Hysterectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from both Berek & Novak's Gynecology and Sabiston's Textbook of Surgery. Let me compile a thorough answer.
Hysterectomy
Hysterectomy is the surgical removal of the uterus. It is one of the most commonly performed gynecologic operations in the United States, with leiomyomas and abnormal uterine bleeding each accounting for approximately 195,000 procedures annually.
Types of Hysterectomy
By Extent of Uterine Removal
| Type | What is Removed |
|---|---|
| Total hysterectomy | Uterine corpus + cervix |
| Supracervical (subtotal) hysterectomy | Uterine corpus only; cervix left in situ |
| Radical hysterectomy | Uterus + cervix + parametria + upper vaginal cuff + pelvic lymph nodes (for malignancy) |
By Route of Access
- Vaginal hysterectomy (VH) - the preferred route unless contraindicated
- Abdominal hysterectomy (total abdominal hysterectomy, TAH) - open laparotomy via low transverse (Pfannenstiel) or vertical midline incision
- Laparoscopic hysterectomy (LH) - includes laparoscopic-assisted vaginal hysterectomy (LAVH), total laparoscopic hysterectomy (TLH), and laparoscopic supracervical hysterectomy (LSH)
- Robotic-assisted laparoscopic hysterectomy - uses the da Vinci system; no proven advantage over conventional LH in randomized trials
Indications
The major indications for hysterectomy (National Hospital Discharge Survey, US 2010) are:
| Indication | Approx. Number/Year |
|---|---|
| Uterine leiomyomas | 195,000 |
| Abnormal uterine bleeding | 195,000 |
| Endometriosis | 83,000 |
| Pelvic organ prolapse | 74,000 |
| Benign ovarian neoplasms | 70,000 |
| Gynecologic cancer | 53,000 |
Other indications include:
- Intractable dysmenorrhea / chronic pelvic pain refractory to medical therapy
- Cervical intraepithelial neoplasia (CIN)
- Obstetric emergencies (postpartum hemorrhage, uterine rupture)
- Pelvic inflammatory disease (PID) with abscess not responding to treatment
- Adenomyosis
- Pelvic organ prolapse
Key principle: Hysterectomy for leiomyomas should be considered only in symptomatic patients who do not desire future fertility. Alternatives (myomectomy, endometrial ablation, uterine artery embolization, GnRH agonist) should be considered first.
Surgical Access - Choice and Comparison
Vaginal hysterectomy (VH) is the procedure of choice unless contraindicated, based on Cochrane review evidence (Aarts et al., 2015):
| Comparison | Key Finding |
|---|---|
| VH vs. abdominal | Shorter return to normal activities (mean -9.5 days); fewer complications |
| LH vs. abdominal | Shorter return to activities (mean -13.6 days); BUT more urinary tract injuries (OR 2.4) |
| LH vs. VH | No difference in primary outcomes; VH is less expensive |
| Robotic vs. LH | No difference in primary outcomes |
"Adopting published guidelines for choosing the route of hysterectomy increased the proportion performed vaginally to over 90% and reduced the ratio of abdominal to vaginal hysterectomy from 3:1 to 1:11."
- Berek & Novak's Gynecology, p. 1418
Remaining indications for laparotomy:
- Cardiopulmonary disease precluding pneumoperitoneum
- Suspected uterine malignancy requiring morcellation avoidance
- Severely distorted anatomy not amenable to laparoscopic/vaginal approach
- No access to surgeons skilled in minimally invasive techniques
Surgical Technique
Total Abdominal Hysterectomy (TAH) - Key Steps
(From Sabiston Textbook of Surgery, Figure 120.12)
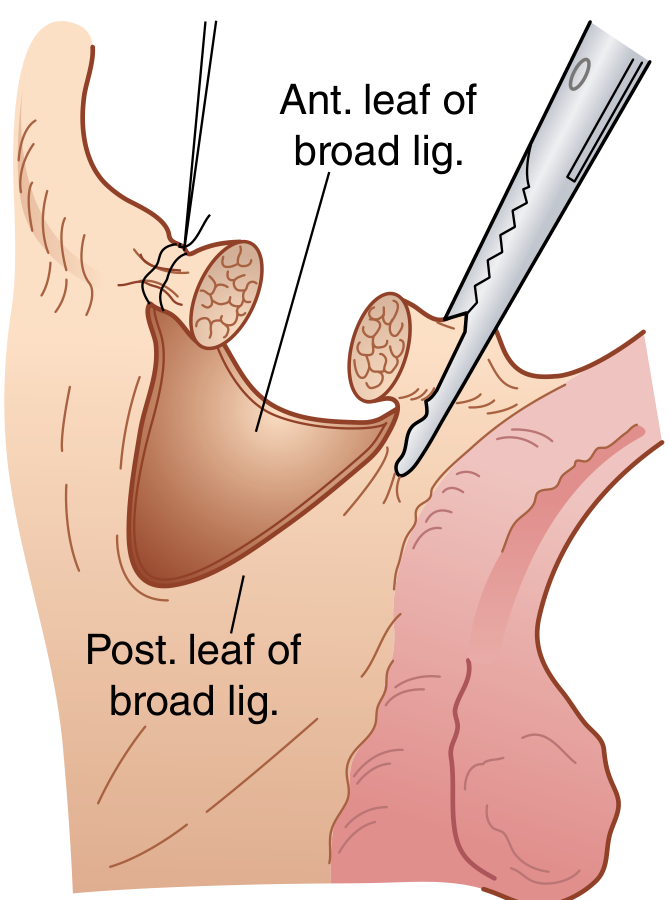
- Transect round ligaments bilaterally
- Incise anterior and posterior broad ligament
- Develop bladder flap - dissect bladder off the lower uterine segment/cervix
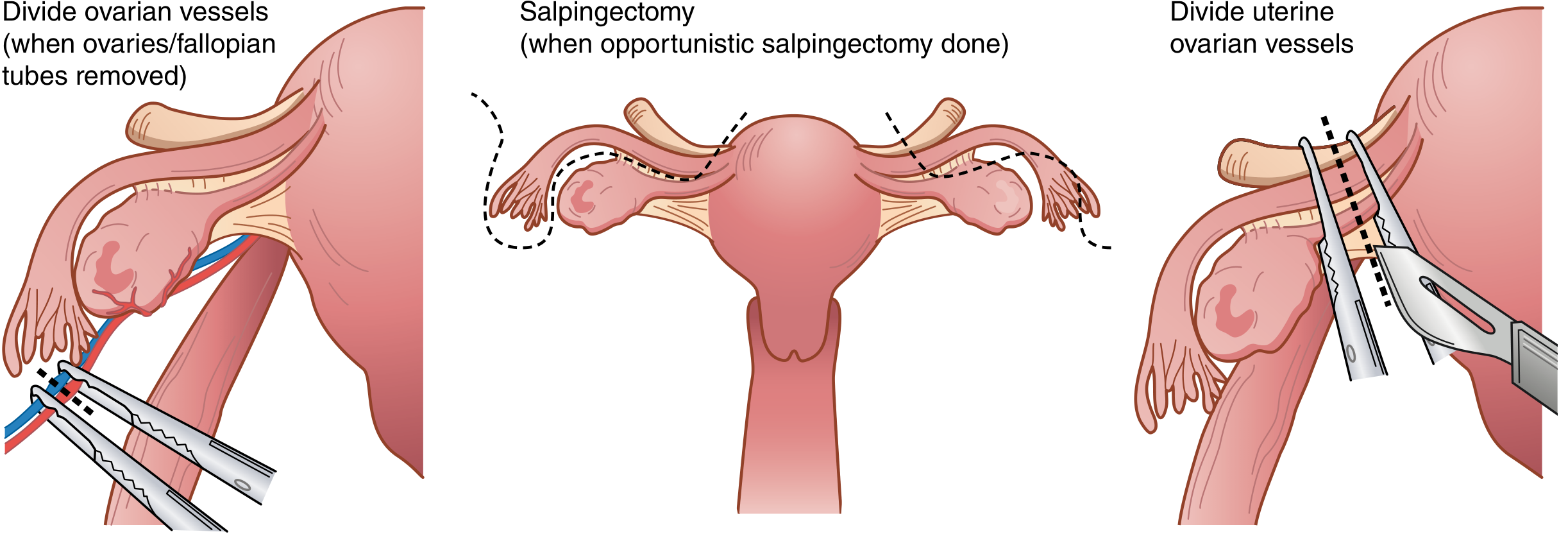
- Divide ovarian vessels (infundibulopelvic ligament) if bilateral salpingo-oophorectomy (BSO) is planned; or divide uteroovarian vessels to preserve ovaries
- Skeletonize and ligate uterine arteries at the level of the internal cervical os (clamp, cut, suture-ligate with delayed absorbable suture)
- Serial clamping and ligation of cardinal and uterosacral ligaments
- Colpotomy - circumferential incision of the vagina just below the cervix
- Close vaginal cuff - lateral angle sutures incorporate uterosacral ligaments for apical support
Vaginal Hysterectomy - Key Steps
The steps are in reverse order from abdominal:
- Circumferential colpotomy around cervix
- Enter posterior cul-de-sac; clamp/ligate uterosacral ligaments
- Dissect bladder anteriorly; enter anterior peritoneum
- Serial clamping of cardinal ligaments and uterine vessels
- Cornual pedicles (round ligament, tube, uteroovarian ligament) last
- Close colpotomy incorporating uterosacral ligaments (McCall culdoplasty if prolapse present)
Supracervical Hysterectomy
- Same as TAH until uterine artery ligation at the level of the internal cervical os
- Uterine corpus is amputated from the cervix
- Endocervix is cauterized; stump closed with figure-of-eight sutures
- Cervical cancer screening must continue per guidelines
- Contraindicated with malignant/premalignant uterine or cervical disease
Preoperative Considerations
Hysterectomy vs. Supracervical Hysterectomy
Three prospective RCTs (Cochrane review) show no advantage to leaving the cervix for:
- Sexual function
- Urinary incontinence rates
- Constipation
Supracervical hysterectomy does save ~11 minutes of operative time and avoids the most dangerous step in LH (detachment of cervix from lateral ligaments, where ureteral injuries most commonly occur). However:
- 5-20% risk of ongoing cyclic cervical bleeding
- 1-2% risk of reoperation (trachelectomy)
- Patients with endometrial hyperplasia, cervical dysplasia, or suspected malignancy are not candidates
Prophylactic Salpingo-Oophorectomy
- Premenopausal women at average ovarian cancer risk (~1.4% lifetime): ovarian conservation is strongly recommended - BSO before age 50 confers an 8.58% excess mortality by age 80 from cardiovascular disease
- Routine opportunistic salpingectomy (tubes only) is now recommended at hysterectomy as it may reduce ovarian cancer risk
- BSO is appropriate for BRCA1/BRCA2 carriers (44% and 17% lifetime risk of ovarian cancer, respectively)
VTE Prophylaxis
All hysterectomy patients are at minimum moderate VTE risk:
- Mechanoprophylaxis (intermittent pneumatic compression)
- Chemoprophylaxis (unfractionated or low-molecular-weight heparin)
- Combination, depending on individual risk level
Postoperative Cystoscopy
Many organizations advocate immediate postoperative cystoscopy at conclusion of hysterectomy to assess bladder integrity and confirm bilateral ureteral efflux.
Postoperative Complications
| Complication | Notes |
|---|---|
| Hemorrhage | Most common; uterine artery pedicle or vaginal cuff |
| Urinary tract injury | Higher with LH (OR 2.4 vs. abdominal); ureteral injury most common during lateral dissection near cervix |
| Urinary retention | More common after VH |
| Vesicovaginal fistula | Classic complication; abdominal > vaginal approach |
| Incisional infection / abscess | Vault granulations, cuff cellulitis |
| VTE | DVT/PE; minimally invasive routes reduce risk but prolonged OR time dampens benefit |
| Bowel injury | Risk with adhesiolysis |
| Sexual dysfunction | Most studies show improvement or no change; minority worsen (especially nerve injury in radical cases) |
Radical Hysterectomy
Used for treatment of cervical cancer (primarily). Involves removal of:
- Uterus + cervix
- Parametria (cardinal and uterosacral ligaments)
- Upper 1-2 cm of vaginal cuff
- Pelvic lymph node dissection
Nerve-sparing techniques have been developed to preserve the inferior hypogastric plexus within the cardinal and broad ligaments, improving bladder function and sexual outcomes compared to traditional radical hysterectomy. Meta-analysis confirms no worsening of oncologic prognosis with nerve-sparing technique.
Special Considerations
GnRH Agonist Pretreatment
For large leiomyomas (14-18 weeks' size), 8 weeks of leuprolide acetate before surgery:
- Reduces uterine size
- Allows conversion from abdominal to vaginal approach
- Associated with preoperative rise in hematocrit and shorter hospital stay
Hysterectomy for Pelvic Pain
- ACOG criteria: at least 6 months of pelvic pain without otherwise correctable pathology
- 74-77% of women report relief at 1 year
- ~25% have persistent or worsened pain (associated with multiparity, prior PID, absence of pathology)
- Hysterectomy is generally not indicated for CPP without identifiable uterine pathology
Sources:
- Berek & Novak's Gynecology, Chapter 27 (Hysterectomy), pp. 1408-1420
- Sabiston Textbook of Surgery, Chapter 120, pp. 2799-2802
- Aarts JWM et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2015;(8):CD003677
Cornus cancer syndrome
Reading File
Finding Sources
Finding Sources
Searching the Web
Cowden cancer syndrome PTEN hamartoma tumor syndrome clinical features management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compile a full answer.
Note on terminology: "Cornus cancer syndrome" is a phonetic spelling of Cowden (cancer) syndrome - also called Cowden disease or, more broadly, PTEN Hamartoma Tumor Syndrome (PHTS). This is the condition covered below.
Cowden Syndrome (Cowden Cancer Syndrome / PTEN Hamartoma Tumor Syndrome)
Definition
Cowden syndrome (CS) is a rare autosomal dominant inherited condition characterized by multiple hamartomas affecting tissues derived from all three germ layers, and a significantly elevated risk for several malignancies - primarily breast, thyroid, and endometrial cancers. It is the prototypical member of the PTEN Hamartoma Tumor Syndrome (PHTS) spectrum.
- Prevalence: ~1 in 200,000-250,000
- Penetrance: Nearly complete; 90% of affected individuals show stigmata by age 20
Genetics and Molecular Biology
The condition is genetically heterogeneous with 7 recognized types (CWS1-7):
| Type | Gene | Chromosome | Notes |
|---|---|---|---|
| CWS1 | PTEN (tumor suppressor) | 10q23.31 | Most common (~85%); main type |
| CWS2 | SDHB | 1p36.13 | Also linked to pheochromocytoma |
| CWS3 | SDHD | 11q13.1 | Also linked to pheochromocytoma |
| CWS4 | KILLIN promoter (hypermethylation) | 10q23.31 | Higher breast and renal cancer rates |
| CWS5 | PIK3CA | 3q26.32 | PI3K pathway |
| CWS6 | AKT1 | 14q32.33 | PI3K/Akt pathway |
| CWS7 | SEC23B | 20p11.23 |
Mechanism of PTEN: PTEN is a tumor suppressor gene that acts as a negative regulator of the Akt/PKB (PI3K) signaling pathway, which controls levels of phosphoinositol triphosphate and regulates cell cycle, apoptosis, and angiogenesis. Loss of PTEN function leads to uncontrolled cell proliferation.
In 10% of cases with no PTEN or promoter mutation, mutations occur in succinate dehydrogenase genes (SDHB/SDHD).
PHTS Spectrum
Cowden syndrome is the most clinically recognized disorder within the broader PHTS spectrum, which also includes:
- Bannayan-Riley-Ruvalcaba syndrome (BRRS) - earlier-onset variant; macrocephaly, penile lentigines, motor and speech delay, hamartomatous polyps, myopathies, lipomas, hemangiomas; >65% have PTEN mutations; now considered a PHTS variant
- PTEN-related Proteus syndrome
- PTEN-related Proteus-like syndrome
- Adult Lhermitte-Duclos disease (LDD)
- Autism spectrum disorder with macrocephaly
Clinical Features
Pathognomonic Mucocutaneous Findings
These are specific enough to be used as major diagnostic criteria:
- Multiple trichilemmomas (benign neoplasms differentiating toward outer root sheath) - present in 86% of CS patients; appear on average at age 22; located on central face (around nose, cheeks, orifices, ears)
- Acral keratoses - verrucous hyperkeratosis on extensor extremities (28%) and palmoplantar translucent keratoses (20%); acral neuromatosis may appear as translucent papules on fingers
- Papillomatous papules - multiple oral/mucosal papillomas

Oral papillomas producing the characteristic cobblestone tongue in Cowden syndrome - Andrews' Diseases of the Skin
- Mucosal lesions - present in >80% of patients; buccal and gingival mucosa most commonly involved; can coalesce into the characteristic cobblestone pattern (seen in 40% of patients)
- Macrocephaly (head circumference >97th percentile: ≥58 cm in females, ≥60 cm in males)
Other skin findings: Lipomas, hemangiomas, xanthomas, acanthosis nigricans, hyperpigmented macules, storiform collagenoma.
Systemic Features
| System | Feature | Notes |
|---|---|---|
| Breast | Fibrocystic disease (benign), adenocarcinoma | >75% of patients have breast abnormalities |
| Thyroid | Multinodular goiter, Hashimoto thyroiditis, follicular adenoma, follicular carcinoma | Thyroid abnormalities in ~2/3 of patients; <10% have frank carcinoma |
| GI tract | Hamartomatous polyps (intestinal, colonic) | Occur in 30-85% of cases; NOT significantly associated with increased CRC risk |
| CNS | Lhermitte-Duclos disease (dysplastic gangliocytoma of cerebellum), macrocephaly | Adult onset LDD is pathognomonic |
| Uterus | Endometrial carcinoma | Lifetime risk 13-20% |
| Kidney | Renal cell carcinoma | |
| Esophagus | Glycogenic acanthosis (≥3) | Minor criterion |
| Testis | Testicular lipomatosis | Minor criterion |
| Vascular | Vascular anomalies, intracranial developmental venous anomalies |
Cancer Risks
Malignancies develop in up to 40% of patients with Cowden syndrome:
| Cancer | Approximate Lifetime Risk |
|---|---|
| Breast cancer (female) | 25-50% |
| Breast cancer (male) | Reported (rare) |
| Endometrial cancer | 13-20% |
| Follicular thyroid cancer | ~10% of thyroid abnormalities |
| Renal cell carcinoma | Elevated |
| Colorectal cancer | Minor elevated risk (Minor criterion) |
Diagnostic Criteria (PTEN Hamartoma Tumor Syndrome / Cowden Syndrome)
Diagnosis is based on meeting established pathognomonic, major, and minor criteria:
Major Criteria
- Breast cancer
- Endometrial cancer (epithelial)
- Follicular thyroid cancer
- Multiple GI hamartomas or ganglioneuromas (≥3, excluding hyperplastic polyps)
- Lhermitte-Duclos disease (adult onset)
- Macrocephaly (≥97th percentile)
- Macular pigmentation of the glans penis
- Multiple mucocutaneous lesions (any of the following):
- Multiple trichilemmomas (≥3, at least one biopsy-proven)
- Acral keratoses (≥3 palmoplantar keratotic pits and/or acral hyperkeratotic papules)
- Mucocutaneous neuromas (≥3)
- Oral papillomas (multiple, ≥3; or biopsy-proven; or dermatologist-diagnosed)
Minor Criteria
- Autism spectrum disorder
- Colorectal cancer
- Esophageal glycogenic acanthosis (≥3)
- Lipomas (≥3)
- Intellectual disability (IQ ≤75)
- Renal cell carcinoma
- Testicular lipomatosis
- Papillary thyroid cancer or follicular variant of papillary thyroid cancer
- Thyroid structural lesions (adenoma, multinodular goiter)
- Vascular anomalies (including multiple intracranial developmental venous anomalies)
- Single GI hamartoma or ganglioneuroma
Operational diagnosis in an individual (either):
- Meeting certain major criterion combinations
- Three major criteria (one of which must be macrocephaly, LDD, or GI hamartomas)
- Two major and three minor criteria
Testing offered to relatives if they meet any major OR two minor criteria (in setting of an affected family member not yet tested molecularly).
Diagnosis
- Definitive: Identification of a heterozygous germline pathogenic variant in PTEN on molecular genetic testing
- Genetic counseling recommended for all patients and at-risk family members
- Prenatal testing possible once a family-specific pathogenic variant is identified
- Thyroid screening: neck ultrasonography + fine-needle aspiration with cytologic analysis
Histopathology of Trichilemmomas
- Variable hyperkeratosis and parakeratosis
- Tumor lobules extend downward from the epidermis
- Glycogen-rich clear cells, peripheral palisading
- Thick, hyalinized basement membrane (distinctive feature)
Management and Surveillance
Cancer Surveillance Recommendations
| Organ | Screening Modality | Start Age |
|---|---|---|
| Breast | Annual mammogram + breast MRI | Age 30-35 (or earlier based on family history) |
| Endometrium | Annual endometrial biopsy | Age 30-35 |
| Thyroid | Annual neck ultrasound | At diagnosis |
| Kidney | Renal imaging | Age 40 (or per guidelines) |
| Colon | Colonoscopy | Age 35, then every 5 years (or 5-10 years before earliest CRC in family) |
Skin Lesion Treatment
- Facial papillomas: surgical removal, dermabrasion, CO2 laser - but new lesions continue appearing throughout life
- Rapamycin (mTOR inhibitor) prevents development of mucocutaneous lesions and premature death in animal models, implicating the mTOR pathway in the cutaneous manifestations
Related Syndrome: Bannayan-Riley-Ruvalcaba Syndrome (BRRS)
BRRS is now considered an early-onset PHTS variant, sharing >65% PTEN mutation overlap with CS. It presents with:
- Macrocephaly + hypotonia
- Genital lentigines (pigmented speckling of the penis)
- Motor and speech delay, intellectual disability (in ~50%)
- Hypermobile joints
- Lipomas, hemangiomas
- Hamartomatous intestinal polyps (45% incidence)
Cancer risks in BRRS are not as well-defined but are considered analogous to Cowden syndrome; most authors recommend similar surveillance.
Sources:
- Andrews' Diseases of the Skin, pp. 774-775 (Trichilemmoma and Cowden Syndrome)
- Harrison's Principles of Internal Medicine, 22E (2025), p. 2007 (Cowden's syndrome genetics and screening)
- Mulholland & Greenfield's Surgery, p. 3349 (Cowden Syndrome/PHTS)
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed., p. 3522 (Clinical features)
- Pilarski R et al. Cowden Syndrome and the PTEN Hamartoma Tumor Syndrome. J Natl Cancer Inst 2013;105:1607-1616 (Revised diagnostic criteria)
This is a shared conversation. Sign in to Orris to start your own chat.