Make notes of jaundice for mbbs 1st year for university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, exam-ready notes.
🟡 JAUNDICE — Complete MBBS 1st Year Notes
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed, Ganong's Review of Medical Physiology 26th ed, Harrison's Principles of Internal Medicine 22E, Schwartz's Principles of Surgery 11th ed
1. DEFINITION
Jaundice (= icterus) is the yellow discoloration of skin, sclera, and mucous membranes due to accumulation of bilirubin in tissues.
- Clinically detectable when serum bilirubin > 2 mg/dL (34 μmol/L)
- Normal serum bilirubin: 0.2–1.0 mg/dL
- Scleral icterus appears earliest (sclera has high affinity for bilirubin due to elastin content)
2. BILIRUBIN METABOLISM (Normal)
Understanding this is the key to understanding all types of jaundice.
Step-by-step:
| Step | Location | Process |
|---|---|---|
| 1. Formation | Macrophages of MPS (spleen, liver, bone marrow) | Heme → Biliverdin (via heme oxygenase, needs NADPH + O₂) → Bilirubin (via biliverdin reductase). CO and Fe²⁺ also released. |
| 2. Transport | Blood | Unconjugated bilirubin (UCB) is insoluble in water → binds albumin for transport. NOT filtered by kidney. |
| 3. Hepatic Uptake | Hepatocyte surface | Bilirubin dissociates from albumin; enters hepatocyte via facilitated diffusion; binds intracellular protein ligandin (Y protein). |
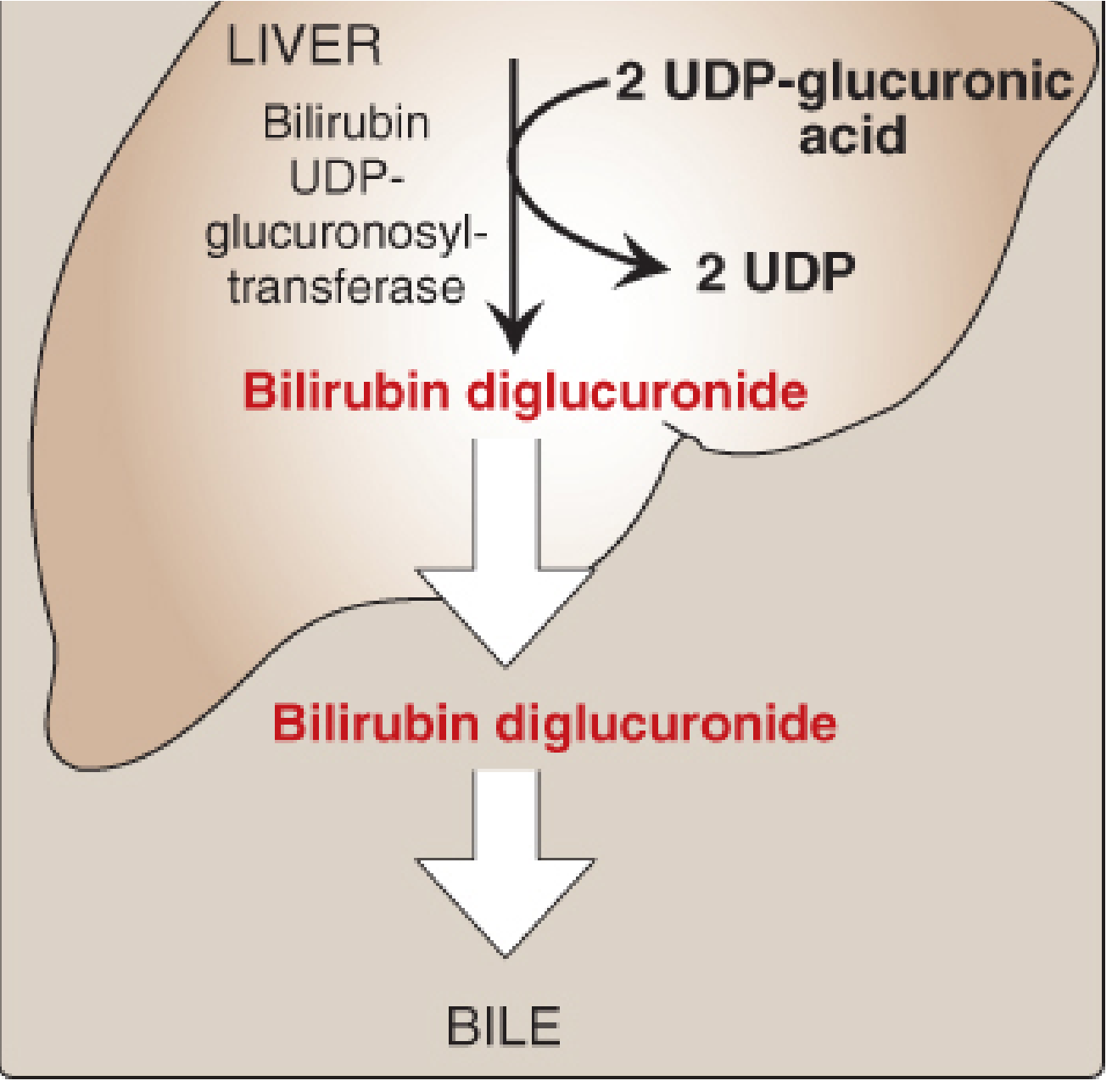
| 4. Conjugation | Hepatocyte ER | Bilirubin + 2× UDP-glucuronic acid → Bilirubin diglucuronide (conjugated bilirubin, CB). Enzyme: bilirubin UDP-glucuronosyltransferase (UGT). Now water-soluble. |
| 5. Excretion | Bile canaliculi | CB actively transported into bile against concentration gradient. Rate-limiting step. |
| 6. Intestinal fate | Gut (terminal ileum & colon) | CB reduced by gut bacteria → Urobilinogen → partly reabsorbed (enterohepatic circulation) → excreted in urine as urobilin (yellow) OR oxidized in colon → Stercobilin (gives stool its brown color). |
Key distinction:
- Unconjugated (indirect) bilirubin = water insoluble, albumin-bound, NOT in urine, van den Bergh reaction indirect
- Conjugated (direct) bilirubin = water soluble, NOT albumin-bound, appears in urine if elevated, van den Bergh reaction direct
3. CLASSIFICATION OF JAUNDICE
Type 1: Pre-hepatic (Hemolytic) Jaundice
Cause: Excessive RBC breakdown → bilirubin produced faster than liver can conjugate it.
Examples:
- Hereditary spherocytosis, sickle cell anemia, thalassemia
- G6PD deficiency
- Malaria, immune hemolysis
- Massive blood transfusion / resorption of hematoma
Mechanism: Excess heme → excess UCB → overwhelms hepatic conjugation capacity
Lab findings:
| Parameter | Result |
|---|---|
| Serum UCB (indirect) | ↑↑ |
| Serum CB (direct) | Normal |
| Urine bilirubin | Absent (UCB not filtered) |
| Urine urobilinogen | ↑↑ |
| Stool color | Normal/dark (↑ stercobilin) |
| ALT/AST | Normal |
| Serum bilirubin | Usually < 5 mg/dL |
Type 2: Hepatic (Hepatocellular) Jaundice
Cause: Damage to liver cells → impaired uptake, conjugation, AND/OR secretion.
Examples:
- Viral hepatitis (Hepatitis A, B, C, E)
- Cirrhosis, alcoholic liver disease
- Drug-induced liver injury (paracetamol overdose)
- Leptospirosis, yellow fever
Mechanism: Damaged hepatocytes → ↓ conjugation → UCB rises; if bile canaliculi damaged → CB regurgitates back into blood → both UCB & CB elevated.
Lab findings:
| Parameter | Result |
|---|---|
| Serum UCB | ↑ |
| Serum CB | ↑ (if intrahepatic cholestasis component) |
| Urine bilirubin | Present (CB leaks into blood → filtered) |
| Urine urobilinogen | ↑↑ (damaged liver can't recirculate urobilinogen absorbed from gut) |
| Stool color | Pale (↓ CB reaching gut) |
| ALT/AST | ↑↑ (hallmark) |
| Alkaline phosphatase | Mildly ↑ |
| Prothrombin time | ↑ (impaired clotting factor synthesis) |
Type 3: Post-hepatic (Obstructive/Cholestatic) Jaundice
Cause: Obstruction of bile flow (intrahepatic or extrahepatic) → CB cannot reach intestine → regurgitates into blood.
Extrahepatic obstruction examples:
- Choledocholithiasis (common bile duct stones)
- Carcinoma head of pancreas (most common cause of painless obstructive jaundice)
- Cholangiocarcinoma
- Strictures, worms (Ascaris), CBD compression
Intrahepatic cholestasis examples:
- Primary biliary cholangitis, Primary sclerosing cholangitis
- Drug-induced (chlorpromazine, estrogens)
Mechanism: Obstruction → bile cannot flow → CB accumulates in hepatocytes → regurgitates into sinusoids → enters blood.
Lab findings:
| Parameter | Result |
|---|---|
| Serum UCB | Normal |
| Serum CB (direct) | ↑↑ (hallmark) |
| Urine bilirubin | ↑↑ ("dark/cola-colored urine") |
| Urine urobilinogen | Absent (no CB reaches gut, no urobilinogen formed) |
| Stool color | Pale/clay-colored (no stercobilin) |
| ALT/AST | Mildly ↑ or normal |
| ALP + GGT | ↑↑↑ (hallmark of obstruction) |
| Serum cholesterol | ↑ |
| Pruritus | Common (bile salts deposit in skin) |
4. COMPARATIVE TABLE: THE 3 TYPES
| Feature | Pre-hepatic | Hepatic | Post-hepatic |
|---|---|---|---|
| UCB (indirect) | ↑↑ | ↑ | Normal |
| CB (direct) | Normal | ↑ | ↑↑ |
| Urine bilirubin | Absent | Present | Present (↑↑) |
| Urine urobilinogen | ↑↑ | ↑↑ | Absent |
| Stool color | Normal/dark | Pale | Pale/clay |
| ALT/AST | Normal | ↑↑ | Normal/mildly ↑ |
| ALP | Normal | Mildly ↑ | ↑↑↑ |
| Pruritus | Absent | Variable | Present |
| Van den Bergh reaction | Indirect +ve | Both +ve | Direct +ve |
5. GENETIC / INHERITED SYNDROMES (High-Yield for Exams)
Unconjugated hyperbilirubinemia:
| Syndrome | Defect | Bilirubin | Severity |
|---|---|---|---|
| Gilbert's syndrome | ↓ UGT activity (10–35% normal); ↓ hepatic uptake | Mild ↑ UCB (< 3 mg/dL) | Benign; triggered by fasting/stress |
| Crigler-Najjar type I | Complete absence of UGT | Severe ↑ UCB (> 20 mg/dL) | Fatal without liver transplant; kernicterus |
| Crigler-Najjar type II | UGT activity ≤ 10% | UCB 6–25 mg/dL | Responds to phenobarbital |
Conjugated hyperbilirubinemia:
| Syndrome | Defect | Feature |
|---|---|---|
| Dubin-Johnson syndrome | Defective MRP2 transporter (CB cannot exit hepatocyte) | Black liver (melanin-like pigment); benign |
| Rotor syndrome | Defective hepatic storage of CB | Similar to Dubin-Johnson but no black liver |
6. NEONATAL JAUNDICE (Physiological)
- Appears 2nd–3rd day of life, resolves by 10th day in term infants
- Premature infants: may persist up to 2 weeks
- Cause: Immature UGT enzyme (only ~1% activity at birth) + high rate of RBC breakdown + short RBC lifespan in neonates
- Serum bilirubin peaks at 5–6 mg/dL in term, higher in premature
- Pathological if: appears within 24 hrs of birth, bilirubin > 20 mg/dL, or persists beyond 2 weeks
- Kernicterus: UCB crosses blood–brain barrier → neurological damage (especially basal ganglia)
- Treatment: Phototherapy (converts bilirubin to water-soluble isomers excreted in urine/bile)
Note: Salicylates and sulfonamides displace bilirubin from albumin → increase risk of kernicterus in neonates — avoid these drugs in newborns.
7. DIAGNOSTIC APPROACH (Flowchart)
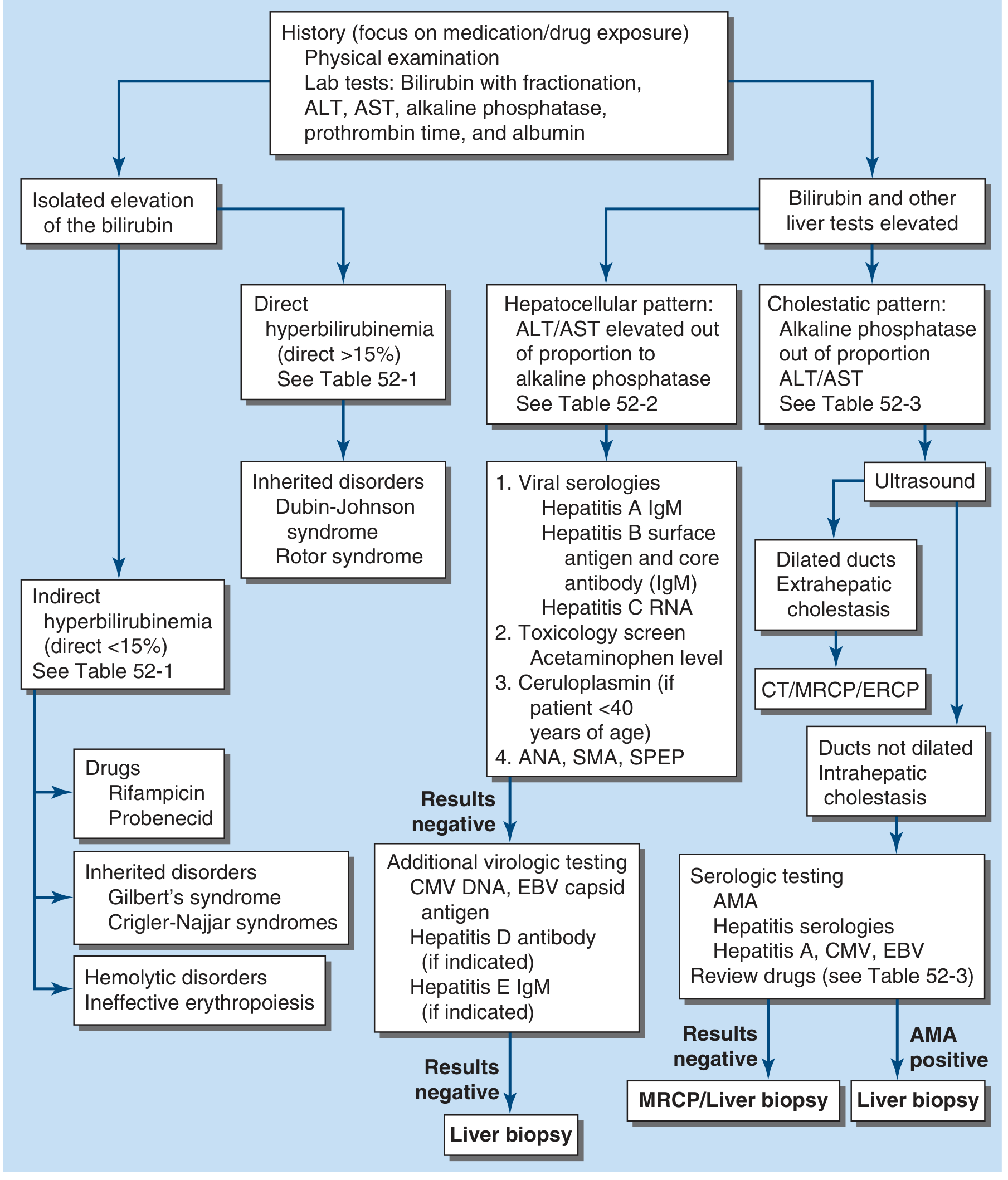
Step 1: History + Physical Examination
Step 2: LFTs — Bilirubin with fractionation (direct vs indirect), ALT, AST, ALP, GGT, albumin, PT
Step 3: Determine pattern:
- Isolated bilirubin elevation → check if direct or indirect → see inherited disorders
- Hepatocellular pattern (ALT/AST >> ALP) → viral serologies, autoimmune markers
- Cholestatic pattern (ALP >> ALT/AST) → Ultrasound → dilated ducts = extrahepatic (→ CT/MRCP/ERCP) vs non-dilated = intrahepatic
8. CLINICAL FEATURES
| Feature | Details |
|---|---|
| Scleral icterus | Earliest sign |
| Skin yellowing | Most visible in natural light |
| Dark urine | Conjugated bilirubin excreted by kidney |
| Pale stools | Absent stercobilin in obstructive jaundice |
| Pruritus | Due to bile salt deposits in skin (obstructive) |
| Hepatomegaly/splenomegaly | Depending on cause |
| Features of liver failure | Spider angiomata, palmar erythema, caput medusae, ascites, encephalopathy |
9. INVESTIGATIONS SUMMARY
| Test | Purpose |
|---|---|
| Total & direct bilirubin | Quantify and classify |
| ALT, AST | Hepatocellular damage |
| ALP, GGT | Cholestatic disease |
| Serum albumin, PT/INR | Hepatic synthetic function |
| CBC | Hemolysis (↓ Hb, ↑ reticulocytes, ↑ LDH) |
| Peripheral smear | Sickle cells, spherocytes |
| Viral markers | Hepatitis A IgM, HBsAg, HCV RNA, HEV IgM |
| Urine bilirubin & urobilinogen | Dipstick — quick bedside test |
| Ultrasound abdomen | First imaging for obstructive workup |
| MRCP/ERCP | Biliary tree visualization |
| Liver biopsy | Gold standard for intrahepatic cause |
10. KEY POINTS TO REMEMBER
- UCB = insoluble, albumin-bound, no urine bilirubin, indirect van den Bergh
- CB = water-soluble, appears in urine, direct van den Bergh
- Conjugation = bilirubin + 2 UDP-glucuronic acid → catalyzed by UGT in liver ER
- ALP is the most sensitive marker of biliary obstruction
- Absence of urobilinogen in urine = complete biliary obstruction
- Dark urine + pale stool + pruritus = classic triad of obstructive jaundice
- Gilbert's syndrome is the most common inherited jaundice (benign, autosomal recessive)
- Phenobarbital induces UGT → useful in Crigler-Najjar type II and neonatal jaundice
- Kernicterus risk in neonates when UCB > 20 mg/dL
— Lippincott Illustrated Reviews: Biochemistry 8th ed, pp. 796–804 | Ganong's Review of Medical Physiology 26th ed, p. 513 | Harrison's Principles of Internal Medicine 22E, pp. 365–366
This is a shared conversation. Sign in to Orris to start your own chat.