the most common use of Nd:YAG in routine practice
- Laser peripheral iridotomy (LPI): Creates a full-thickness hole in the peripheral iris for acute angle-closure glaucoma; treats both the affected and the fellow eye
- Vitreolysis: Disruption of vitreous floaters (off-label but practised)
4. Selective Laser Trabeculoplasty (SLT) — Frequency-doubled Nd:YAG, 532 nm
- Mechanism: Selectively targets melanin in trabecular meshwork (TM) cells without thermal damage to non-pigmented structures
- Clinical significance: Based on the LiGHT trial (6-year data), SLT is now recommended as first-line treatment for ocular hypertension and primary open-angle glaucoma — patients who had SLT first showed less disease progression and were less likely to require trabeculectomy. IOP reductions of 10–40% can be expected; ~80% of patients will be drop-free at 3 years
- Because there is no thermal tissue damage, treatment can be repeated even after initial failure
- Complications: transient mild inflammation, transient IOP spike (especially in heavily pigmented angles), rare endothelial decompensation
5. Excimer Laser (ArF, 193 nm – ultraviolet)
- Mechanism: Photoablation — breaks molecular bonds with negligible thermal spread; ablates corneal stroma to a precise depth
- Applications (Refractive Surgery):
- Photorefractive keratectomy (PRK): Epithelium removed; stroma ablated directly. Corrects myopia up to ~6 D, astigmatism up to ~3 D, low–moderate hypermetropia. Main disadvantage vs LASIK: slower recovery, more stromal haze
- LASER subepithelial keratectomy (LASEK): Epithelium chemically separated then replaced after ablation
- LASIK (Laser-Assisted in Situ Keratomileusis): Corneal flap created (by microkeratome or femtosecond laser) → stromal ablation by excimer → flap repositioned. Corrects myopia up to 6–8 D, hypermetropia up to 3–4 D, astigmatism up to 5 D. Advantages: faster recovery, better comfort, wider correction range. Risk: flap-related complications
- Wavefront-guided LASIK: Excimer ablation pattern based on wavefront aberrometry measurements to minimise induced higher-order aberrations
6. Femtosecond Laser (1053 nm – infrared, ultrashort pulses)
- Mechanism: Photodisruption at extremely precise focal points
- Applications:
- LASIK flap creation: Produces uniform, precise flap thickness (100–120 μm) — significantly reduces flap-related complications vs mechanical microkeratome
- Small incision lenticule extraction (SMILE): Entirely femtosecond-based; lenticule of stroma removed through small incision — no flap
- Femtosecond-assisted cataract surgery (FLACS): Capsulotomy, lens fragmentation, corneal incisions
- Corneal transplantation: Precise lamellar cuts for DALK, DSAEK
7. Photodynamic Therapy (PDT) — Verteporfin + 689 nm Diode Laser
- Mechanism: Verteporfin (photosensitiser) is infused IV → accumulates in abnormal choroidal neovascular tissue → activated by 689 nm laser → singlet oxygen generation → selective vascular occlusion
- Applications:
- Wet AMD with predominantly classic subfoveal choroidal neovascularisation (CNV)
- Polypoidal choroidal vasculopathy (PCV) — often combined with anti-VEGF
- Chronic central serous chorioretinopathy (CSC) — half-dose or half-fluence PDT
8. Micropulse Laser
- Mechanism: Delivers thermal energy in extremely short pulses with off-time periods; subthreshold — no visible tissue reaction
- Applications:
- Micropulse laser trabeculoplasty (MLT): Comparable IOP lowering to SLT/ALT; no visible burns, no repeat limitations
- Subthreshold micropulse laser (SML): For diabetic macular oedema and central serous chorioretinopathy — as effective as conventional photocoagulation with considerably less retinal damage; onset slower
Summary Table
| Laser | Wavelength | Type | Key Ophthalmic Uses |
|---|---|---|---|
| Argon | 488/514 nm | Photocoagulation | PRP, focal/grid retinal, ALT, retinal tears |
| Diode | 810 nm | Photocoagulation | Retinal, trans-scleral cyclophotocoagulation |
| Nd:YAG | 1064 nm | Photodisruption | Posterior capsulotomy, laser iridotomy |
| SLT (freq-doubled Nd:YAG) | 532 nm | Selective photocoagulation | First-line open-angle glaucoma |
| Excimer (ArF) | 193 nm | Photoablation | PRK, LASIK, LASEK |
| Femtosecond | ~1053 nm | Photodisruption | LASIK flap, SMILE, FLACS, corneal transplant |
| PDT (verteporfin + diode) | 689 nm | Photochemical | Wet AMD, PCV, CSC |
| Micropulse diode | 810 nm | Subthreshold thermal | Macular oedema, SLT equivalent, CSC |
Retina: Panretinal Photocoagulation Post-Treatment Appearance
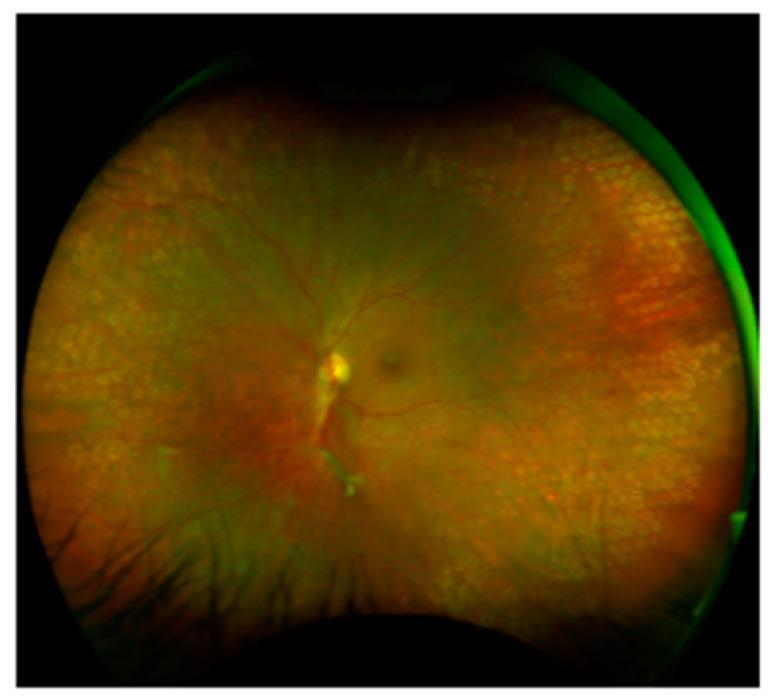
Post-PRP retina showing characteristic pale laser scars (577 nm yellow Pascal laser) across the peripheral retina in proliferative diabetic retinopathy.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. — Chapters on Glaucoma (LTP), Refractive Surgery, Macula
- Bailey & Love's Short Practice of Surgery, 28th ed. — "Lasers in Ophthalmology," p. 757
- The Wills Eye Manual, 8th ed. — Glaucoma, Retina, Cornea sections
- Goodman & Gilman's Pharmacological Basis of Therapeutics — Verteporfin/PDT
- Harrison's Principles of Internal Medicine, 22nd ed. — Diabetic retinopathy laser treatment
This is a shared conversation. Sign in to Orris to start your own chat.