Explain me PathoMechanics & biomechanics of hip then forces acting on hip 15 marks MPT level answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Searching the Web
hip joint biomechanics pathomechanics MPT level forces acting coxa vara valga Trendelenburg
I now have comprehensive content from Campbell's Operative Orthopaedics, THIEME Atlas, Bailey & Love's, and Rockwood & Green's. Let me now compile the full MPT-level answer.
Pathomechanics & Biomechanics of the Hip Joint, and Forces Acting on the Hip
[MPT-Level Answer | 15 Marks]
PART I: BIOMECHANICS OF THE HIP JOINT
1. Structural Basis for Biomechanics
The hip (coxofemoral) joint is a ball-and-socket (spheroidal) joint formed by the femoral head articulating within the acetabulum of the pelvis. Its design allows a wide range of motion while remaining well-constrained - stability is derived not only from its bony architecture but from its role as the fulcrum about which large surrounding muscles act. These muscular actions force the femoral head deeper into the acetabulum, taking advantage of its depth.
Key structural features:
- The femoral head forms approximately two-thirds of a complete sphere; its articular cartilage is thickest on the medial and central surfaces - corresponding to the primary loading zone.
- The acetabular cartilage is horseshoe-shaped and thickest laterally and peripherally, reflecting a peripherally dominant loading pattern.
- The acetabular labrum adds more than 10% to femoral head coverage, making the joint functionally deeper. It takes >400 N of force to distract the hip joint.
- The capsule is reinforced by three ligaments: iliofemoral (Y-ligament of Bigelow) - strongest, pubofemoral, and ischiofemoral. The iliofemoral ligament limits extension and external rotation; the pubofemoral limits abduction; ischiofemoral limits internal rotation.
(Campbell's Operative Orthopaedics 15th Ed, p. 2581; Rockwood & Green's 10th Ed)
2. Axes of Motion and Degrees of Freedom
As a spheroidal joint, the hip has 3 degrees of freedom with all axes passing through the center of the femoral head:
| Axis | Motion |
|---|---|
| Transverse axis | Flexion (0-140°) / Extension (0-20°) |
| Sagittal axis | Abduction (0-45°) / Adduction (0-30°) |
| Longitudinal axis | Internal rotation (0-40°) / External rotation (0-50°) |
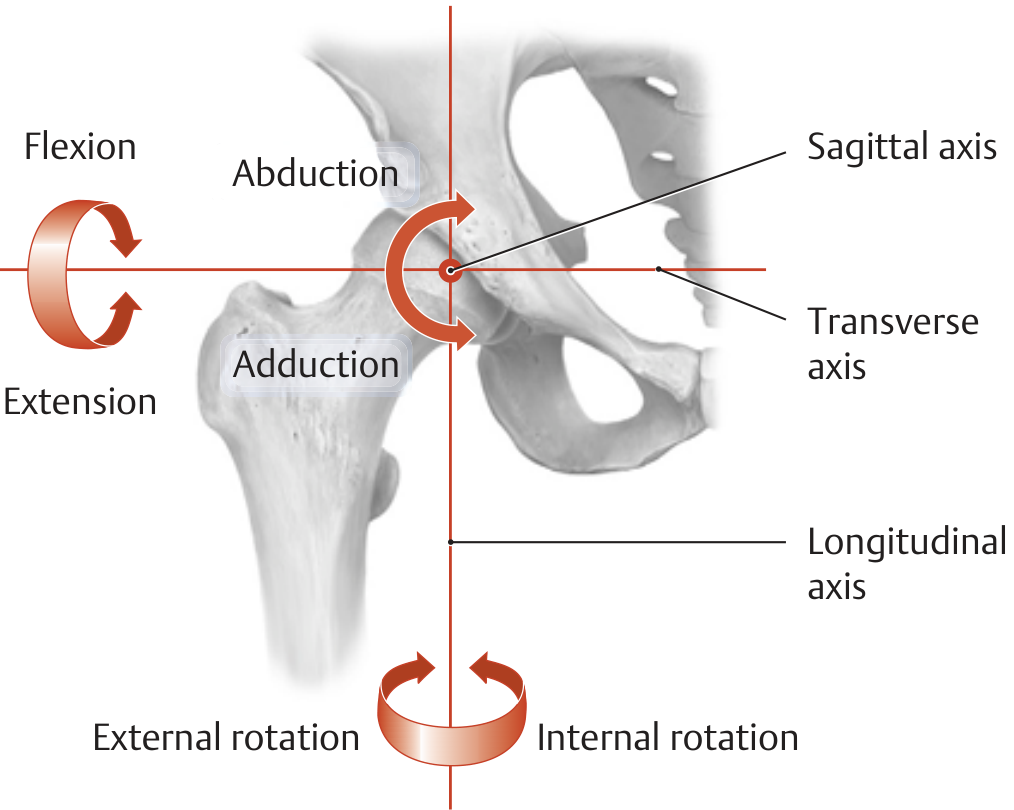
(THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, p. 456)
3. Osseous Angles and Their Biomechanical Significance
a. Neck-Shaft Angle (CCD Angle - Centrum-Collum-Diaphysis)
- Normal: 125-126°
- This angle provides femoral offset, separating the shaft laterally from the pelvis and allowing freedom of motion.
- Variation from normal significantly alters hip joint loading.
b. Femoral Anteversion
- Normal: approximately 12°
- Determines the position of the femoral head within the acetabulum and strongly influences rotation.
- Increased anteversion: excessive internal rotation gait (in-toeing)
- Decreased anteversion/retroversion: external rotation gait (out-toeing)
c. Acetabular Inclination (Wiberg's CE Angle)
- Normal: 25-40° - reflects lateral coverage of the femoral head
- Reduced coverage (dysplasia) concentrates stress on smaller cartilage areas, accelerating OA.
4. Weight-Bearing Mechanics - The Lever System
The hip joint operates as a first-class lever during single-limb stance. The three components are:
- Fulcrum: Center of the femoral head
- Load (effort arm): Body weight (HAT - head, arms, trunk) acting through the body's center of gravity, located medial to the stance hip
- Effort (resistance arm): Abductor muscle force acting through the greater trochanter, lateral to the femoral head
The lever arm of body weight (from center of gravity to center of femoral head) is approximately 2.5 times longer than the abductor lever arm (from greater trochanter to center of femoral head). To maintain pelvic level during single-limb stance, the abductor muscles must therefore generate a force of approximately 2.5 times body weight.
The resultant joint reaction force (R) = Body weight component + Abductor muscle force:
R = body weight (K) + abductor muscle force (M) In single-limb stance: R ≈ 3-4 times body weight
This can be calculated using:
R = √(K² + M² + 2KM·cosθ)
where θ is the angle between the two force vectors.
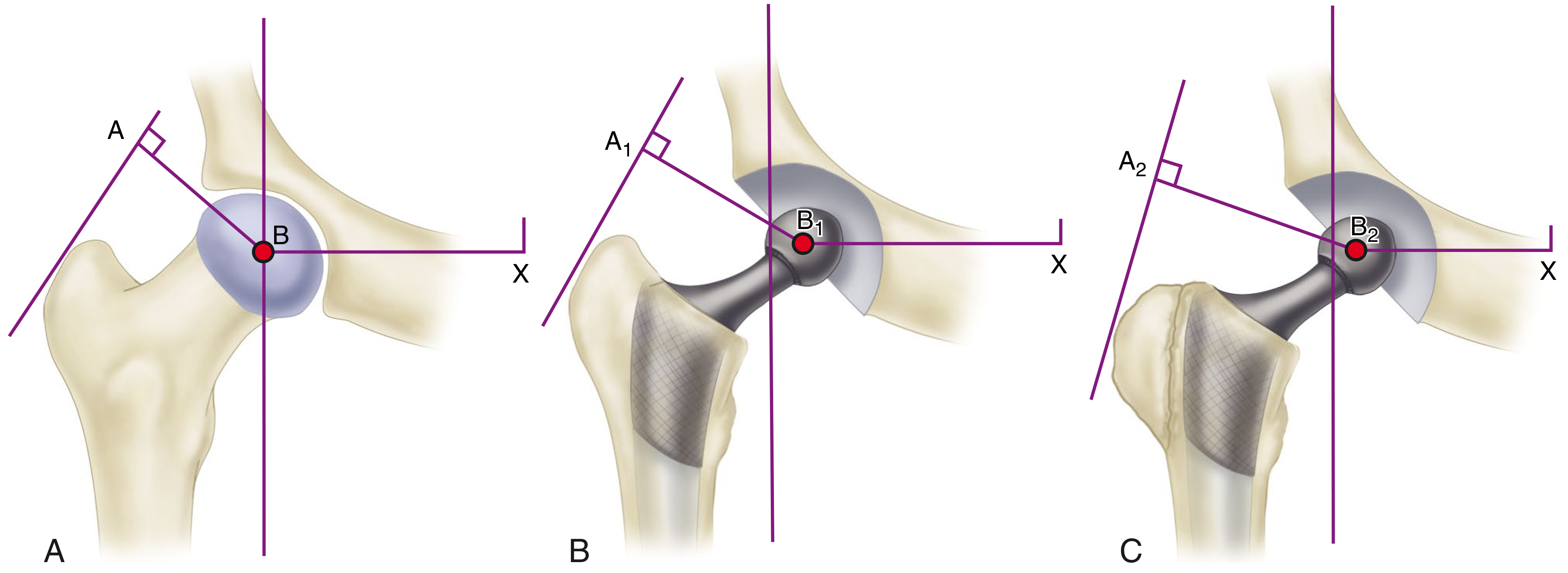
Figure: (A) Normal hip - body weight lever arm B-X is 2.5x abductor lever arm A-B. (B) Medialization of acetabulum shortens B1-X; high-offset neck lengthens A1-B1. (C) Lateral/distal reattachment of trochanter lengthens A2-B2 further, reducing joint reaction force.
(Campbell's Operative Orthopaedics 15th Ed, p. 191)
PART II: FORCES ACTING ON THE HIP
5. Joint Reaction Force (JRF) in Different Activities
| Activity | Joint Reaction Force (multiples of body weight) |
|---|---|
| Double-limb stance | ~1/3 body weight |
| Lifting leg from bed (straight leg raise) | ~1.5 × BW |
| Normal walking (stance phase) | ~3-4 × BW |
| Single-limb stance | ~3-4 × BW |
| Getting onto a bedpan | >2 × BW |
| Running / jumping | ~8-10 × BW |
Key clinical point: During the swing phase of gait, the weight of the hanging leg itself generates a JRF greater than body weight - relevant for rehabilitation. Experimentally measured forces using instrumented prostheses are in the range of 2.6-3.0 × BW during single-limb stance.
(Bailey & Love's Surgery 28th Ed, p. 572; Campbell's Operative Orthopaedics 15th Ed, p. 227; Rockwood & Green's 10th Ed)
6. Multi-Planar Nature of Hip Forces
Forces at the hip do not act in the coronal plane alone:
- Coronal plane forces: Tend to deflect the femoral stem medially (varus bending moment)
- Sagittal plane forces: Because the body's center of gravity (anterior to S2) is posterior to the joint axis, forces in the sagittal plane tend to deflect the stem posteriorly. These forces are amplified when the hip is flexed - e.g., during stair-climbing, rising from a chair, or lifting.
- Combined torsion: The combination of coronal and sagittal forces produces torsion of the femoral stem - important in THA stem design and fixation.
During gait, the resultant force is directed against the femoral head from a polar angle of 15-25° anterior to the sagittal plane of the prosthesis.
7. Effect of Neck-Shaft Angle on Hip Loading
The THIEME Atlas provides an elegant model for this:
- Normal CCD angle (~126°): Abductor lever arm ≈ 1/3 of body weight lever arm → R ≈ 4 × body weight (K)
- Coxa Valga (increased CCD angle): The abductor lever arm shortens because the greater trochanter is positioned more proximally and medially. The abductors must generate greater force to balance the pelvis → R increases to ~7 × K. This increases articular cartilage stress and predisposes to OA.
- Coxa Vara (decreased CCD angle): The abductor lever arm lengthens because the trochanter is displaced more laterally. Abductors require less force → R decreases to ~3 × K. However, increased bending stress is placed on the femoral neck, predisposing it to fracture.
Clinical Note: This is the biomechanical rationale behind intertrochanteric osteotomies - changing the neck-shaft angle surgically can reduce or redistribute hip joint loading.
(THIEME Atlas, p. 457)
PART III: PATHOMECHANICS OF THE HIP
8. Trendelenburg Gait and Abductor Insufficiency
The abductor muscles (gluteus medius, gluteus minimus) insert at the greater trochanter and must generate sufficient force to keep the pelvis level when standing on the ipsilateral leg. When the abductors are insufficient:
Trendelenburg sign (positive): The pelvis drops to the contralateral (unsupported) side during single-limb stance on the affected side - because the abductors fail to generate adequate counter-moment.
Trendelenburg gait (compensated): The patient lurches the trunk over the stance leg, shifting the body's center of gravity directly over the femoral head. This reduces the lever arm of body weight to near zero, minimizing the abductor moment required. This compensation reduces the JRF but causes the characteristic lurching or waddling gait.
Causes of abductor insufficiency:
- Gluteus medius/minimus weakness (nerve injury, disuse)
- Short abductor lever arm (coxa valga, lateral trochanteric migration, arthritis)
- Painful hip (antalgic gait - similar pattern adopted to relieve pain by reducing JRF)
9. Pathomechanics in Hip Dysplasia
In developmental dysplasia of the hip (DDH) or acetabular dysplasia:
- Reduced acetabular coverage concentrates load over a small cartilage area, dramatically increasing contact stress (P = F/A)
- The abductor lever arm is shortened because the trochanter is positioned posteriorly (external rotational deformity), mimicking the mechanics of coxa valga
- The body weight lever arm is relatively lengthened, increasing the JRF
- These combined effects accelerate articular cartilage degeneration and secondary OA
10. Pathomechanics in Hip Osteoarthritis
In established OA of the hip:
- Loss of articular cartilage and femoral head architecture alters the position of the center of rotation
- The abductor lever arm may shorten further (ratio of body weight lever arm to abductor lever arm becomes 4:1 vs. normal 2.5:1)
- This demands even greater abductor muscle force and elevates JRF disproportionately
- Osteophytes form at the acetabular rim and femoral head-neck junction, altering loading patterns
- Pain inhibits abductor activation, triggering the antalgic/Trendelenburg gait pattern
- In protrusio acetabuli, the femoral head migrates medially, shortening the body weight lever arm but also shortening the abductor lever arm
11. Pathomechanics in Femoroacetabular Impingement (FAI)
FAI arises when osseous deformity of the femoral head-neck junction (cam type), acetabular rim (pincer type), or both causes abnormal contact during hip motion:
- Cam FAI: Non-spherical femoral head enters the acetabulum during flexion/internal rotation, shearing the acetabular cartilage from the labrum at the anterosuperior acetabulum
- Pincer FAI: Over-coverage of the acetabular rim causes linear impingement between the rim and femoral neck, crushing the labrum
- Chronic labral damage leads to chondrolabral separation and eventual OA
- Osseous deformities limit range of motion in all planes and increase compensatory lumbopelvic motion, loading the lumbar spine
12. Femoral Neck Stress Fractures - Pathomechanical Basis
The femoral neck experiences both compressive and tensile forces during loading:
- Superior neck: Under tension (tensile stress - inferior trabecular group is primary compression carrier)
- Inferior neck: Under compression
- The femoral neck's bending moment increases with varus loading, coxa vara geometry, osteoporosis, or muscle fatigue (fatigue fractures in athletes)
- The calcar femorale (dense cortical bone posteromedially at femoral neck base) is the primary compressive stress concentrator
13. Biomechanical Rationale for Clinical Interventions
| Problem | Biomechanical Solution | Effect |
|---|---|---|
| Shortened abductor lever arm (arthritis, DDH) | Medialization of acetabulum + high-offset femoral stem | Restores lever arm ratio toward 1:1, reduces JRF by ~30% |
| Insufficient abductor lever arm after THA | Lateral/distal reattachment of greater trochanter after osteotomy | Maximally lengthens abductor lever arm A-B |
| Coxa valga | Varus intertrochanteric osteotomy | Increases abductor lever arm, reduces JRF |
| Coxa vara | Valgus intertrochanteric osteotomy | Distributes femoral neck bending stress |
| Hip OA with pain | Walking stick (contralateral hand) | Forces contralateral hand push = reduces abductor demand on affected hip by ~30% |
SUMMARY TABLE: Key Forces
| Parameter | Value |
|---|---|
| Abductor lever arm: body weight lever arm ratio | 1 : 2.5 (normal) |
| Abductor force required (single-limb stance) | ~2.5 × BW |
| JRF (double-limb stance) | ~1/3 BW |
| JRF (single-limb stance/walking) | 3-4 × BW |
| JRF (running/jumping) | 8-10 × BW |
| JRF (coxa valga, single limb) | ~7 × BW |
| JRF (coxa vara, single limb) | ~3 × BW |
| Force to distract hip joint | >400 N |
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Applied Biomechanics & Forces Acting on the Hip, p. 191-227
- Bailey and Love's Short Practice of Surgery 28th Ed, Biomechanics of the Hip Joint, p. 572
- Rockwood and Green's Fractures in Adults 10th Ed 2025, Biomechanics, p. 2581
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, The Movements and Biomechanics of the Hip Joint, p. 456-457
Explain this in simple language
Here's the entire topic explained in simple, easy-to-understand language:
Hip Joint - Biomechanics, Pathomechanics & Forces (Simple Explanation)
PART 1: WHAT IS THE HIP JOINT AND HOW DOES IT WORK?
Think of it like a Ball in a Cup
The hip joint is simply a ball-and-socket joint. The rounded head of the thigh bone (femur) is the "ball," and the cup-shaped hollow in the pelvis (acetabulum) is the "socket."
- The ball fits about 2/3 into the socket - not fully, which allows movement
- A rubber-ring-like structure called the labrum makes the socket slightly deeper and grips the ball tighter
- Strong ligaments (like rubber bands) wrap around the joint to hold everything together
- It takes more than 400 Newtons of force just to pull the ball out of the socket - it's very stable
PART 2: HOW THE HIP MOVES (3 Directions)
The hip can move in 3 directions because the ball can spin in any direction inside the socket:
| Direction | Movement |
|---|---|
| Front-to-back (transverse axis) | Bending (flexion) and straightening (extension) - like kicking a ball |
| Side-to-side (sagittal axis) | Spreading legs apart (abduction) and bringing together (adduction) |
| Spinning (longitudinal axis) | Rotating inward and outward - like turning your foot in/out |
Normal range:
- Flexion: 0-140° (you can bring your knee to your chest)
- Extension: 0-20° (you can push your leg backward)
- Abduction: 0-45°, Adduction: 0-30°
- Rotation: 40° inward, 50° outward
PART 3: THE IMPORTANT ANGLES OF THE HIP BONE
Neck-Shaft Angle (like the angle of a walking stick handle)
The thigh bone has a neck that connects the shaft (long part) to the ball (head). The angle between the neck and shaft is called the CCD angle or neck-shaft angle.
- Normal = 125-126°
- This angle creates a gap between the thigh bone and the pelvis, which is what allows your leg to move freely
If this angle changes:
- Too big (>130°) = Coxa Valga - the ball sits more upright, neck too straight
- Too small (<120°) = Coxa Vara - the neck is too tilted downward
Think of it like this: if you hold a walking stick at the wrong angle, it won't support your weight properly. Same thing happens with the hip.
Femoral Anteversion (how much the neck is twisted forward)
- Normal twist = 12° forward
- Too much twist forward = your toes naturally point inward when you walk (in-toeing)
- Too little/backward twist = your toes point outward when you walk (out-toeing)
PART 4: FORCES ACTING ON THE HIP - THE SEESAW EXPLANATION
Picture a Seesaw (Lever)
When you stand on one leg, your hip joint works like a seesaw (first-class lever):
FULCRUM (Center of femoral head)
|
Body weight lever (long side) | Abductor muscle lever (short side)
(from your center of gravity) | (from greater trochanter)
- Your body weight (everything above the hip - trunk, arms, head) presses DOWN on the LONG side of the seesaw
- Your hip abductor muscles (the muscles on the outer side of your hip - mainly gluteus medius) pull UP on the SHORT side to balance the seesaw
- The long side (body weight arm) is 2.5 times longer than the short side (muscle arm)
So what does this mean?
Because the body weight side is 2.5x longer, to keep the seesaw balanced, the muscles have to pull with a force that is 2.5 times your body weight!
If you weigh 70 kg → your abductor muscles must pull with force equal to 175 kg just to keep your pelvis level!
The Total Force on the Hip Joint
The hip joint has to handle BOTH forces at the same time:
- Body weight pushing down
- Abductor muscles pulling up
So the total force crushing the hip joint = abductor force + body weight component = about 3-4 times your body weight
If you weigh 70 kg (700 N) → the hip joint experiences about 2100-2800 N of force just while walking!
PART 5: FORCES IN DIFFERENT ACTIVITIES
| What you're doing | Force on the hip |
|---|---|
| Standing on both legs | Very low (~1/3 body weight) - muscles barely needed |
| Lifting your leg up straight | ~1.5 × body weight |
| Normal walking | 3-4 × body weight |
| Standing on one leg | 3-4 × body weight |
| Climbing stairs or getting off a chair | 4-5 × body weight |
| Using a bedpan (bedridden patient) | >2 × body weight |
| Running | ~6 × body weight |
| Jumping | 8-10 × body weight |
Key insight: Even during the swing phase (when your foot is in the air), the weight of the hanging leg alone creates a force greater than body weight at the hip. This is why even partial weight bearing is not truly "resting" the hip.
PART 6: HOW NECK-SHAFT ANGLE CHANGES THE FORCES
Coxa Valga (angle too big) - More Force on the Joint
When the neck is too upright (coxa valga):
- The greater trochanter is pushed inward and upward
- This shortens the muscle's lever arm (the short side of the seesaw gets even shorter)
- The muscles now have to work even harder to balance the pelvis
- Total force on the hip goes up to ~7 × body weight
- Over time, this extra stress wears out the cartilage → Osteoarthritis
Coxa Vara (angle too small) - Less Force on the Joint, But Different Problem
When the neck is too tilted (coxa vara):
- The greater trochanter is pushed outward
- This lengthens the muscle's lever arm (the short side of the seesaw gets longer)
- Muscles don't have to work as hard
- Total force on the hip reduces to ~3 × body weight
- BUT - the neck itself takes more bending stress → risk of femoral neck fracture
Simple rule: Surgeons can do an operation (osteotomy) to change this angle and reduce hip pain/OA by redistributing forces.
PART 7: FORCES IN MULTIPLE PLANES
Forces on the hip don't just push straight down. They act in two directions:
-
Side to side (coronal plane): Tends to push the femur inward (like a varus bending force) - like a tree bending in side wind
-
Front to back (sagittal plane): Your body's center of gravity is actually slightly BEHIND the hip joint. This creates a force that pushes the hip backward. This force increases a lot when you:
- Bend your hip (getting off a chair)
- Climb stairs
- Lift heavy objects
The combination of these two forces creates a twisting (torsional) stress on the femoral neck - like wringing a towel from both ends simultaneously.
PART 8: PATHOMECHANICS (When Things Go Wrong)
What is Pathomechanics?
Pathomechanics = Abnormal mechanics due to injury or disease. It explains why people walk differently when the hip is damaged.
A. Trendelenburg Gait - The "Waddling Walk"
Normal situation: When you stand on your right leg, the right hip abductor muscles contract strongly to hold your pelvis level. The left (unsupported) side stays up.
When abductors are weak or the hip is painful:
- The muscles can't hold the pelvis level
- The pelvis on the opposite side drops down (positive Trendelenburg sign)
How the body compensates (Trendelenburg gait):
- The person leans their trunk sideways over the affected hip
- This shifts the body's center of gravity directly over the femoral head
- Now the body weight lever arm becomes almost zero
- The muscles barely need to work, and the force on the joint drops dramatically
- This is the "waddling" or "lurching" gait you see in hip patients
Causes:
- Weak gluteus medius (stroke, nerve damage, disuse)
- Short abductor lever arm (hip OA, DDH)
- Pain (patient deliberately leans to avoid pain)
B. Pathomechanics in Hip Arthritis (OA)
When cartilage wears away in OA:
- The femoral head changes shape, altering the center of rotation
- The abductor lever arm shortens (ratio worsens from 2.5:1 to 4:1)
- This means muscles must work even harder → joint force goes up even more
- More force → more cartilage damage → more OA → vicious cycle
- Pain inhibits muscle use → Trendelenburg gait → uneven loading → worsens OA
C. Pathomechanics in Hip Dysplasia (DDH)
In DDH, the socket (acetabulum) doesn't fully cover the ball:
- The same force is now spread over a smaller area of cartilage
- Pressure = Force ÷ Area → Pressure goes up dramatically on less cartilage
- This leads to early cartilage failure and OA even in young adults
- Also, the trochanter is often positioned poorly → abductor lever arm shortened → more force needed → higher joint reaction force
D. Pathomechanics in FAI (Femoroacetabular Impingement)
- In FAI, there's a bony bump on the femoral neck (cam type) or extra bone on the socket rim (pincer type)
- When you bend or rotate the hip, this bump jams into the socket
- It crushes and tears the labrum and cartilage at the front of the joint
- Over time → cartilage loss → OA
- Limited hip motion forces the lower back to compensate → lower back pain + hip pain
E. Pathomechanics of Femoral Neck Fractures
The femoral neck is under:
- Compression on the lower (inferior) surface
- Tension (pulling stress) on the upper (superior) surface
When bone is weak (osteoporosis), muscles are fatigued (long-distance runners), or sudden overload occurs, the neck snaps - usually on the tension side first.
PART 9: CLINICAL TRICKS TO REDUCE HIP FORCE
| Trick | Why it Works |
|---|---|
| Walking stick in opposite hand | The stick push creates an external force that helps balance the pelvis, reducing abductor demand by ~30% and cutting joint force |
| Losing weight | Less body weight = less force on the seesaw = less joint load |
| Varus osteotomy in coxa valga | Lengthens abductor lever arm → reduces muscle force needed → reduces JRF |
| High-offset hip replacement stem | Moves the ball further from the shaft → lengthens abductor lever arm → reduces force |
| Medializing the hip socket (in THA) | Brings center of rotation closer to the body midline → shortens body weight lever arm → reduces JRF by ~30% |
QUICK REVISION SUMMARY
Normal hip forces:
- Walking = 3-4 × body weight
- Running = 8-10 × body weight
- Double stance = 1/3 body weight
Normal angles:
- Neck-shaft angle = 125°
- Anteversion = 12°
Key lever arm:
- Body weight arm : Abductor arm = 2.5 : 1
Coxa Valga → Abductor arm shortens → Force ↑ (7×BW) → OA risk ↑
Coxa Vara → Abductor arm lengthens → Force ↓ (3×BW) → Neck fracture risk ↑
Pathomechanics:
- Trendelenburg = abductor weakness → pelvis drops → trunk lean compensation
- OA = bad lever arm → more force → more damage
- Dysplasia = small surface area → high pressure → early OA
- FAI = bony bump → impingement → labral tear → OA
This is the same knowledge as before - just explained as if you're picturing it step by step rather than reading a textbook. The key idea throughout is: the hip is a lever system, and anything that disturbs the lever arms or the joint surfaces changes the forces and leads to pathology.
This is a shared conversation. Sign in to Orris to start your own chat.