Varicose vein anatomy
Reading File
Finding Sources
Searching the Web
varicose vein anatomy venous system pathophysiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I now have a comprehensive set of information from multiple authoritative textbooks with images. Let me compile the full answer.
Varicose Vein Anatomy
Varicose veins are abnormally dilated, tortuous, elongated superficial veins resulting from prolonged increased intraluminal pressure and subsequent incompetence of venous valves. They occur most commonly in the lower limbs.
The Venous System of the Lower Limb
The lower limb has two interconnected venous systems:
1. Deep venous system
Lies within the muscle compartments, enclosed by deep fascia. Includes the femoral vein (thigh), popliteal vein (behind the knee), and the anterior/posterior tibial and peroneal veins (leg). These veins carry approximately 90% of venous return from the leg.
2. Superficial venous system
Lies in the subcutaneous fat, superficial to the deep fascia. Drains only skin and subcutaneous tissue. The two major trunks are:
- Great Saphenous Vein (GSV) - also called the long saphenous vein. Originates from the medial end of the dorsal venous arch of the foot, passes anterior to the medial malleolus, runs up the medial aspect of the calf and thigh, and terminates by passing through the saphenous opening (cribriform fascia) in the upper thigh to join the common femoral vein at the saphenofemoral junction (SFJ) - also called the saphena varix.
- Small Saphenous Vein (SSV) - also called the short saphenous vein. Runs up the posterior calf and drains into the popliteal vein in the popliteal fossa at the saphenopopliteal junction (SPJ).
3. Perforating (communicating) veins
Connect the superficial to the deep system by traversing the deep fascia. Normally have one-way valves directing flow from superficial to deep. The clinically important perforators include:
- Midthigh perforator - connecting the GSV to the femoral vein
- Calf perforators (Cockett's perforators) - connecting the GSV tributaries to the posterior tibial veins, located at 5, 10, and 15 cm above the medial malleolus
Normal Venous Return Mechanism
Blood in the superficial veins is driven into the deep veins via perforators, then propelled toward the heart by:
- Calf muscle pump - contraction of the soleus and gastrocnemius squeezes the deep veins, generating pressures up to 200 mmHg
- Respiratory pressure changes - negative intrathoracic pressure on inspiration aids venous return
- Competent venous valves - bicuspid valves prevent retrograde flow (reflux) between contractions
Anatomy of Valvular Incompetence - How Varicose Veins Form
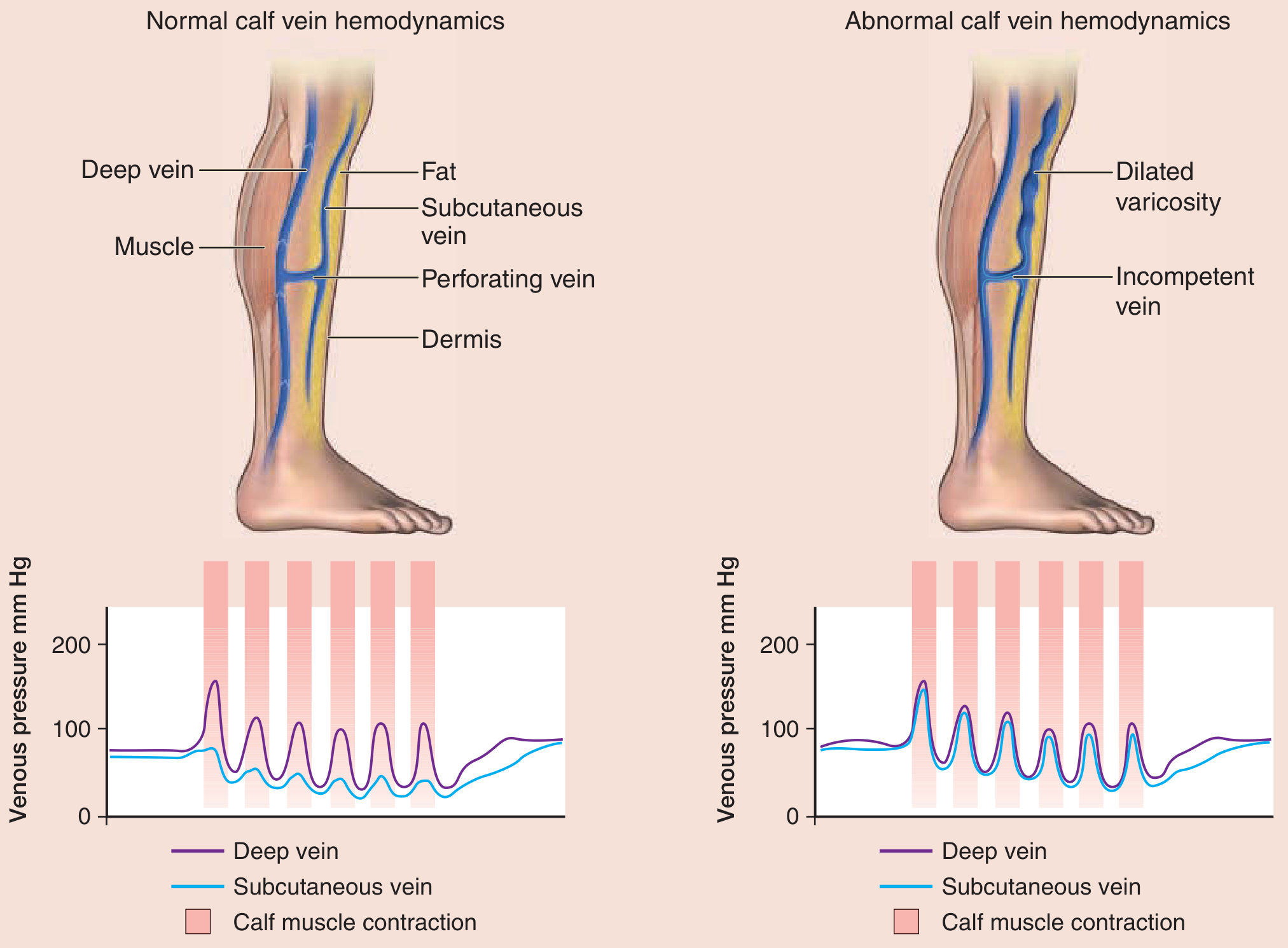
Fig: Normal (left) vs. abnormal (right) calf vein hemodynamics. With incompetent perforating veins, high-pressure deep venous blood refluxes into the unsupported superficial veins, causing dilation. - Fitzpatrick's Dermatology, Fig. 148-15
When venous valves become incompetent, blood refluxes retrograde under the influence of gravity. This raises pressure in distal valves, causing a cascade of progressive incompetence. Blood flows in the opposite direction - from the deep system back into the superficial system through incompetent perforators. The superficial veins, unsupported by muscle or fascia, cannot withstand the elevated pressure and dilate, elongate, and become tortuous.
Venous pressure in these superficial veins can rise to up to 10 times normal in prolonged dependent posture. - Robbins & Cotran
Key Anatomical Sites of Valvular Incompetence
According to Gray's Anatomy for Students, the typical sites where incompetent valves cause marked varicosities are:
| Site | Structures Involved |
|---|---|
| Saphena varix | Saphenofemoral junction - GSV joining femoral vein |
| Midthigh perforator | GSV to femoral vein |
| Calf (Cockett's) perforators | 5, 10, 15 cm above medial malleolus - GSV to deep calf veins |
| Popliteal junction | SSV to popliteal vein |
The GSV system is affected in ~60% of cases; the SSV system in ~20%. - Bailey and Love's, p. 1052
Clinical Photo

Clinical appearance: extensive varicose veins on the calf and thigh. - Fitzpatrick's Dermatology
Classification
Primary varicose veins - result from intrinsic weakness of the venous wall (faulty collagen/smooth muscle development), with no prior deep vein thrombosis. Genetic predisposition is well recognised.
Secondary varicose veins - result from pre-existing deep or superficial venous insufficiency, most commonly following deep vein thrombosis (DVT). When thrombus incorporates the valve cusps and the clot is lysed by plasmin, the valve leaflets are destroyed, rendering them permanently incompetent. This is the post-phlebitic (post-thrombotic) syndrome.
CEAP classification places varicose veins at C2 (visible varicose veins ≥3 mm diameter).
Consequences of Anatomical Disruption
Once perforating vein valves fail, high-pressure deep venous blood refluxes into the unsupported superficial veins. The resulting chronically elevated venous pressure causes:
- Capillary hypertension - fluid and proteins leak into the interstitium - oedema
- Red cell extravasation - haemolysis produces haemosiderin - brown skin pigmentation
- Fibrin cuff formation - fibrinogen leaks around capillaries, potentially impairing tissue nutrition
- White cell trapping - leads to soft-tissue inflammation and fibrosis - lipodermatosclerosis
- Venous ulceration - particularly around the medial malleolus (the "gaiter area"), where perforators are most numerous and reflux pressure is highest
Notably, embolism from superficial varicose veins is very rare, in contrast to deep vein thrombosis. - Robbins & Cotran, p. 60
Surgical Anatomy Points
The saphenous nerve runs alongside the GSV in the lower leg and can be injured during stripping. In the popliteal fossa, the SSV junction with the popliteal vein is variable - it may enter higher than expected, and the common peroneal nerve and sural nerve lie in close proximity, explaining why nerve injury is a recognised complication of SPJ surgery.
Sources: Gray's Anatomy for Students (4th Ed.) | Bailey and Love's Short Practice of Surgery (28th Ed.) | Robbins, Cotran & Kumar Pathologic Basis of Disease | Schwartz's Principles of Surgery (11th Ed.) | Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.