Gingival buccal sulcus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here is a comprehensive overview of the gingival buccal sulcus (gingivobuccal sulcus / mucobuccal fold), drawing from multiple authoritative medical and surgical textbooks.
Gingival Buccal Sulcus (Gingivobuccal Sulcus / Mucobuccal Fold)
Anatomy and Definition
The term "gingival buccal sulcus" actually encompasses two related but distinct anatomical structures that are frequently discussed together:
1. The Gingival Sulcus (crevicular sulcus)
The gingival sulcus is the shallow V-shaped furrow (crevice) between the free gingival margin and the surface of the tooth. It is lined by crevicular (sulcular) epithelium, which is continuous with the junctional (attachment) epithelium at its base.
- Normal depth: 2-3 mm in a healthy individual
- Depths greater than 3 mm are considered a periodontal pocket, indicating pathology
- The depth is measured clinically with a periodontal probe and serves as the primary indicator of periodontal disease
-
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1661
2. The Buccal Sulcus / Mucobuccal Fold (Oral Vestibule Fornix)
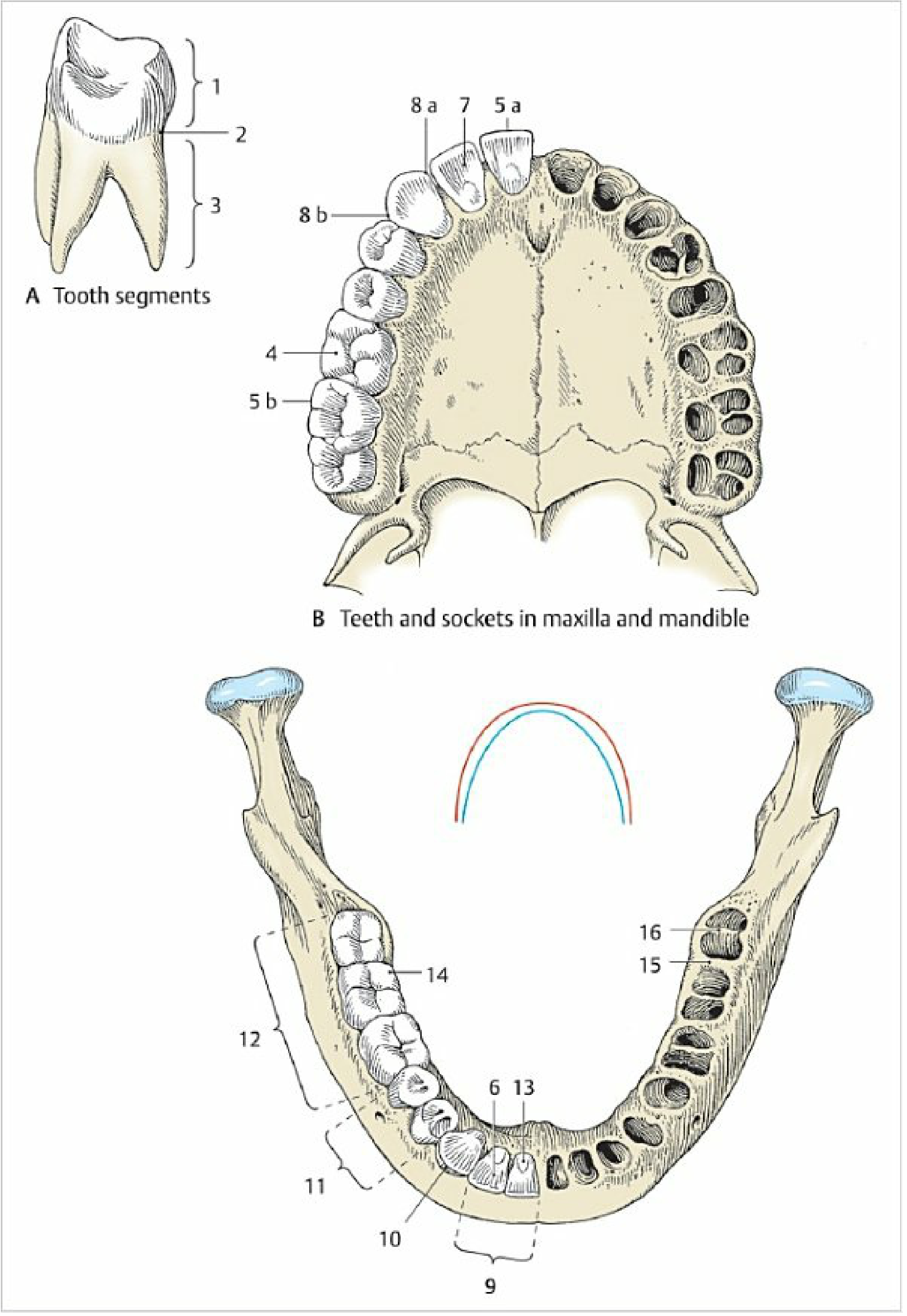
The buccal sulcus (or gingivobuccal sulcus) is the fold/groove formed where the gingiva (attached gum) reflects off the alveolar bone and transitions into the loose, mobile mucosa of the cheeks and lips. This creates the oral vestibule.
- The oral vestibule is bounded anteriorly by the lips, laterally by the cheeks, and internally by the teeth and alveolar processes of the maxilla and mandible
- The gingiva reflects on to the lips and cheeks forming the fornix, which has freely movable mucous membrane
- This junction is also called the mucogingival junction
-
- Color Atlas of Human Anatomy, Vol. 2, p. 244-245
Histology
The gingiva is composed of keratinized, stratified squamous epithelium and is divided into:
| Zone | Description |
|---|---|
| Free gingiva | Unattached cuff of tissue forming the gingival sulcus around the neck of the tooth |
| Attached gingiva | Firmly bound to underlying alveolar bone; extends apically to the mucogingival junction |
| Alveolar mucosa | Nonkeratinized; begins at the mucogingival junction and forms the buccal sulcus/fold |
The junctional (attachment) epithelium adheres to the tooth surface via a basal lamina and hemidesmosomes (the epithelial attachment). In young individuals this attachment is to enamel; in older individuals with gingival recession, it shifts to cementum. Above this attachment, the crevicular epithelium lines the gingival sulcus proper.
-
- Histology: A Text and Atlas (Pawlina), p. 1462-1463
Clinical Significance
1. Periodontal Assessment
A periodontal probe is inserted into the gingival sulcus to measure pocket depth. Bleeding on probing indicates inflammation (gingivitis or periodontitis). Sulcular depth >3 mm indicates loss of periodontal attachment.
-
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery
2. Dental Nerve Blocks (Local Anesthesia)
The mucobuccal fold (gingivobuccal sulcus) is the standard site for supraperiosteal injections (infiltration blocks):
- The lip is retracted to make tissues taut (down-and-out for maxillary, up-and-out for mandibular teeth)
- The needle is inserted at the mucobuccal fold with the bevel facing the tooth, inserted just a few millimeters
- The anesthetic diffuses through the periosteum to the tooth apex
- Also used for the infraorbital nerve block - the needle is directed through the mucobuccal fold over the maxillary second bicuspid, aimed at the infraorbital foramen
-
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 657-658
3. Surgical Access - Incisions
The buccal sulcus is a standard incision site in many oral and maxillofacial procedures:
| Procedure | Use |
|---|---|
| Genioplasty | Inferior buccal sulcus incision for access to mandibular symphysis |
| Rhytidectomy (facelift) | Superior buccal sulcus incision combined with temporal incisions |
| Zygomatic fracture reduction (Keen approach) | Mucogingival incision in the buccal sulcus of the molar/premolar region to pass an elevator behind the zygomatic body |
| Piriform aperture stenosis | Sublabial gingivobuccal sulcus incision with periosteal elevation |
| Upper cheek flap (oncologic) | Mucosal incision in the gingivolabial and gingivobuccal sulcus |
-
- Scott-Brown's Otorhinolaryngology; Mulholland and Greenfield's Surgery
4. Oral Cancer
The buccal-alveolar sulci (upper and lower vestibule) are specifically listed as subsites of the oral cavity in head and neck oncology. Squamous cell carcinoma (SCC) commonly arises here, particularly in tobacco-chewing populations where the substance is placed in the mandibular vestibule/buccal sulcus.
-
- Sabiston Textbook of Surgery; Scott-Brown's Otorhinolaryngology
5. Pathological Changes
- Crohn's disease: Linear ulcers in the depth of the buccal sulcus are a classic oral manifestation
- Tobacco-related lesions: Mucosal changes, erythroplakia, and carcinoma develop in sites where tobacco is habitually placed
- Gingivitis/Periodontitis: Inflammation leads to deepening of the sulcus into a true periodontal pocket
Summary
The gingival buccal sulcus is the anatomical space/fold at the junction between the fixed gingiva and the mobile mucosa of the cheeks. It is:
- A landmark for dental injections (supraperiosteal blocks, infraorbital blocks)
- A standard surgical incision site for facial and oral procedures
- A site for oral cancer subsites in the TNM staging system
- A zone whose depth (when referring to the gingival sulcus proper) reflects periodontal health
Image
It looks like you meant to attach an image but it didn't come through. Could you please re-upload the image you'd like me to analyze?


105133.jpg
105145.jpg
How to make use and uses explain about it in detail
Reading File
analyse_media
analyse_media
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Here is a complete, detailed guide on SustaGlar (Insulin Glargine) - what it is, how to use the pen, and its medical uses.
SustaGlar - Insulin Glargine Injection IP (rDNA Origin)
What Is It?
SustaGlar is a brand of Insulin Glargine 100 IU/mL, manufactured by Regenix Biosciences Ltd. (India). It comes as a 3 mL pre-filled disposable insulin pen for subcutaneous injection. It is a long-acting (basal) insulin analog that provides glucose control for a full 24 hours with a single daily dose.
Understanding the Pen Device
| Part | Description |
|---|---|
| Clear cartridge window (top) | Shows the insulin - should be clear, colorless, water-like fluid |
| Dose display window | Shows "0" when reset; dial shows the number of units to inject |
| Dose dial knob (bottom ribbed end) | Turn this to set your dose in units |
| Needle cap (teal/green, bottom) | Attach a fresh pen needle here before each injection |
| Plunger | Automatically advances as you inject |
How to Use the SustaGlar Insulin Pen - Step by Step
Before You Start
- Check the insulin - Look through the cartridge window. It should be clear and colorless. Do NOT use if it looks cloudy, colored, or has particles.
- Check the expiry date on the box and pen label.
- Remove the pen cap from the top.
Step 1 - Attach a New Needle
- Remove the protective tab from a fresh pen needle.
- Screw the needle firmly onto the pen tip (clockwise).
- Remove the outer and inner needle caps (keep the outer cap - you will need it to remove the needle safely after).
Step 2 - Prime the Pen (Air Shot)
- Dial 2 units on the dose knob.
- Point the pen upward and press the injection button.
- A small drop of insulin should appear at the needle tip.
- This removes air bubbles and confirms the pen is working.
- Repeat if no drop appears.
Step 3 - Set Your Dose
- Turn the dose dial to your prescribed number of units.
- The dose window will display the number clearly.
- If you dial past your dose, you can dial back down.
Step 4 - Choose Your Injection Site
Suitable sites (subcutaneous fat layer):
| Site | Notes |
|---|---|
| Abdomen (belly) | Most commonly used; away from navel by at least 5 cm |
| Outer thigh | Slower, more consistent absorption |
| Upper outer arm | Less preferred for self-injection |
| Buttocks | Slowest absorption |
- Rotate sites with each injection to prevent lipodystrophy (fat lumps under the skin).
- Clean the skin with an alcohol swab and let it dry.
Step 5 - Inject
- Pinch a fold of skin gently.
- Insert the needle at 90 degrees (straight in). For thin patients, 45 degrees may be used.
- Press the injection button all the way down and hold for 10 seconds before withdrawing - this ensures the full dose is delivered.
- Release the pinched skin.
- Do NOT rub the injection site.
Step 6 - Remove and Dispose of the Needle
- Replace the outer needle cap and unscrew the needle.
- Dispose of the needle in a sharps container.
- Never leave the needle on the pen during storage (this can cause leakage or air bubbles).
- Replace the pen cap.
When to Take It
- Insulin glargine is given once daily, at the same time every day (commonly at bedtime or in the evening, but the time should be consistent).
- It does NOT need to be given with meals (it is a basal/background insulin, not a mealtime insulin).
-
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Storage Instructions
| Condition | Rule |
|---|---|
| Unopened pen | Store in refrigerator (2°C - 8°C). Do NOT freeze. |
| In-use pen (opened) | Keep at room temperature (below 30°C) for up to 28 days. Do NOT refrigerate once in use. |
| Protect from | Direct sunlight, heat, freezing |
Medical Uses (Indications)
1. Type 1 Diabetes Mellitus (T1DM)
Used as basal insulin alongside rapid-acting mealtime insulin. It provides a steady, low-level background insulin throughout the day and night. It must always be given as a separate injection and cannot be mixed with other insulins.
-
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 3757
2. Type 2 Diabetes Mellitus (T2DM)
Used when oral antidiabetic drugs are no longer enough to control blood sugar. Glargine is typically started at a low dose (10 units/day or 0.1-0.2 units/kg/day) and titrated upward based on fasting glucose readings.
-
- Textbook of Family Medicine, 9th Ed.
3. Gestational Diabetes / Diabetes in Pregnancy
Insulin glargine is used in pregnancy when insulin is required for glucose control. Safety data are generally reassuring, though each case should be evaluated individually.
-
- Creasy & Resnik's Maternal-Fetal Medicine
4. Perioperative Diabetes Management
On the day of surgery, glargine may be given at 50% of the usual dose to maintain some basal coverage while reducing hypoglycemia risk during fasting.
-
- The Washington Manual of Medical Therapeutics
How It Works (Mechanism of Action)
Insulin glargine is an engineered analog of human insulin:
- Two arginine molecules are added to the B-chain C-terminal.
- Glycine replaces asparagine at position A21.
- This makes the molecule soluble at acidic pH (pH 4.0) in the pen, but when injected into the body's neutral pH tissue, it precipitates into microcrystals under the skin.
- These crystals slowly dissolve, releasing small amounts of insulin continuously over 24 hours - hence the "peakless" (flat, no spike) profile.
-
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Advantages Over Older Insulins (e.g., NPH)
| Feature | Glargine (SustaGlar) | NPH Insulin |
|---|---|---|
| Duration | ~24 hours | ~12-18 hours |
| Peak | Peakless (flat) | Has a peak (risk of night hypoglycemia) |
| Dosing frequency | Once daily | Usually twice daily |
| Hypoglycemia risk | Lower | Higher (due to peak) |
| Mixing | Cannot mix | Can mix with regular insulin |
-
- Textbook of Family Medicine, 9th Ed.; Lippincott Pharmacology
Side Effects and Precautions
| Side Effect | Details |
|---|---|
| Hypoglycemia (low blood sugar) | Most common and dangerous. Symptoms: shaking, sweating, dizziness, confusion. Treat with glucose immediately. |
| Injection site reactions | Redness, swelling, itching - usually mild |
| Lipodystrophy | Fat lumps or hollows at injection site from not rotating sites |
| Weight gain | Common with all insulins |
| Hypokalemia | Insulin drives potassium into cells; monitor in susceptible patients |
Important Warnings
- Do NOT mix with any other insulin in the same syringe (the acidic pH of glargine will alter the action of other insulins).
- Do NOT inject into a vein or muscle - subcutaneous only.
- Dose adjustments needed during illness, surgery, pregnancy, or changes in activity level.
- Monitor blood glucose regularly.
-
- Katzung's Basic and Clinical Pharmacology; Lippincott Pharmacology
Key Facts Summary
| Feature | Detail |
|---|---|
| Drug | Insulin Glargine 100 IU/mL |
| Brand | SustaGlar (Regenix) |
| Type | Long-acting basal insulin analog |
| Onset | 0.5-1 hour after injection |
| Duration | ~24 hours |
| Peak | None (peakless/flat profile) |
| Route | Subcutaneous injection only |
| Dose frequency | Once daily (same time each day) |
| Pen volume | 3 mL = 300 units |
| Storage (in use) | Room temperature, up to 28 days |
Important: Always use this medication exactly as prescribed by your doctor. Never adjust your dose without medical guidance. If you experience symptoms of low blood sugar (shakiness, cold sweat, confusion), take glucose immediately and inform your doctor.
This is a shared conversation. Sign in to Orris to start your own chat.