Crush syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"crush syndrome" AND rhabdomyolysis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Crush Syndrome
Definition
Crush syndrome is the systemic manifestation of skeletal muscle cell damage resulting from prolonged pressure or crushing - with or without subsequent compartment syndrome. It is the body's systemic response to crushed muscle tissue, particularly when blood flow is restored to the area and toxic intracellular contents flood the circulation.
- Crush injury = the local mechanical damage (lacerations, fractures, degloving, bleeding)
- Crush syndrome = the downstream systemic toxidrome that follows
"Crush syndrome is the systemic manifestation of muscle cell damage resulting from pressure or crushing with or without subsequent compartment syndrome." - Tintinalli's Emergency Medicine, p. 75
History
First formally described in victims trapped during the London Blitz (WWII). The association between crush injury, rhabdomyolysis, and acute kidney injury (AKI) was established from these observations. It is now recognized in earthquake survivors, mining accident victims, and battlefield casualties.
Epidemiology
- Occurs in 3-20% of earthquake victims; up to 40% of survivors of multi-story building collapses
- Incidence of crush syndrome with subsequent renal failure ranges from 1-25% in various reports, depending on disaster type, rescue timing, and quality of early care
- Most common in the extremities (trunk/head-neck crush is usually quickly lethal)
- Associated injuries: fractures, lacerations, degloving injury
Pathophysiology
Step 1 - Muscle Cell Destruction
Prolonged compression + ischemia ruptures the sarcolemma, releasing intracellular contents:
| Released Substance | Consequence |
|---|---|
| Calcium ions | Activates proteolytic enzymes; generates oxygen free radicals → perpetuates myocyte destruction |
| Potassium | Hyperkalemia → arrhythmias, cardiac arrest |
| Phosphate | Precipitates in renal tubules, binds Ca²⁺ |
| Myoglobin | Direct and indirect nephrotoxicity |
| Creatine kinase (CK) | Marker of muscle damage |
| Uric acid | Precipitates in distal tubules at low pH |
| Thromboplastin | Can trigger DIC |
Serum haptoglobin binds some myoglobin, but its capacity is rapidly overwhelmed.
Step 2 - Reperfusion Injury
On extrication, restoration of blood flow causes reperfusion syndrome - a paradoxical worsening through:
- Oxidant production and complement activation
- Neutrophil and platelet interaction with endothelium
- Systemic inflammatory response
Systemic effects: hypotension, vasodilation, hypovolemia, myocardial depression, hyperkalemia, acidosis.
Step 3 - Fluid Third-Spacing & Hypovolemia
Membrane damage to myocytes AND systemic capillary endothelium causes massive fluid shift into the damaged tissues. An adult may require up to 12 L/day of fluids to maintain adequate circulation.
Step 4 - Renal Failure (Most Serious Complication)
Renal failure is multifactorial:
- Systemic hypoperfusion from hypovolemia
- Renal vasoconstriction (reflex + mediator-driven)
- Direct myoglobin nephrotoxicity: myoglobin forms ferriheme, which generates free hydroxyl radicals → lipid peroxidation → tubular damage
- Tubular obstruction by precipitation of myoglobin, uric acid, and phosphate (worsened by low urine pH)
Compartment Pressure Dynamics
Normal muscle compartment pressure: < 10 mmHg
- Pressures > 30 mmHg → muscle ischemia
- Irreversible nerve and muscle damage after 4-6 hours at these pressures
Clinical Features
"Appears Stable, Then Deteriorates"
Victims may appear stable while trapped, then rapidly deteriorate after extrication as toxins flood the systemic circulation.
Timeline
- Can develop within 1 hour in severe cases
- Typically takes 4-6 hours to manifest
- All patients trapped ≥ 4 hours should be treated as having crush injury
Compartment Syndrome: The 5 Ps
- Pain - diffuse, intense, out of proportion, worsened by passive stretch
- Paresthesias - numbness/tingling from nerve compression
- Passive stretch pain - hallmark of compartment syndrome
- Pressure - compartment feels tense and tight
- Pulselessness - late and unreliable sign (macrovasculature often spared)
Systemic Manifestations
- Hypovolemic shock (third-spacing + capillary leak)
- Hyperkalemia + hypocalcemia → arrhythmias, cardiac arrest
- Metabolic acidosis → worsens arrhythmogenicity
- Myoglobinuria - urine appears dark brown/"cola-colored"
- Acute kidney injury / renal failure
- ARDS, sepsis, ischemic organ injury, DIC (delayed causes of death)
Early vs. Late Death
| Timing | Causes |
|---|---|
| Early | Hypovolemia (third-spacing), dysrhythmias (hyperkalemia + acidosis) |
| Delayed | Renal failure, ARDS, sepsis, DIC, electrolyte disturbances |
Diagnosis
Laboratory Tests (every 2-4 hours)
- Serum CK - marker and monitoring tool (not perfectly predictive of AKI severity)
- Serum potassium - critical; fatal hyperkalemia can occur without renal failure
- Serum calcium, phosphorus
- ABG/pH - metabolic acidosis severity
- Serum creatinine - AKI monitoring
- Coagulation indices - DIC surveillance
- Urine myoglobin, pH, electrolytes
- Creatinine clearance calculations may be considered
Compartment Pressure Measurement
- Dedicated device (e.g., Stryker STIC) or saline-filled needle manometry
- Positive: pressure > 30 mmHg
- Delta pressure (diastolic BP - compartment pressure) < 30 mmHg is also an indication for fasciotomy
Treatment
1. Pre-Extrication (BEFORE releasing the patient)
"Treatment of crush syndrome should start before extrication." - Bailey & Love's Surgery, 28th Ed., p. 480
- Start IV fluids immediately - aggressive volume loading before, during, and after extrication is the single most important intervention
- Start cardiac monitoring (can be done in confined spaces)
- Begin hyperkalemia management: insulin + glucose, calcium, ion exchange resins, β-agonists
2. Fluid Resuscitation
- Two large-bore IV lines
- Fluid of choice: Normal saline (0.9% NaCl)
- AVOID Ringer's lactate and other potassium-containing fluids - can precipitate fatal hyperkalemia
- Initial bolus: 1-2 L, then:
- 1000 mL/h for first 2 hours → reduce to 500 mL/h
- Target urine output: 200-300 mL/h (~5-7 L/24 hours) in adults
- Bailey & Love recommends 1000-1500 mL/h saline initially in adults
- May require up to 12 L/day total
3. Forced Alkaline Diuresis
Once urine flow is established:
- Mannitol - osmotic diuretic; reduces reperfusion injury component, increases tubular flow
- Urine alkalinization - keep urinary pH > 6.5 to prevent myoglobin/uric acid precipitation
- Target: alkaline diuresis of up to 8 L/day
- Continue until myoglobin is no longer detectable in urine
4. Fasciotomy - Controversial Timing
Indications:
- Absent distal pulses
- Need for debridement of necrotic muscle
- Compartment pressure > 30 mmHg (measured within 6 hours)
- Delta pressure < 30 mmHg
Critical caveat on late fasciotomy:
"A late fasciotomy, when it is obvious that the muscles of that compartment must be dead, is only likely to cause a massive release of myoglobin, as well as potentially introducing infection into dead tissue. It is therefore best not to perform a fasciotomy in cases where entrapment has been for over 12 hours." - Bailey & Love, 28th Ed.
Post-earthquake data: most fasciotomies were done > 12 hours post-injury, with high infection rates, increased amputations, and poor outcomes. Routine fasciotomy for crush wounds is not recommended.
5. ICU Monitoring & Renal Support
- Catheterize for accurate urine output monitoring
- Serial labs every 2-4 hours
- Renal dialysis if AKI progresses
- Monitor fluid balance closely
6. Adjunct: Hyperbaric Oxygen Therapy
- Supplements oxygen to hypoxic tissues in early post-injury period
- At 2 atm: blood oxygen content increased by ~125% (via plasma oxygen)
- Also reduces edema through oxygen-induced vasoconstriction (reduces blood flow 10-20% while maintaining oxygen delivery)
- Useful adjunct for both crush injury and compartment syndrome
Summary of Key Points
| Feature | Detail |
|---|---|
| Mechanism | Rhabdomyolysis + reperfusion + systemic toxin release |
| Most serious complication | Acute kidney injury / renal failure |
| Key toxin | Myoglobin (ferriheme → hydroxyl radicals → tubular damage) |
| Most important early intervention | Aggressive IV fluids BEFORE extrication |
| Fluid of choice | Normal saline (avoid potassium-containing fluids) |
| Target urine output | 200-300 mL/h |
| Urine alkalinization target | pH > 6.5 |
| Early deaths | Hyperkalemia, metabolic acidosis → arrhythmias; hypovolemia |
| Delayed deaths | AKI, ARDS, DIC, sepsis |
| Fasciotomy timing | Early only; avoid after > 12 hours of entrapment |
Sources:
- [Tintinalli's Emergency Medicine, 9th Ed.](p. 75-76) - Pathophysiology, diagnosis, treatment
- [Rosen's Emergency Medicine, 9th Ed.](p. 3777) - Epidemiology, pre-extrication management
- [Bailey & Love's Surgery, 28th Ed.](p. 479-480) - Clinical management, fasciotomy guidance
- Recent reviews: Fernandez & Smith, J Am Acad Orthop Surg 2024 and Luo et al., Diagnostics 2023 confirm the above management principles remain current
Hyperkalemia management
Finding Sources
Finding Sources
Searching PubMed
"hyperkalemia" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, well-illustrated answer. Let me compile it.
Hyperkalemia Management
Definition & Severity Classification
| Severity | Serum K⁺ (mEq/L) |
|---|---|
| Mild | 5.5 - 6.0 |
| Moderate | 6.0 - 6.5 |
| Severe | > 6.5 |
Hyperkalemia with any ECG changes is a true medical emergency regardless of the absolute K⁺ level. Patients with K⁺ ≥ 6.5-7.0 mEq/L without ECG changes should still be aggressively managed.
First Step: ECG
A 12-lead ECG is the most important initial test. ECG changes follow a progressive sequence as K⁺ rises:
- Peaked (tall, narrow, symmetric) T waves - earliest change
- Prolonged PR interval
- Widened QRS complex
- Sine wave pattern (merging of QRS and T wave)
- Ventricular fibrillation / asystole
Treatment Framework
Treatment is organized into three sequential categories:
"The treatment of hyperkalemia is generally divided into three categories: (1) antagonism of the cardiac effects of hyperkalemia; (2) rapid reduction in K⁺ by redistribution into cells; and (3) removal of K⁺ from the body." - Brenner & Rector's The Kidney
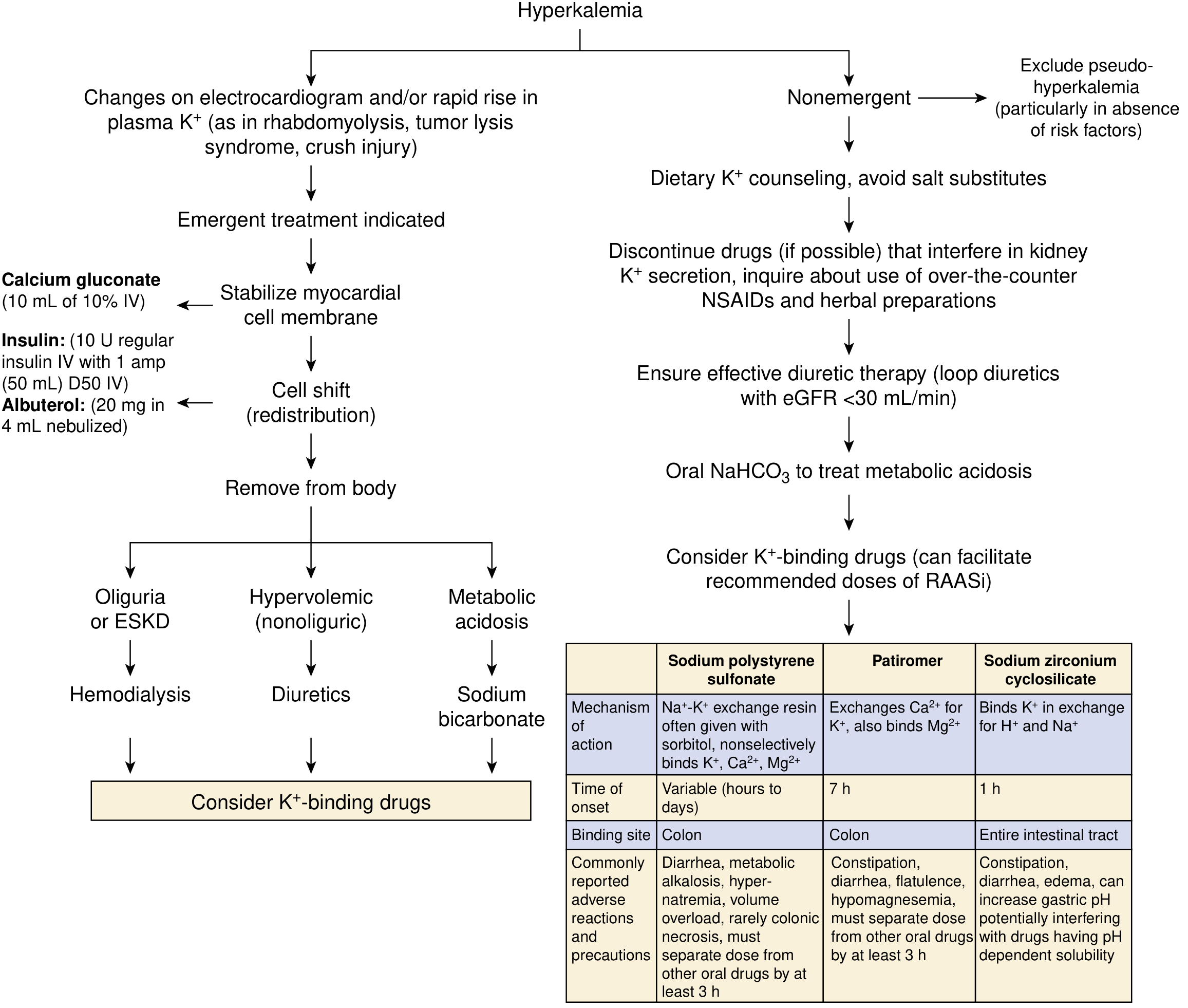
Step 1 - Stabilize the Myocardium (Membrane Antagonism)
Calcium (First-Line for ECG Changes)
Calcium raises the action potential threshold, restoring the normal 15-mV difference between resting and threshold potentials, thereby reducing myocyte excitability and restoring myocardial conduction. It does not lower the K⁺ level.
| Agent | Dose | Route | Notes |
|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 2-3 min | Peripheral line preferred | Less irritating to veins |
| Calcium chloride 10% | 3-4 mL IV over 2-3 min | Central line required | Higher elemental Ca²⁺; risk of tissue necrosis if extravasates |
- Onset: 1-3 minutes; Duration: 30-60 minutes
- Repeat if no ECG improvement or if changes recur
- CAUTION in digoxin toxicity: hypercalcemia potentiates digitalis cardiac toxicity - give 10 mL Ca gluconate diluted in 100 mL D5W over 20-30 minutes instead
- Never mix calcium with bicarbonate (precipitates calcium carbonate)
Step 2 - Redistribute K⁺ into Cells (Temporizing)
These measures shift K⁺ intracellularly but do not remove it from the body. They are temporary bridges to definitive therapy.
A. Insulin + Glucose (Most Reliable)
Shifts K⁺ into skeletal muscle and hepatocytes. Effect is reliable even in CKD/ESKD.
- Dose: 10 U regular insulin IV bolus + 50 mL of 50% dextrose (D50W, 1 ampule) IV
- Follow with continuous 5% dextrose at 100 mL/h to prevent late hypoglycemia
- Onset: within 15 minutes; peak effect ~60 min
- If blood glucose > 300 mg/dL (in diabetes): insulin can be given without concurrent dextrose
- Never give dextrose alone without insulin in patients with inadequate endogenous insulin - the resulting hyperglycemia can paradoxically raise K⁺
- Monitor blood glucose closely - hypoglycemia is common, especially in renal failure (prolonged insulin half-life)
B. Beta-2 Agonists (Additive to Insulin)
Stimulates Na⁺/K⁺-ATPase → shifts K⁺ into cells. Effect is additive to insulin.
- Dose: Albuterol (salbutamol) 20 mg nebulized over 10 minutes
- Note: This is far higher than the asthma dose - only a small fraction of nebulized albuterol is absorbed systemically
- IV albuterol 0.5 mg (available in Europe) produces equivalent effect
- Onset: ~30 minutes
- Some patients (~20-40%) are non-responders (particularly dialysis patients)
C. Sodium Bicarbonate (Controversial)
- Useful in patients with severe metabolic acidosis (HCO₃⁻ < 10 mmol/L)
- Lowers K⁺ by enhancing renal K⁺ excretion in patients with residual kidney function
- Not effective in anuric patients / ESKD - does not enhance effects of insulin or albuterol
- Use isotonic sodium bicarbonate
- Caution: can cause hypernatremia, volume overload, and reduce ionized calcium
Step 3 - Remove K⁺ from the Body (Definitive)
A. Diuretics (for patients with residual renal function)
- Loop diuretics (furosemide, torsemide, bumetanide) preferred
- In CKD: prefer torsemide (highest bioavailability, least renal metabolism) or furosemide (least hepatic metabolism for IV use)
- Combine loop + thiazide-like diuretics for greater efficacy (ceiling dose strategy)
- Ensure adequate Na⁺ delivery to distal tubule to augment K⁺ excretion (saline hydration)
- Not effective in oliguria or ESKD
B. Hemodialysis (Most Effective - for ESKD / Severe AKI)
- Most effective method to remove K⁺
- Can rarely be initiated quickly enough to preclude the emergency measures above
- Indicated when: anuric/oliguric ESKD, severe AKI, K⁺ unresponsive to other measures
C. Potassium Binders (Adjunct / Chronic Prevention)
Used after emergency stabilization; not for acute monotherapy. Key comparisons:
| Drug | Mechanism | Site | Onset | Dosing | Key Side Effects |
|---|---|---|---|---|---|
| Sodium polystyrene sulfonate (SPS, Kayexalate) | Na⁺-K⁺ resin exchange | Colon | Hours to days | 50 g PO in sorbitol or rectal enema | Colonic necrosis (rare, esp. with sorbitol), hypernatremia, volume overload |
| Patiromer (Veltassa) | Ca²⁺-K⁺ exchange | Colon | ~7 hours | 8.4 g once daily PO; titrate weekly | Constipation, hypomagnesemia; separate from other meds by 3 h |
| Sodium zirconium cyclosilicate (Lokelma) | K⁺/H⁺/Na⁺ exchanger (9× higher capacity than SPS) | Entire GI tract | ~1 hour | 10 g TID × 48 h, then 5 g daily maintenance | Edema (sodium load), constipation; may raise gastric pH (affects pH-dependent drug absorption) |
- Patiromer and SZC are not approved for emergency monotherapy but can be adjuncts
- A 2025 systematic review and network meta-analysis (Huang et al., Drugs) confirmed both novel binders (patiromer, SZC) effectively lower K⁺ by ~1 mEq/L and allow continuation of RAASi in CKD/heart failure
Non-Emergent / Chronic Management
For mild, non-emergent hyperkalemia without ECG changes:
- Exclude pseudohyperkalemia (hemolysis, thrombocytosis, prolonged tourniquet time)
- Dietary K⁺ restriction (~60 mEq/day); avoid salt substitutes (contain KCl)
- Discontinue offending drugs: ACE inhibitors, ARBs, K⁺-sparing diuretics (spironolactone, amiloride), NSAIDs, heparin, TMP-SMX
- Loop diuretics if adequate renal function
- Oral NaHCO₃ if metabolic acidosis present
- K⁺ binders (patiromer or SZC) to enable continued RAASi therapy in CKD/HF
Special Situations
Digoxin Toxicity
- If hyperkalemia is driven by digoxin, treat the digoxin toxicity first with anti-digoxin Fab fragments
- Give calcium slowly and with caution (hypercalcemia worsens digoxin toxicity)
Renal Failure / ESKD
- Bicarbonate less effective (no renal excretion)
- Insulin half-life prolonged → higher hypoglycemia risk; consider lispro/aspart (not renally metabolized)
- Dialysis is the cornerstone of definitive management
- Fludrocortisone (0.1-0.3 mg/day) may be considered in hypoaldosteronism but evidence for interdialytic hyperkalemia is modest
Mineralocorticoid Deficiency (Hypoaldosteronism)
- Fludrocortisone 0.1-0.3 mg/day is the treatment of choice
Summary: Rapid Action Table
| Step | Intervention | Onset | Duration | Mechanism | K⁺ Reduction |
|---|---|---|---|---|---|
| 1 | Calcium gluconate 10% 10 mL IV | 1-3 min | 30-60 min | Membrane stabilization | None (protects heart) |
| 2a | Insulin 10 U + D50 IV | 15 min | 4-6 h | Intracellular shift | ~0.5-1.5 mEq/L |
| 2b | Albuterol 20 mg nebulized | 30 min | 2-4 h | Intracellular shift (additive) | ~0.5-1.0 mEq/L |
| 2c | NaHCO₃ IV (if acidosis) | 30-60 min | Variable | Intracellular shift + renal excretion | ~0.5 mEq/L |
| 3a | Loop diuretics IV | 30-60 min | Ongoing | Renal excretion | Variable |
| 3b | Hemodialysis | 1-2 h (setup) | Ongoing | Removal from body | Most effective |
| 3c | K⁺ binders (adjunct) | Hours | Ongoing | GI removal | ~0.5-1.0 mEq/L |
Sources:
- [Brenner & Rector's The Kidney](p. 774-780) - Detailed mechanisms and dosing
- [NKF Primer on Kidney Diseases, 8e](p. 128-129) - Practical clinical approach
- Huang et al., Drugs 2025 - PMID 40542996 - Novel K⁺ binders meta-analysis (recent evidence)
Hyponatremia
Finding Sources
Finding Sources
Searching PubMed
"hyponatremia" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Hyponatremia
Definition & Severity
Hyponatremia = serum Na⁺ < 135 mEq/L. It is the most common electrolyte disorder in hospitalized patients.
| Severity | Serum Na⁺ (mEq/L) |
|---|---|
| Mild | 130 - 134 |
| Moderate | 125 - 129 |
| Severe / Profound | < 125 |
Step 1: Classify by Plasma Osmolality
The first step is always to measure plasma osmolality to distinguish true hyponatremia from pseudohyponatremia.
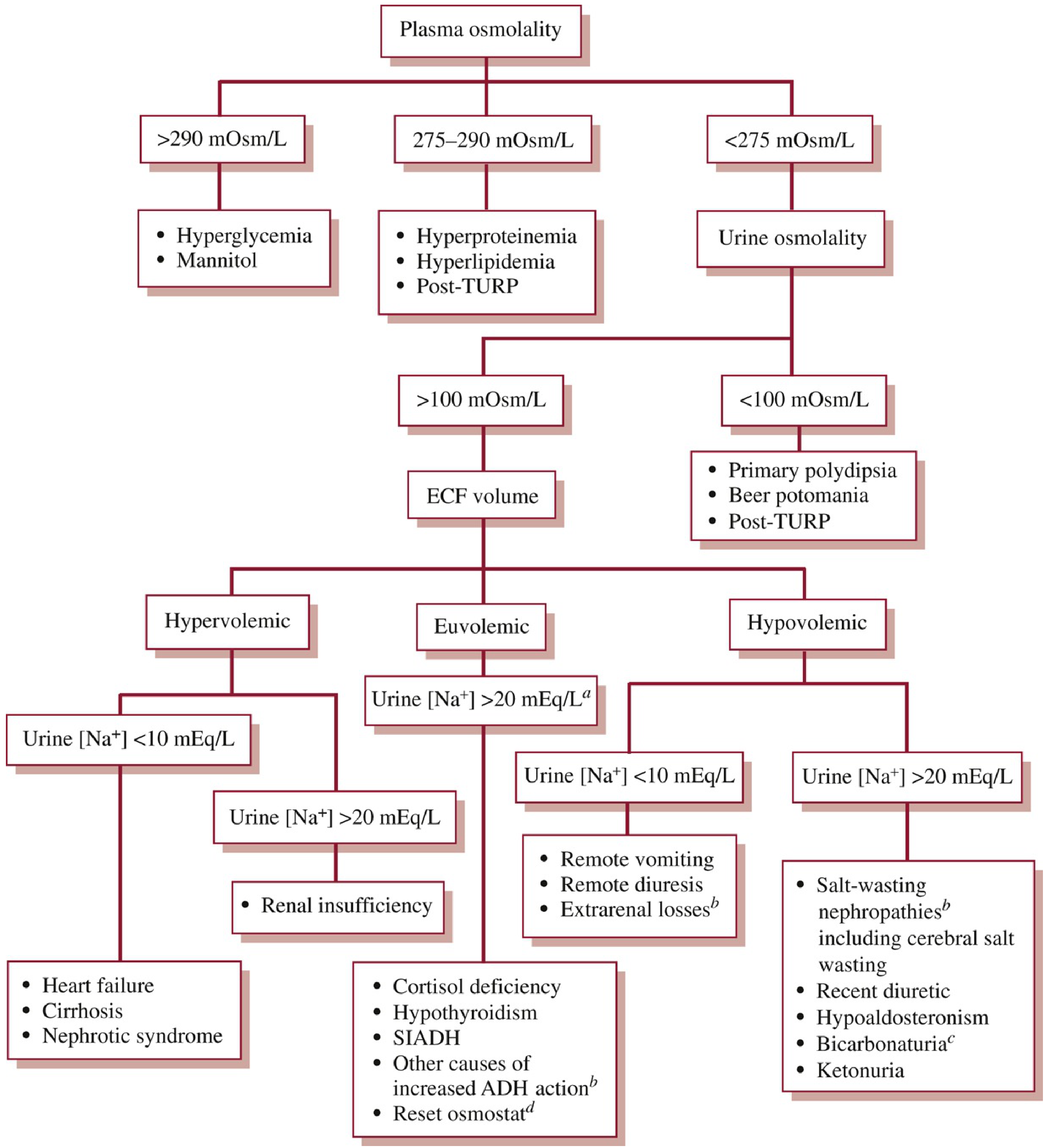
| Plasma Osm | Interpretation | Causes |
|---|---|---|
| > 290 mOsm/L (Hyperosmolar) | Osmotically active solutes displacing Na⁺ | Hyperglycemia (most common), mannitol |
| 275-290 mOsm/L (Iso-osmolar) | Pseudohyponatremia | Hyperproteinemia, hyperlipidemia, post-TURP |
| < 275 mOsm/L (Hypo-osmolar) | True hyponatremia | → proceed to urine osmolality |
Step 2: Urine Osmolality (for true hypo-osmolar hyponatremia)
| Urine Osm | Interpretation |
|---|---|
| < 100 mOsm/L | ADH suppressed; kidneys diluting normally but overwhelmed |
| > 100 mOsm/L | ADH present/active - impaired water excretion |
Step 3: ECF Volume Status + Urine Na⁺
Hypovolemic Hyponatremia (↓ ECF volume)
| Urine Na⁺ | Cause |
|---|---|
| < 10 mEq/L (extrarenal losses) | Vomiting, diarrhea, burns, third-spacing |
| > 20 mEq/L (renal losses) | Diuretics (thiazides > loop), salt-wasting nephropathies, cerebral salt wasting, hypoaldosteronism, ketonuria |
Euvolemic Hyponatremia (normal ECF volume, urine Na⁺ > 20 mEq/L)
Most common causes:
- SIADH (most common euvolemic cause)
- Hypothyroidism
- Cortisol/glucocorticoid deficiency (Addison's disease)
- Reset osmostat
Hypervolemic Hyponatremia (↑ ECF volume, edematous states)
| Urine Na⁺ | Cause |
|---|---|
| < 10 mEq/L | Heart failure, cirrhosis, nephrotic syndrome |
| > 20 mEq/L | Renal insufficiency/AKI |
Clinical Features
Acute Hyponatremia (< 24-48 hours)
Rapid fall in Na⁺ → cerebral edema before brain adaptation can occur:
- Headache, nausea, vomiting
- Confusion, disorientation
- Seizures, respiratory arrest
- Brain herniation (most feared - almost exclusively acute)
- Noncardiogenic pulmonary edema can exacerbate brain swelling via hypoxia
Chronic Hyponatremia (> 48 hours)
Brain extrudes solutes (brain volume regulation) → less acute edema:
- Often labelled "asymptomatic" but subtle deficits are common
- Headache, nausea, mood disturbances
- Cognitive slowing, difficulty concentrating
- Gait instability, falls (markedly increased fracture risk)
- Increased osteoporosis and bone fractures in older patients
- Seizures (can still occur)
"Many such patients very often do have neurologic symptoms, even if milder and more subtle in nature... The major clinical significance of chronic hyponatremia may lie in the increased morbidity and mortality associated with falls and fractures in older populations." - NKF Primer on Kidney Diseases, 8e
High-risk groups for severe neurologic outcomes: menstruating women, young children, postoperative patients, those with underlying epilepsy.
Treatment
The Cardinal Rule: Rate of Correction
This is the most important concept in hyponatremia management.
| Scenario | Target Correction |
|---|---|
| Symptomatic (acute/severe) | Raise Na⁺ by 4-6 mEq/L in first 4-6 hours to control symptoms |
| Chronic hyponatremia | Do NOT exceed 8 mEq/L in 24 hours (or 18 mEq/L in 48 hours) |
Osmotic Demyelination Syndrome (ODS) / Central Pontine Myelinolysis (CPM)
- Caused by overly rapid correction of chronic hyponatremia
- Risk threshold: correction > 10-12 mEq/L in 24 hours
- Clinical features: flaccid paralysis (locked-in syndrome), dysarthria, dysphagia
- Diagnosis: CT/MRI of brain (demyelination in pons)
- Risk factors: hypokalemia, malnutrition, alcohol use disorder, chronic liver disease
- In acute hyponatremia (< 24-48 h): rapid correction is safe and needed - ODS risk is from correcting chronic hyponatremia too fast
Treatment by Type
1. Symptomatic / Severe Hyponatremia (neurologic symptoms, seizures, herniation)
Hypertonic 3% Saline - most reliable method to rapidly raise Na⁺
- Bolus method (preferred for emergencies): 100 mL of 3% NaCl IV bolus; repeat once after 30 min if no improvement
- Raises serum Na⁺ by ~2-4 mEq/L per bolus
- Sufficient to reduce brain swelling and lower intracranial pressure in acute hyponatremia
- Continuous infusion (stable severe hyponatremia): 0.25-0.3 mL/kg/h as a safer starting rate (titrate based on labs)
- Simple formula to estimate infusion rate:
Patient's weight (kg) × desired correction rate (mEq/L/h) = infusion rate of 3% NaCl (mL/h)
- CRITICAL: No equation reliably predicts dynamic water balance; recheck serum Na⁺ frequently (every 2-4 hours) and adjust
- Can be given peripherally (low rate of minor complications); central line not always required
- DDAVP can be given prophylactically to clamp aquaporins and prevent overcorrection, especially in patients with a reversible ADH cause (e.g., pain, hypovolemia) where Na⁺ may correct too rapidly once the stimulus resolves
2. Hypovolemic Hyponatremia (asymptomatic)
Isotonic (0.9%) saline - restores ECF volume → removes nonosmotic stimulus for ADH → aquaresis follows
- Supplement with K⁺ (30-40 mmol/L) if diuretic-induced, even if serum K⁺ is not low
- Avoid isotonic saline in SIADH - it will worsen hyponatremia in euvolemic patients by providing a Na⁺ load that is excreted while free water is retained
3. SIADH - Euvolemic Hyponatremia
First-line: Fluid restriction
- Restrict to 500-1000 mL/24 hours
- Guide degree of restriction using the electrolyte-to-Na⁺ ratio formula:
| Urine (Na⁺+K⁺) / Serum Na⁺ | Fluid restriction |
|---|---|
| < 0.5 | Restrict to 1 L/day |
| 0.5-1.0 | Restrict to 500 mL/day |
| > 1.0 | Adjunctive therapy required (any fluid intake will be retained) |
Second-line options for SIADH:
- Loop diuretics - impair urine concentrating ability, enhance free water excretion
- Salt tablets / oral urea - increase solute excretion; each gram of urea excreted obligates water co-excretion
- Vasopressin receptor antagonists (Vaptans):
- Conivaptan (IV, V1a/V2 antagonist) - inpatient only
- Tolvaptan (oral, selective V2 antagonist) - inpatient and outpatient
- Mechanism: block ADH at V2 receptors in collecting duct → aquaresis (free water excretion without significant Na⁺ or K⁺ loss)
- Approved for euvolemic and hypervolemic hyponatremia (SIADH, heart failure, cirrhosis - though EMA restricts tolvaptan to SIADH only)
- Contraindicated in hypovolemic hyponatremia (can worsen hypotension)
- Tolvaptan FDA warning: potential for irreversible/fatal liver injury (based on TEMPO ADPKD trial at higher doses); limit to ≤ 30 days; avoid in underlying liver disease/cirrhosis
- Ineffective if serum creatinine > 3.0 mg/dL
- Risk: overly rapid Na⁺ correction - requires close monitoring; start only in hospital
- Generic tolvaptan available since 2020 (cost barrier reduced)
Other agents (limited role):
- Demeclocycline - works too slowly; nephrotoxic; not recommended for acute management
- Fludrocortisone/mineralocorticoids - adjunct in specific salt-wasting conditions
4. Hypervolemic Hyponatremia (CHF, cirrhosis, nephrotic syndrome)
- Definitive treatment: manage the underlying condition
- Fluid restriction to attenuate hyponatremia
- Loop diuretics (furosemide) to remove free water and Na⁺ together
- Vaptans (conivaptan/tolvaptan): approved but tolvaptan now restricted in cirrhosis (FDA warning); EMA does not approve for HF or cirrhosis
- Avoid isotonic saline (worsens volume overload)
- A 2025 AGA Clinical Practice Update (Orman et al., Gastroenterology) addresses hyponatremia specifically in cirrhosis
SIADH Diagnosis (Criteria)
Classic criteria for SIADH:
- Hypo-osmolality (serum osm < 275 mOsm/L)
- Urine osmolality > 100 mOsm/L (inappropriately concentrated for the hypo-osmolar state)
- Urine Na⁺ > 20 mEq/L (on normal salt intake)
- Euvolemia (no hypovolemia, no edema)
- Normal thyroid and adrenal function
- Not on diuretics
Common causes of SIADH: CNS disorders (meningitis, stroke, SAH), pulmonary disease (pneumonia, TB), malignancy (small cell lung cancer), drugs (SSRIs, carbamazepine, vincristine, cyclophosphamide, NSAIDs, oxytocin, MDMA/ecstasy), surgery/pain
Treatment Summary Table
| Type | Na⁺ | Volume | Primary Treatment |
|---|---|---|---|
| Acute symptomatic | Any | Any | 3% NaCl bolus (100 mL IV), ICU monitoring |
| Hypovolemic | Low | Low | 0.9% NaCl ± K⁺ supplementation |
| SIADH (euvolemic) | Low | Normal | Fluid restriction → loop diuretics/salt tablets → vaptans |
| Hypervolemic (CHF/cirrhosis) | Low | High | Fluid restriction + loop diuretics + treat underlying cause |
| Pseudohyponatremia | Low | Normal | Treat underlying (hyperglycemia, hypertriglyceridemia) |
Key Safety Rules
- Never correct chronic hyponatremia faster than 8 mEq/L/24 h - risk of osmotic demyelination
- Never use isotonic saline for SIADH - will worsen hyponatremia
- Never use hypertonic saline for hypovolemic hyponatremia as primary therapy - isotonic saline corrects the ADH stimulus
- Monitor Na⁺ every 2-4 hours when using 3% NaCl - no formula fully predicts water balance
- DDAVP as rescue if correction is going too fast - clamps the aquaresis
A 2025 JAMA Internal Medicine meta-analysis (Ayus et al., PMID 39556338) on correction rates in severe hyponatremia confirmed that both under- and over-correction are associated with increased mortality, reinforcing the importance of the 8 mEq/L/24h ceiling and frequent Na⁺ monitoring.
Sources:
- [Brenner & Rector's The Kidney](p. 674-677) - Pathophysiology, hypertonic saline, vaptans
- [NKF Primer on Kidney Diseases, 8e](p. 127-129) - Clinical algorithm, rates of correction, CPM
- [Washington Manual of Medical Therapeutics](p. 446-448) - Diagnostic algorithm and fluid restriction formula
- Ayus et al., JAMA Intern Med 2025 - PMID 39556338 - Meta-analysis on correction rates and outcomes
This is a shared conversation. Sign in to Orris to start your own chat.