what is fev1 in simple terms
FEV1 stands for Forced Expiratory Volume in 1 second - it's the amount of air you can forcefully blow out of your lungs in the first second of a hard exhale.
Simple analogy: Imagine your lungs are a balloon. FEV1 measures how fast you can deflate it - specifically, how much air rushes out in just one second when you blow as hard as you can.
Why it matters:
- A healthy person can exhale about 75-80% of their total lung air in that first second
- If your airways are narrowed (like in asthma or COPD), less air gets out in that first second - so FEV1 is lower
- Doctors use it to detect and grade lung diseases, and to see if treatments are working
How it's measured: You breathe into a device called a spirometer - take the deepest breath possible, then blast air out as fast and hard as you can.
Normal vs. abnormal:
| Result | Meaning |
|---|---|
| FEV1 ≥ 80% of predicted | Normal |
| 70-79% | Mild reduction |
| 50-69% | Moderate reduction |
| < 50% | Severe reduction |
FEV1 is almost always looked at alongside FVC (total air you can exhale). The FEV1/FVC ratio tells doctors whether the problem is obstructive (blocked airways, like asthma) or restrictive (stiff lungs, like pulmonary fibrosis).
difference between obstructive and restrcutive diseases for 1 yr mbbs student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Here is a clean, 1st-year-friendly breakdown:
Obstructive vs Restrictive Lung Disease
The Core Idea (One Line Each)
| Core Problem | Air Movement | |
|---|---|---|
| Obstructive | Airways are narrowed/blocked | Air gets trapped IN - hard to breathe OUT |
| Restrictive | Lungs are stiff or compressed | Lungs can't expand - hard to breathe IN |
The Balloon Analogy
- Obstructive = Try blowing air out of a balloon through a narrow straw - air gets stuck inside
- Restrictive = Try inflating a balloon wrapped in tight cling wrap - it just won't expand
Spirometry Values (THE KEY TABLE)
| Value | Obstructive | Restrictive |
|---|---|---|
| FEV1 | ↓ (low) | ↓ (low) |
| FVC | Normal or slightly ↑ | ↓↓ (low) |
| FEV1/FVC ratio | ↓↓ LOW (< 70%) | Normal (both fall equally) |
| TLC (total lung capacity) | Normal or ↑ (air trapping) | ↓↓ (small lungs) |
Memory trick: In obstructive disease, the ratio breaks down because FEV1 drops more than FVC. In restrictive disease, everything shrinks proportionally, so the ratio stays normal. - Barash Clinical Anesthesia, p.1139
Why Does FEV1/FVC Differ?
Obstructive:
- Narrowed airways = air can't rush out fast
- FEV1 (speed-dependent) drops a lot
- FVC (total volume) is relatively preserved or even high (hyperinflation)
- Ratio = LOW
Restrictive:
- Lungs are small/stiff
- Both FEV1 and FVC drop by the same amount
- Ratio stays the same = NORMAL
- "A proportional decrease in all lung volumes" - Barash, p.1139
Common Diseases
| Obstructive | Restrictive |
|---|---|
| Asthma | Pulmonary fibrosis |
| COPD (emphysema + chronic bronchitis) | Sarcoidosis |
| Bronchiectasis | Pleural effusion |
| Cystic fibrosis | Obesity (compresses lungs) |
| Neuromuscular diseases (polio, myasthenia) |
Flow-Volume Loop (Diagrams you'll see in exams)
- Obstructive: The expiratory curve is scooped inward (concave) - air can't rush out
- Restrictive: The loop is smaller overall but normal shape - lungs just don't fill up
Reversibility - Key for Asthma vs COPD
- Asthma (obstructive): Reversible - FEV1 improves by >12% after a bronchodilator (salbutamol)
- COPD (obstructive): NOT fully reversible
- Restrictive: Bronchodilators don't help
Quick Exam Summary
FEV1/FVC < 0.7 → OBSTRUCTIVE (Airways blocked)
FEV1/FVC normal, FVC ↓ → RESTRICTIVE (Lungs small/stiff)
Both FEV1 and FVC are low in restrictive, but the ratio is what tells them apart - this is the single most tested concept in 1st-year respiratory physiology.
Why CO2 is used for, uh, identifying volume of dead space in single breath CO2 technique.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Great - got everything needed from the textbook. Here's the full explanation:
Why CO2 is Used in the Single-Breath Technique for Dead Space
The Key Reason - In One Sentence
Room air has virtually zero CO2, but alveolar air is rich in CO2 - so CO2 naturally acts as a perfect "tracer" that labels alveolar air and is completely absent from dead space air, with no special setup needed.
What is Dead Space (Quick Recap)?
Dead space = the part of your airway where no gas exchange happens - the nose, trachea, bronchi (conducting airways). Air sitting here never touches blood, so it contributes nothing useful.
- Anatomical dead space ~150 mL - the conducting airways
- Physiological dead space - anatomical + any alveoli that are ventilated but not perfused
Why CO2 Works So Well
| Location | CO2 content |
|---|---|
| Room air (inhaled) | ~0 mmHg (essentially zero) |
| Dead space (conducting airways) | ~0 mmHg - just inhaled room air sitting there |
| Alveolar air | ~40 mmHg - CO2 continuously diffuses in from venous blood |
So when you exhale, the first air out = pure dead-space air = zero CO2, and the later air out = alveolar air = CO2 rises to ~40 mmHg. The transition between them is sharp and measurable.
As Medical Physiology (Boron & Boulpaep) puts it:
"Room air has practically no CO2. Yet plenty of CO2 is in the alveoli, where it evolves from the incoming mixed-venous blood."
The Single-Breath CO2 Technique - Step by Step
- Patient breathes out fully, then inhales one normal tidal breath (~500 mL) of room air
- The first ~350 mL goes into the alveoli and dilutes the CO2 there
- The remaining ~150 mL stays in the conducting airways (PCO2 = 0)
- Patient now exhales - a CO2 probe records continuously:
Phase I: PCO2 = 0 → Pure dead-space air (conducting airways)
Phase II: PCO2 rises fast → Mixture of dead-space + alveolar air
Phase III: PCO2 plateau ~40 → Pure alveolar air (end-tidal CO2)
The volume at the transition point = anatomical dead space (VD)
This diagram from the textbook (Fowler technique with N2, same principle with CO2) shows exactly this:
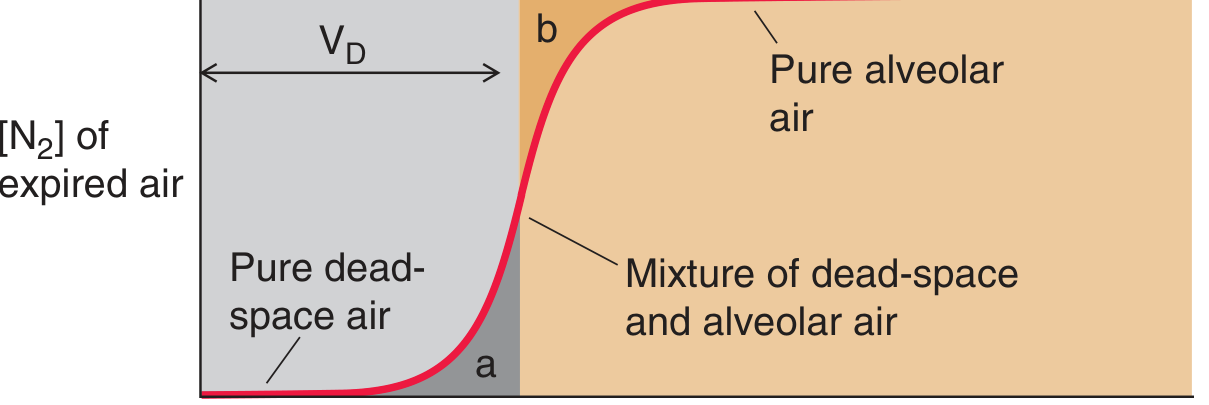
The grey zone = pure dead-space air (zero gas marker), tan zone = pure alveolar air (high gas marker), and VD is measured at the inflection point.
Why NOT other gases?
- N2 (Fowler's original method): Also works, but you need to first make the patient inhale 100% O2 to wash nitrogen out - an extra artificial step
- CO2 is easier: No special gas needed - room air already has near-zero CO2, and the body naturally loads alveolar air with CO2 from venous blood
"Nitrogen is useful because we can easily create an artificial situation...Another possibility is CO2. Its profile during expiration is similar to that of N2. Moreover, we do not need to use any special tricks to get it to work because room air has practically no CO2." - Medical Physiology, Boron & Boulpaep
The Bohr Equation (Bonus - Physiological Dead Space)
Christian Bohr (father of physicist Niels Bohr!) used CO2 to calculate physiological dead space:
$$V_D = V_E \times \frac{P_{A}CO_2 - P_{\bar{E}}CO_2}{P_{A}CO_2}$$
- VD = dead space volume
- VE = total expired volume
- PACO2 = alveolar CO2 (≈ arterial CO2, ~40 mmHg)
- P̄ECO2 = mixed-expired CO2 (averaged over whole breath)
The logic: Dead space air contributes zero CO2 to the exhaled mix. So the more dead space you have, the more diluted the mixed-expired CO2 is. The dilution tells you exactly how much dead space there is.
Summary
CO2 is ideal because:
- Zero in inhaled air - no background noise
- Naturally high in alveoli - the body loads it automatically
- No special setup needed - unlike N2 washout which needs a 100% O2 breath
- Measurable in real time - with a capnograph/CO2 probe at the mouth
I need an simple explanation, uh, how CO2 is helpful here.
Here's the simplest way to think about it:
CO2 as a "Stamp" on Alveolar Air
Think of CO2 like a ink stamp that the body puts on air - but only after it reaches the alveoli and touches blood.
- Air sitting in the dead space (trachea, bronchi)? No stamp - it never touched blood, so CO2 = 0
- Air that reached the alveoli? Stamped - blood loaded it with CO2 ~40 mmHg
What Happens When You Exhale
You breathe out slowly. A CO2 sensor sits at your mouth and watches:
First air out → CO2 = 0 "This is dead space air - unstamped"
...
Later air out → CO2 = 40 "This is alveolar air - stamped"
The exact moment CO2 jumps from zero to 40 tells you: "dead space just ended, alveoli just started."
Measure the volume exhaled up to that point = your dead space volume.
Why CO2 Specifically?
Because it gives you a natural, built-in contrast:
| CO2 | |
|---|---|
| Room air you inhaled | ~0 (essentially none) |
| Dead space air | ~0 (just the room air sitting there) |
| Alveolar air | ~40 mmHg (loaded by venous blood) |
The jump from 0 → 40 is sharp and easy to detect. CO2 does this automatically - the body produces it constantly in the blood and it diffuses into the alveoli on its own. No special gas or preparation needed.
One line summary: CO2 = 0 in dead space, CO2 = 40 in alveoli. You just watch where the switch happens - that's your dead space.
How does the Bohr equation use CO2 to calculate dead space?
The Bohr equation works on one simple idea: dead space air has zero CO2, so any "dilution" of CO2 in your exhaled breath must be caused by dead space air mixing in.
The Core Logic - Dilution Thinking
Imagine you have a glass of juice (alveolar air, rich in CO2). You add plain water to it (dead space air, zero CO2). The final drink is watered down.
The more water you added, the more diluted the juice is.
The Bohr equation just works backwards from how diluted the CO2 is, to figure out how much "water" (dead space) was added.
Breaking Down the Equation
$$V_D = V_T \times \frac{P_ACO_2 - P_{\bar{E}}CO_2}{P_ACO_2}$$
Let's name each part in plain English:
| Symbol | What it is | Typical value |
|---|---|---|
| VD | Dead space volume (what we want) | ~150 mL |
| VT | Total tidal volume (one breath) | ~500 mL |
| PACO2 | CO2 in alveolar air ("pure juice") | ~40 mmHg |
| P̄ECO2 | CO2 in ALL exhaled air mixed together ("diluted juice") | ~28 mmHg |
The Fraction Part - What it Actually Means
$$\frac{P_ACO_2 - P_{\bar{E}}CO_2}{P_ACO_2}$$
- The top = how much CO2 was "lost" due to dilution
- The bottom = what the CO2 should have been if there was no dead space
- The fraction = what proportion of your breath was dead space
Example with numbers:
- PACO2 = 40, P̄ECO2 = 28
- Fraction = (40 - 28) / 40 = 12/40 = 0.3
- VD = 500 × 0.3 = 150 mL of dead space
Why Does Dead Space Dilute CO2?
When you exhale a full breath (500 mL total):
- ~350 mL comes from alveoli → carries CO2 ~40 mmHg
- ~150 mL comes from dead space → carries CO2 = 0
When these mix together in the exhaled air, the average CO2 drops below 40. The bigger the dead space, the more the CO2 gets diluted, the lower P̄ECO2 becomes.
One-Line Intuition
"If exhaled CO2 is lower than alveolar CO2, something with zero CO2 diluted it - that's your dead space."
The equation just quantifies exactly how much of your breath had to be zero-CO2 air to cause that exact drop.
This is a shared conversation. Sign in to Orris to start your own chat.