What are scapular dissociation exercises
Reading File
Searching the Web
scapular dissociation exercises rehabilitation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have enough context to give a thorough, accurate answer. The term "scapular dissociation exercises" does not exist as a formal clinical category in the orthopaedic literature — it conflates two distinct concepts:
- Scapulothoracic dissociation (STD) — a severe traumatic injury
- Scapular stabilization/isolation exercises — what people likely mean when using this term informally
Here is a comprehensive answer:
Scapular Dissociation: Clarifying the Term
"Scapular dissociation exercises" is not a standard clinical term. It appears in two very different contexts depending on who is using it:
1. Scapulothoracic Dissociation (STD) — The Medical Injury
This is the formal orthopaedic diagnosis. It is a rare, severe traumatic injury — effectively a closed internal forequarter amputation.
Mechanism: A violent lateral traction force separates the scapula from the thoracic cage, typically in motorcycle crashes (the rider grips the handlebars while the body is flung away) or industrial avulsion injuries.
Key features:
- Massive shoulder soft tissue swelling
- Clavicle distraction injury (AC separation, clavicle fracture, or SCJ dislocation)
-
1 cm lateral displacement of the scapula on AP chest X-ray (pathognomonic)
- Vascular injury (subclavian/axillary/brachial) in 65–100% of cases
- Neurologic injury (brachial plexus) in ~95% of cases
Classification (Zelle):
| Grade | Injury |
|---|---|
| 1 | Musculoskeletal only |
| 2A | + Vascular injury |
| 2B | + Incomplete neurologic deficit |
| 3 | + Incomplete neuro + vascular |
| 4 | + Complete brachial plexus avulsion |
Treatment: Focuses on neurovascular injury, not exercises. Grade 4 injuries (complete brachial plexus avulsion) often require above-elbow amputation. Outcomes are generally poor — 10% mortality, frequent flail/anesthetic limbs.
— Rosen's Emergency Medicine, Chapter 45; Rockwood and Green's Fractures in Adults, 10th ed.
2. Scapular Isolation / Stabilization Exercises — The Rehab Context
If you encountered "scapular dissociation exercises" in a physical therapy or fitness context, the term likely refers to exercises that isolate scapular movement independently from glenohumeral (shoulder) movement — sometimes called scapular dissociation from arm movement.
The goal is to train the periscapular muscles (serratus anterior, trapezius, rhomboids) to control the scapula as a stable base for shoulder function. These are used in:
- Rotator cuff rehabilitation
- Shoulder impingement
- Multidirectional instability (MDI)
- Scapular winging from serratus anterior weakness
Common exercises in this category include:
| Exercise | Primary Muscles | What It Does |
|---|---|---|
| Scapular retraction (squeeze shoulder blades together) | Middle/lower trapezius, rhomboids | Trains isolated retraction without arm elevation |
| Scapular protraction (wall push-up plus) | Serratus anterior | Isolates forward scapular movement |
| Scapular depression | Lower trapezius | Counters upper trapezius dominance |
| Scapular clock | All periscapular muscles | Guided movement through all planes |
| Prone Y-T-W raises | Lower/middle trapezius | Strengthens scapular stabilizers |
| Serratus punches | Serratus anterior | Scapular protraction in loaded position |
The principle is to dissociate (separate) scapular motion from arm motion — moving the scapula without lifting the arm — before progressing to integrated movements. This is critical because impaired scapular control (dyskinesis) underlies many shoulder conditions.
— Miller's Review of Orthopaedics, 9th ed. (scapular stabilization in MDI management)
Bottom line: If you're asking about the injury, STD is a surgical emergency. If you're asking about rehab exercises, the correct term is scapular stabilization or periscapular strengthening — let me know which context you're working in and I can go deeper on either.
Exercises with pictures
Searching Images
scapular stabilization exercises retraction protraction
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here are scapular stabilization exercises with clinical photographs from published rehabilitation research:
Scapular Stabilization Exercises
1. Scapular Retraction with Resistance Band
Target muscles: Middle trapezius, rhomboids

How to perform: Hold a resistance band at shoulder height with both hands, arms extended forward. Pull the band apart by drawing both arms out to the sides, squeezing the shoulder blades together. Hold 2–3 seconds, return slowly.
2. Wall Push-Up Plus, Lawnmower & Resisted Retraction
Target muscles: Serratus anterior (push-up plus), rhomboids/lower trapezius (lawnmower & band pull)
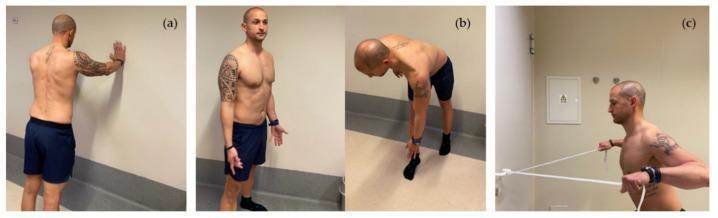
- (a) Wall push-up plus — At the end of the push, actively push the scapula away from the spine (protraction). This strongly activates serratus anterior, which keeps the scapula flat against the ribcage.
- (b) Lawnmower — Bend forward, reach toward the opposite foot, then stand upright pulling the elbow back like starting a lawnmower. Integrates trunk rotation with scapular retraction.
- (c) Resisted scapular retraction — Band anchored at chest height; pull back focusing on pinching the shoulder blades, not just pulling with the arm.
3. Side-Lying & Prone Dumbbell Series + Standing Protraction
Target muscles: Full periscapular muscle balance (upper, middle, lower trapezius; serratus anterior)
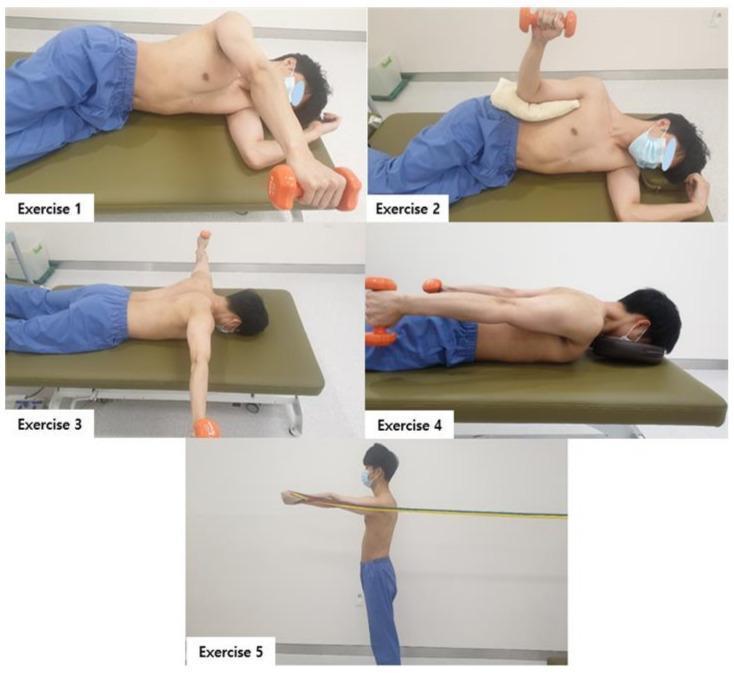
| # | Position | Movement | Muscle |
|---|---|---|---|
| 1 | Side-lying | External rotation with dumbbell | Infraspinatus, teres minor |
| 2 | Side-lying (towel roll in axilla) | Arm elevation | Deltoid + scapular upward rotators |
| 3 | Prone | Bilateral 90° abduction (T-raise) | Middle trapezius |
| 4 | Prone | Bilateral shoulder extension (Y-raise) | Lower trapezius |
| 5 | Standing | Scapular protraction against band | Serratus anterior |
4. Quadruped Push-Up Plus (Serratus Anterior Isolation)
Target muscles: Serratus anterior — the key scapular "dissociator"
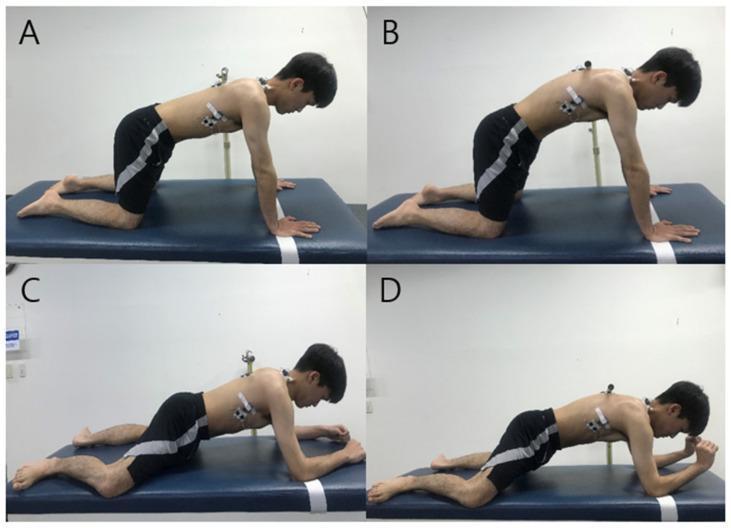
- (A→B) Knee Push-Up Plus: Start in quadruped (hands and knees). At the top, push the thorax away from the floor by maximally protracting both scapulae. The spine rounds slightly upward — this is the "plus" phase.
- (C→D) Modified 3-Point Support: Weight on elbows and knees; maintain spinal alignment while performing wrist extension. Lower demand, useful for early rehab.
5. Comprehensive Seated/Standing Program (Upper Crossed Syndrome Protocol)
Target muscles: Full shoulder girdle — useful for posture correction, desk workers, overhead athletes
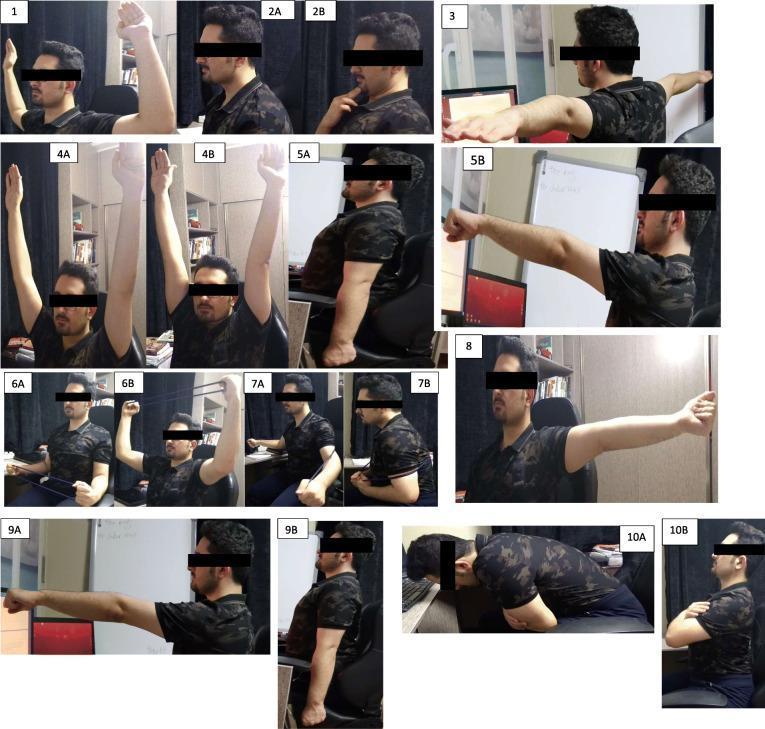
Key movements shown: W-shape external rotation, chin tucks, T-shape retraction/depression, overhead retraction, scapular plane elevation with band, dynamic hug (bilateral protraction), and thoracic extension.
Progression Principles
| Phase | Focus | Examples |
|---|---|---|
| 1 — Isolation | Move scapula without moving the arm | Scapular clocks, manual retraction/protraction |
| 2 — Closed chain | Arm fixed, body moves | Wall push-up plus, quadruped series |
| 3 — Open chain | Arm free with resistance | Band rows, prone Y-T-W, lawnmower |
| 4 — Integrated | Full kinetic chain movement | Overhead press with scapular control, sport-specific |
The goal throughout is to train the scapula as a stable platform — dissociated from, and in advance of, arm movement.
This is a shared conversation. Sign in to Orris to start your own chat.