Cerebellum anatomy, function, diseases, and test
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
cerebellum anatomy lobes zones deep nuclei
Searching Images
cerebellar cortex layers Purkinje cells mossy climbing fibers
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information to produce a thorough answer. Here is the full breakdown:
The Cerebellum: Anatomy, Function, Diseases, and Clinical Testing
1. Anatomy
Gross Structure
The cerebellum sits dorsal to the pons and medulla, attached to the brainstem by three pairs of cerebellar peduncles, and is covered by the tentorium cerebelli. It constitutes ~10% of total brain volume but contains more than half of all brain neurons. Its surface area is approximately 75% that of the cerebral cortex due to dense foliation. — Ganong's Review of Medical Physiology, 26th Ed.
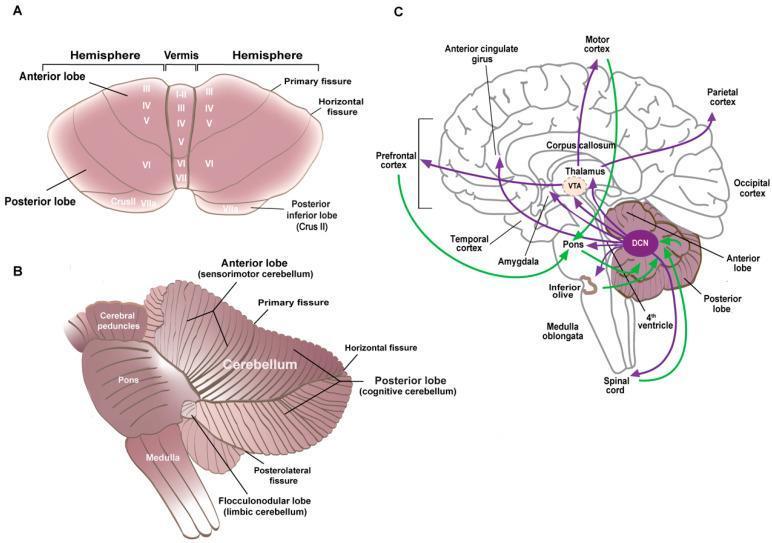
Lobes (Transverse Divisions)
Two transverse fissures divide the cerebellum into three lobes:
| Lobe | Key Structures | Functional Name |
|---|---|---|
| Anterior lobe (lobules I–V) | Vermis + hemisphere | Sensorimotor cerebellum (spinocerebellum) |
| Posterior lobe (lobules VI–IX) | Lateral hemispheres | Cognitive cerebellum (cerebrocerebellum) |
| Flocculonodular lobe (lobule X) | Flocculus + nodulus | Limbic/vestibulo cerebellum |
The primary fissure separates the anterior and posterior lobes; the posterolateral fissure separates the flocculonodular lobe from the rest. — Ganong's Review of Medical Physiology, 26th Ed.
Mediolateral Zones (Functional Longitudinal Zones)
| Zone | Controls | Deep Nucleus |
|---|---|---|
| Vermis (midline) | Axial/trunk muscles, gait | Fastigial nucleus |
| Intermediate hemisphere (paravermal) | Distal limb muscles, limb coordination | Interposed nucleus (globose + emboliform) |
| Lateral hemisphere | Motor planning, cognition, timing | Dentate nucleus |
Cerebellar Peduncles
- Superior cerebellar peduncle (SCP): mainly efferent — deep cerebellar nuclei → thalamus (VA/VL), red nucleus, brainstem
- Middle cerebellar peduncle (MCP): exclusively afferent — from contralateral pontine nuclei (corticopontocerebellar path)
- Inferior cerebellar peduncle (ICP): mixed — afferent from spinal cord and brainstem (spinocerebellar, olivocerebellar); efferent to vestibular nuclei
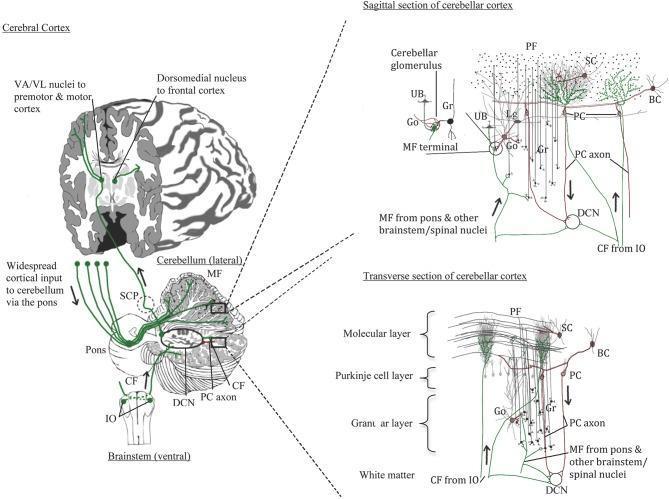
2. Microarchitecture: The Cerebellar Cortex
The cortex has three layers and five neuron types:
| Layer | Key Neurons |
|---|---|
| Molecular layer (outer) | Stellate cells, basket cells, parallel fibers (granule cell axon bifurcations) |
| Purkinje cell layer | Purkinje cells (the sole output of the cerebellar cortex) |
| Granular layer (inner) | Granule cells, Golgi cells, Lugaro cells, unipolar brush cells |
Key Cell Types & Their Roles
- Purkinje cells: Large, flask-shaped neurons with flat, fan-like dendrites perpendicular to parallel fibers. Their axons project inhibitory (GABAergic) signals to the deep cerebellar nuclei and vestibular nuclei — this is the only output of the cortex.
- Granule cells: The most numerous neurons in the CNS. Receive excitatory mossy fiber input; their axons ascend to the molecular layer and bifurcate into parallel fibers that run for long distances and form excitatory synapses on thousands of Purkinje cells.
- Basket & stellate cells: Inhibitory interneurons in the molecular layer.
- Golgi cells: Inhibitory feedback onto granule cells.
Two Afferent Systems
| Input | Source | Terminates on |
|---|---|---|
| Mossy fibers | Spinal cord, pontine nuclei, vestibular organs, reticular formation | Granule cells (via cerebellar glomeruli) → Purkinje cells via parallel fibers |
| Climbing fibers | Inferior olivary nucleus (contralateral) | Directly on Purkinje cell dendrites (1:1 relationship, powerful drive) |
Both systems send collaterals to the deep nuclei before reaching the cortex. The deep nuclei (dentate, interposed, fastigial) provide the primary output pathway of the cerebellum via the SCP.
3. Functions
The cerebellum acts as a comparator and error-correction machine for movement and timing. It does not initiate movement but modulates it through feedforward and feedback control. Key functions:
Motor Functions
- Coordination of movement — smooths out voluntary movements by integrating motor commands and sensory feedback
- Feedforward (predictive) control — acts before sensory feedback arrives, using internal models of the body to anticipate consequences of movement
- Timing control — critical for the precise temporal sequencing of muscle contractions
- Maintenance of posture and balance — especially via vestibulocerebellum (flocculonodular lobe)
- Coordination of eye and head movements — via connections with vestibular nuclei and gaze centers
- Motor learning — climbing fiber activity from the inferior olive modifies parallel fiber → Purkinje cell synaptic strength (long-term depression, LTD); the Marr-Albus-Ito theory proposes this as the cellular basis of motor learning
Cognitive and Non-Motor Functions
The lateral hemispheres connect extensively with prefrontal, parietal, and temporal cortex via the pons and thalamus. Damage to these regions can produce Cerebellar Cognitive Affective Syndrome (CCAS, Schmahmann Syndrome): impaired executive function, spatial cognition, linguistic deficits, and personality change (blunting of affect or disinhibition). — Bradley and Daroff's Neurology in Clinical Practice
4. Diseases of the Cerebellum
Clinical Signs by Lesion Location
| Region Damaged | Primary Signs |
|---|---|
| Vermis / fastigial nucleus | Truncal ataxia, wide-based gait, scanning dysarthria, titubation (head tremor) |
| Flocculonodular lobe | Severe disequilibrium, multidirectional body sway, nystagmus, vertigo |
| Hemispheres / dentate | Ipsilateral limb ataxia (appendicular), intention tremor, dysmetria, dysdiadochokinesis |
Key principle: cerebellar lesions cause ipsilateral deficits (the cerebellum → SCP → crosses → thalamus → ipsilateral cortex → crosses again in corticospinal tract → net ipsilateral effect).
Cardinal Signs of Cerebellar Dysfunction
| Sign | Description |
|---|---|
| Ataxia | General incoordination — jerky, irregular, highly variable movements |
| Dysmetria | Over- or undershooting of intended targets (past-pointing) |
| Intention tremor | Oscillation that worsens as the limb approaches a target |
| Dysdiadochokinesis | Inability to perform rapid alternating movements (e.g., pronation/supination) |
| Decomposition of movement | Breaking a multi-joint movement into sequential single-joint movements |
| Dysarthria | Slurred, scanning, irregular speech; syllables broken apart |
| Nystagmus | Gaze-evoked, horizontal nystagmus; slow phase toward lesion |
| Hypotonia | Reduced resistance to passive limb displacement; pendular reflexes |
| Rebound phenomenon | Failure to stop limb movement promptly when resistance is suddenly removed |
| Gait ataxia | Wide-based, lurching, irregular stride; difficulty with tandem walking |
Disease Classification
A. Vascular
- Posterior inferior cerebellar artery (PICA) infarction / Wallenberg syndrome — lateral medullary + cerebellar involvement → ipsilateral limb ataxia, vertigo, nausea, Horner syndrome
- Superior cerebellar artery (SCA) infarction — limb ataxia + possible CN IV palsy, contralateral sensory loss
- Cerebellar hemorrhage — sudden headache, vomiting, ataxia; may cause obstructive hydrocephalus (neurosurgical emergency)
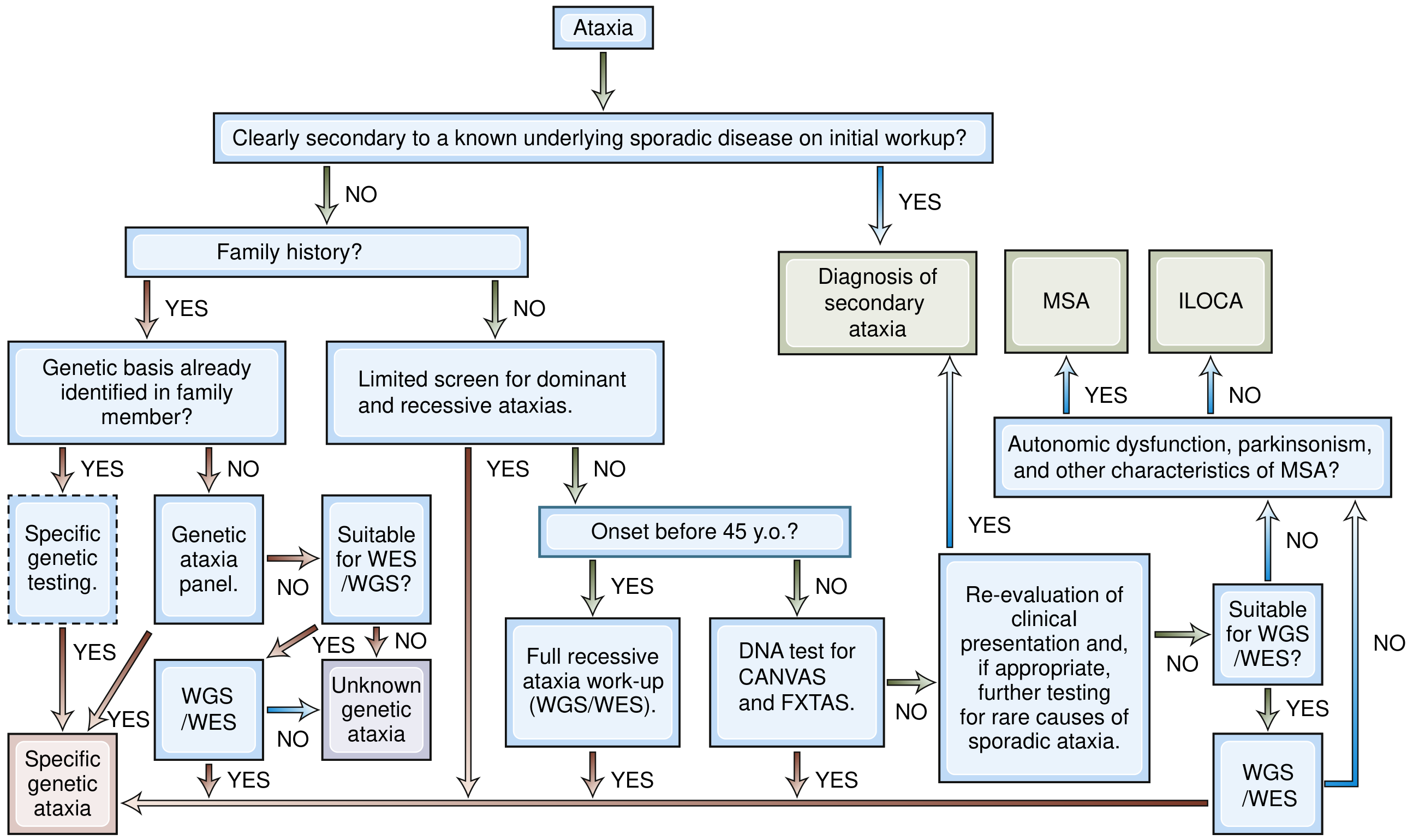
B. Genetic / Hereditary
Autosomal Dominant — Spinocerebellar Ataxias (SCAs)
-
50 subtypes (SCA1–3, 6, 7 most common); caused by CAG repeat expansions or point mutations
- SCA3 (Machado-Joseph disease): most common worldwide
- SCA2: slow saccades are a hallmark
- SCA6: pure cerebellar; CACNA1A calcium channel mutations
Autosomal Recessive
- Friedreich ataxia (most common hereditary ataxia): GAA repeat expansion in FXN (frataxin); onset <25 years; cerebellar ataxia + sensory neuropathy + cardiomyopathy + pes cavus + scoliosis; square-wave jerks on examination
- Ataxia telangiectasia: ATM gene mutation; cerebellar ataxia + telangiectasias + immunodeficiency + cancer predisposition
- Ataxia with vitamin E deficiency (AVED)
- CANVAS syndrome: cerebellar ataxia + neuropathy + vestibular areflexia (RFC1 biallelic expansions)
X-linked: Fragile X-associated tremor/ataxia syndrome (FXTAS) — older males with FMR1 premutation
C. Toxic / Metabolic
- Alcohol (most common acquired cause): anterior lobe atrophy → truncal and gait ataxia; Wernicke encephalopathy (thiamine deficiency) → similar picture acutely
- Drug toxicity: phenytoin, lithium, amiodarone, cytarabine
- Heavy metals: mercury, thallium
- Vitamin deficiencies: B1 (thiamine), B12, vitamin E
D. Immune-Mediated / Paraneoplastic
- Paraneoplastic cerebellar degeneration (PCD): anti-Yo (ovarian/breast), anti-Hu (SCLC), anti-Ri — subacute onset, pan-cerebellar degeneration
- Autoimmune cerebellitis: anti-GAD65 antibodies, anti-CASPR2, NMDAR antibodies
- Gluten ataxia: associated with celiac disease / anti-TTG antibodies
- Miller Fisher syndrome (GQ1b antibodies): ataxia + ophthalmoplegia + areflexia
E. Degenerative
- Multiple system atrophy — cerebellar type (MSA-C): cerebellar ataxia + autonomic dysfunction (orthostatic hypotension, urinary incontinence) ± parkinsonism
- Idiopathic late-onset cerebellar ataxia (ILOCA)
F. Infectious / Structural
- Cerebellar abscess, viral cerebellitis (varicella → acute cerebellar ataxia in children)
- Medulloblastoma (most common posterior fossa tumor in children): midline/vermis → truncal ataxia, hydrocephalus, papilledema
- Cerebellar astrocytoma, ependymoma, hemangioblastoma (VHL syndrome)
- Chiari malformation: cerebellar tonsil herniation → ataxia, headache, syrinx
G. Episodic Ataxias (EA)
- EA1 (KCNA1): brief attacks triggered by startle/exercise
- EA2 (CACNA1A): longer attacks (hours); responsive to acetazolamide
5. Clinical Testing of Cerebellar Function
Bedside Examination (SARA Scale Items)
1. Gait Assessment
- Observe normal walking, running, turning — look for variable stride length, veering, lurching
- Tandem gait (heel-to-toe): highly sensitive for subtle ataxia
- Wide-based gait = compensatory; subtle early ataxia may be detected only on tandem
2. Stance (Romberg-modified)
- Stand with feet together, then tandem stance, then on one foot
- Cerebellar ataxia: unsteady with eyes open (distinguishes from sensory ataxia which worsens with eyes closed)
3. Upper Limb Tests
- Finger-to-nose (FNT): patient alternately touches their nose and examiner's moving finger → reveals intention tremor (worsening oscillation near target) and dysmetria (over/undershoot)
- Finger chase: patient's index finger follows examiner's moving finger — tests smooth pursuit and control
- Rapid alternating movements (RAM) / dysdiadochokinesis: patient rapidly alternates pronation and supination — cerebellar damage → irregular rhythm and amplitude
- Rebound test: patient pushes against examiner's resistance; when resistance is suddenly released, cerebellar patient fails to arrest movement
4. Lower Limb Test
- Heel-knee-shin maneuver: supine; patient places heel on opposite knee and slides it down the shin to the ankle — ataxia causes the heel to deviate off the shin
- Toe-to-finger test: patient touches examiner's finger with great toe
5. Speech
- Assess for dysarthria / scanning speech: slow, irregular, syllables separated; explosive quality
6. Eye Movement Examination
- Gaze-evoked nystagmus: fast-phase toward the direction of gaze; slow-phase toward lesion
- Smooth pursuit: saccadic (jerky) pursuit suggests cerebellar dysfunction
- Saccades: dysmetric (hypermetric = overshoot; hypometric = undershoot)
- VOR suppression failure
7. Tone
- Test for hypotonia: reduced resistance to passive movement; pendular knee reflex (leg oscillates multiple times after patellar tap instead of stopping)
Laboratory and Imaging Investigations
| Investigation | Purpose |
|---|---|
| MRI brain (posterior fossa) | First-line; identifies structural causes (infarct, hemorrhage, tumor, atrophy pattern) |
| Serum vitamins (B1, B12, E) | Rule out nutritional ataxias |
| Paraneoplastic antibody panel (anti-Yo, anti-Hu, anti-Ri, anti-GAD65) | Immune-mediated / paraneoplastic |
| Genetic testing (repeat expansion panels, WES/WGS) | Hereditary ataxias — start with repeat expansions (SCA1/2/3/6/7, Friedreich, FXTAS) |
| CSF (cells, protein, oligoclonal bands) | Multiple sclerosis, infectious, autoimmune |
| Thyroid function, LFTs, toxicology screen | Metabolic/toxic causes |
| Anti-TTG / endomysial antibodies | Gluten ataxia |
Quick Summary Table
| Domain | Key Points |
|---|---|
| Structure | 3 lobes, 3 peduncles, 3 cortical layers, 4 deep nuclei (dentate > interposed > fastigial) |
| Output | Purkinje cells (inhibitory) → deep nuclei → SCP → thalamus → cortex |
| Input | Mossy fibers (via pontine nuclei) + climbing fibers (from inferior olive) |
| Function | Coordination, timing, motor learning, balance, posture, (non-motor: cognition/affect) |
| Lesion rule | Ipsilateral deficits; vermis = truncal; hemispheres = appendicular |
| Hallmark signs | Ataxia, dysmetria, intention tremor, dysdiadochokinesis, nystagmus, hypotonia |
| Common diseases | Alcohol toxicity, stroke (PICA), Friedreich ataxia, SCAs, MSA-C, paraneoplastic |
| Key bedside tests | Finger-to-nose, RAM, heel-knee-shin, tandem gait, gaze-evoked nystagmus |
Sources: Eric Kandel — Principles of Neural Science, 6th Ed. | Bradley and Daroff's Neurology in Clinical Practice | Ganong's Review of Medical Physiology, 26th Ed. | Costanzo Physiology, 7th Ed. | Guyton and Hall Textbook of Medical Physiology | Harrison's Principles of Internal Medicine, 22nd Ed. | Neuroanatomy through Clinical Cases, 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.