Can cbc,fbs,serum creatinine,serum electrolytes,pt-inr levels all be normal in case of erosive gastritis caused by h pylori in patient who is alcoholic
can CBC serum creatinine electrolytes PT-INR be normal in H pylori erosive gastritis alcoholic patient
Can CBC, FBS, Serum Creatinine, Serum Electrolytes, and PT-INR All Be Normal in H. pylori Erosive Gastritis in an Alcoholic?
The Short Answer First
Why Each Lab Can Be Normal
1. CBC (Complete Blood Count)
- In early or mild erosive gastritis, bleeding is superficial (petechial erosions, not deep ulcers). Blood loss is minimal or occult, so haemoglobin, haematocrit, and RBC indices can be normal.
- Even H. pylori-positive patients with endoscopic gastritis commonly show normal CBC. Studies measuring NLR (neutrophil-to-lymphocyte ratio) and PLR as inflammatory markers in H. pylori gastritis found that standard CBC values (Hb, MCV, platelet count) can lie well within normal limits when the disease is mild to moderate.
- An alcoholic who is still well-nourished and not drinking at cirrhotic levels will not yet have the macrocytosis, thrombocytopenia, or anaemia typical of advanced liver disease.
- Caveat: If there is chronic occult blood loss, iron deficiency anaemia may eventually develop. But this is not guaranteed in early disease.
2. FBS (Fasting Blood Sugar)
- Erosive gastritis has no direct effect on glucose metabolism.
- An alcoholic may have hypoglycaemia (acute binge) or insulin resistance (chronic heavy use), but FBS can be normal in a social or moderate drinker.
- H. pylori itself does not cause dysglycaemia.
3. Serum Creatinine
- Gastritis is a luminal/mucosal condition. It does not damage nephrons.
- Serum creatinine reflects GFR, which is unaffected by gastric mucosal inflammation.
- In an alcoholic without hepatorenal syndrome or dehydration, creatinine is normal.
- Caveat: Severe vomiting from gastritis could cause volume depletion and a transient pre-renal rise, but this resolves quickly and is not a fixed finding.
4. Serum Electrolytes
- Mild erosive gastritis produces no electrolyte shifts.
- Electrolytes are disturbed only when there is persistent vomiting (hypokalaemia, metabolic alkalosis, hypochloraemia) or severe diarrhoea - neither of which is a defining feature of simple erosive gastritis.
- In an alcoholic with intact nutrition and hydration, electrolytes are typically normal.
- Caveat: Chronic heavy alcohol use can cause hypomagnesaemia and hypophosphataemia independently of gastritis, but these are not caused by the gastritis itself.
5. PT-INR
- PT-INR reflects hepatic synthetic function (factors II, VII, IX, X) and vitamin K status.
- The liver manufactures clotting factors. Erosive gastritis does not impair the liver.
- PT-INR is abnormal in: cirrhosis, acute hepatitis, vitamin K deficiency (from malabsorption or poor intake), or anticoagulant use.
- An alcoholic with early or compensated liver disease - or one who drinks but has not yet developed hepatic dysfunction - will have a normal PT-INR.
- Caveat: If the patient has alcoholic hepatitis or cirrhosis alongside the gastritis, PT-INR will be elevated. But H. pylori erosive gastritis alone does not prolong clotting time.
What IS Abnormal in H. pylori Erosive Gastritis?
| Finding | Why it Changes |
|---|---|
| Endoscopy | Erythema, erosions, mucosal friability, "mamillated" corpus appearance |
| Gastric biopsy histology | Lymphoplasmacytic infiltrate, neutrophils in epithelium, H. pylori organisms in mucus layer |
| H. pylori serology / urea breath test / stool antigen | Direct evidence of infection |
| Faecal occult blood | May be positive from microscopic erosion bleeding |
| Serum ferritin / iron | May be low-normal or mildly reduced in chronic low-grade blood loss |
| CRP / ESR | Mildly elevated in active infection, but often within normal limits in localised mucosal disease |
Clinical Takeaway
- Endoscopy is the gold standard for diagnosing erosive gastritis - not blood tests.
- H. pylori testing (urea breath test, stool antigen, or biopsy urease test) should be done regardless of CBC/chemistry results.
- Blood tests only become abnormal when complications supervene: significant GI bleeding (drops Hb), cirrhosis (raises PT-INR, drops platelets), dehydration from vomiting (raises creatinine, drops Na/K), or severe malnutrition (drops albumin, prolongs PT).
Goals of therapy and non pharmacological treatment for erosive gastritis
goals of therapy non pharmacological management erosive gastritis H pylori alcohol lifestyle
erosive gastritis goals of therapy symptom relief mucosal healing prevent complications guidelines 2024
https://www.merckmanuals.com/professional/gastrointestinal-d…
Goals of Therapy and Non-Pharmacological Treatment for Erosive Gastritis
Goals of Therapy
1. Remove / Eliminate the Causative Agent
- Discontinue NSAIDs, aspirin, or corticosteroids when possible
- Stop or significantly reduce alcohol intake
- Eradicate H. pylori if confirmed (this reduces active mucosal inflammation and prevents progression)
- Treat the underlying critical illness if stress-related
2. Relieve Symptoms
- Resolve dyspepsia, epigastric pain, nausea, and vomiting
- Improve quality of life
3. Mucosal Healing
- Achieve endoscopic resolution of erosions
- Restore mucosal integrity and barrier function
- Acid suppression (PPIs, H2RAs) is the mainstay pharmacological approach here - less luminal acid = less ongoing mucosal injury and faster re-epithelialization
4. Control Active Bleeding
- In patients presenting with haematemesis or melena: haemodynamic stabilisation, endoscopic haemostasis, surgical backup if needed
- This is a separate acute management goal when the disease is complicated
5. Prevent Complications
- Prevent progression to peptic ulcer disease
- Prevent significant upper GI bleeding
- In H. pylori-related disease specifically: prevent gastric atrophy, intestinal metaplasia, dysplasia, and gastric adenocarcinoma (the long-term stakes of untreated infection)
6. Prevent Recurrence
- Avoid recurrence after healing, especially if the patient cannot permanently stop the offending agent (e.g., patient requires long-term NSAIDs for arthritis)
Non-Pharmacological Treatment
1. Alcohol Cessation or Strict Reduction
- Alcohol directly disrupts the gastric mucosal barrier by dissolving the protective mucous layer, increasing mucosal permeability, and stimulating acid secretion
- Continued alcohol use prevents mucosal healing even with adequate pharmacological therapy
- Alcohol also impairs H. pylori eradication - higher daily alcohol consumption is independently associated with eradication failure, likely through effects on antibiotic pharmacokinetics and gut flora
- Goal: complete cessation during the active treatment phase; long-term reduction to reduce recurrence risk
- Alcohol cessation counselling, motivational interviewing, and referral to addiction services (if applicable) are part of management
2. NSAID / Aspirin Avoidance
- Stop NSAIDs if clinically feasible. If pain management requires continuation, switch to a COX-2 selective inhibitor (lower GI risk), or ensure co-prescription of a PPI
- Avoid over-the-counter NSAID self-medication
3. Smoking Cessation
- Smoking impairs gastric mucosal blood flow, reduces bicarbonate secretion, increases acid secretion, and delays mucosal healing
- It is also a co-factor in H. pylori-related gastric cancer progression
- Smoking cessation counselling should be offered
4. Dietary Modifications
| What to Avoid | Reason |
|---|---|
| Spicy foods, chilli | Direct mucosal irritant in susceptible patients |
| Highly salted, pickled, smoked foods | High salt alters gastric epithelial cells, promotes H. pylori pathogenicity, associated with gastric cancer |
| Fatty / fried foods | Delay gastric emptying, worsen symptoms |
| Citrus juices, carbonated drinks | Increase acid load, irritate inflamed mucosa |
| Coffee and caffeine | Stimulate acid secretion |
| Alcohol (reiterated) | Direct mucosal toxin |
| What to Favour | Reason |
|---|---|
| Small, frequent meals | Reduce distension, buffer acid, less parietal cell stimulation at any one time |
| Well-cooked, soft, easily digestible foods | Less mechanical irritation |
| Adequate hydration | Supports mucosal repair |
| Probiotic-containing foods (yoghurt, kefir) | Some evidence for improved H. pylori eradication rates and reduction of antibiotic side effects when used as adjuncts |
| Cruciferous vegetables (broccoli, cabbage) | Contain sulforaphane with in vitro anti-H. pylori activity |
5. Stress Reduction and Sleep Hygiene
- Psychological stress aggravates gastric symptoms and may impair mucosal repair through neuroendocrine pathways
- Adequate sleep, regular exercise, and relaxation techniques (mindfulness, yoga) are reasonable adjuncts
- These measures do not directly heal erosions but improve overall recovery trajectory and symptom perception
6. H. pylori Hygiene (Prevention of Reinfection)
- H. pylori spreads via the faecal-oral and oral-oral routes
- Good hand hygiene (before meals, after toilet), use of clean water, and avoiding sharing utensils are relevant especially in endemic settings
- In an alcoholic patient with poor self-care, counselling on hygiene is appropriate
7. Food Safety and Hygiene
- Avoid potentially contaminated food and water sources (H. pylori infection risk)
8. Enteral Nutrition (in ICU / Stress Gastritis Context)
- Early enteral nutrition in critically ill patients has been shown to reduce the risk of stress ulceration by maintaining mucosal integrity, supporting blood flow, and improving the gut mucosal barrier
- This is a well-established non-pharmacological measure in the ICU setting
Summary Table
| Goal | Non-Pharmacological Approach |
|---|---|
| Remove causative agent | Stop alcohol, stop NSAIDs, quit smoking |
| Mucosal healing | Diet modification, small frequent meals, avoid irritants |
| Eradicate H. pylori (support) | Alcohol cessation (improves eradication rates), good hygiene |
| Prevent complications | Long-term lifestyle changes, surveillance endoscopy if indicated |
| Prevent cancer progression | H. pylori eradication + smoking cessation + low-salt diet |
| Symptom control | Dietary adjustments, stress reduction |
Patient counselling for erosive gastritis
patient counselling points erosive gastritis H pylori alcohol medication adherence warning signs
https://www.ncbi.nlm.nih.gov/books/NBK544250
Patient Counselling for Erosive Gastritis
1. Explain the Condition (What Is It?)
"Your stomach has a protective lining. This lining has been damaged and has developed small sores or erosions. This is causing your pain, nausea, and discomfort. The good news is this can heal with the right treatment and lifestyle changes."
- The stomach normally makes acid to digest food. When the protective lining is weakened - by alcohol, bacteria (H. pylori), or painkillers - acid attacks the stomach wall itself
- Erosive gastritis is treatable, but only if the underlying cause is addressed
- If left untreated, it can progress to deeper ulcers, bleeding, or in the long term, increase the risk of stomach cancer (especially with untreated H. pylori)
2. Explain the Cause (Why Did This Happen?)
| Cause | Counselling Point |
|---|---|
| H. pylori infection | "You have a bacterial infection in your stomach. It is common and very treatable with a course of antibiotics. Without treating it, the infection will continue damaging your stomach lining." |
| Alcohol | "Alcohol directly burns and strips away your stomach's protective lining. Even moderate alcohol use will slow healing. Heavy use makes this condition much worse." |
| NSAIDs (e.g., ibuprofen, aspirin, diclofenac) | "These painkillers reduce the natural protection your stomach has. They are a common cause of erosions." |
| Smoking | "Smoking reduces blood flow to the stomach, weakens its defences, and slows healing." |
| Stress | "Severe physical or emotional stress can worsen the condition." |
3. Medication Counselling
a) For H. pylori Eradication (if applicable)
- Complete the full course - typically 10 to 14 days of combination therapy (two antibiotics + a PPI). Stopping early is the single biggest cause of treatment failure
- Take medicines on time, every day - set phone alarms if needed. Missing doses allows bacteria to survive and develop antibiotic resistance
- Take PPI 30-60 minutes before food for maximum acid suppression. This improves antibiotic effectiveness
- Take antibiotics with or after food to reduce nausea and metallic taste
- Avoid alcohol completely during the antibiotic course - alcohol interacts with metronidazole (causes severe flushing, nausea, vomiting) and reduces eradication success rates
- Do not stop medicines just because you feel better - feeling better does not mean the bacteria are gone
- Side effects to expect: metallic taste, mild nausea, loose stools, headache - these are common and usually manageable. Severe or persistent diarrhoea should be reported
b) For Acid Suppressants (PPI / H2RA)
- Take the PPI (e.g., omeprazole, pantoprazole) 30 minutes before your first meal each day
- Do not take antacids and PPIs simultaneously without guidance - they can interfere
- Do not stop PPIs abruptly once healed without consulting your doctor - rebound acid secretion can occur
- Long-term PPI use without indication is not recommended; your doctor will advise when to stop
c) Antacids (if prescribed for symptom relief)
- Use for immediate symptom relief (burning, discomfort), not as a replacement for prescribed medicines
- Do not use antacids as a substitute for following treatment
4. Alcohol Counselling (Priority Point in Alcoholic Patients)
- "Alcohol is one of the direct causes of your stomach erosions. Continuing to drink will prevent healing, no matter how well you take your medicines."
- Complete cessation is the goal during the treatment phase (minimum 4-6 weeks, ideally permanent reduction)
- Higher alcohol intake is independently linked to failure of H. pylori eradication - the bacteria survive treatment in heavy drinkers at significantly higher rates
- Chronic alcohol use also causes liver disease, which in turn leads to its own complications (varices, coagulopathy, portal hypertensive gastropathy) - the stomach problem is a warning sign of bigger risk
- Offer signposting to alcohol support services, counselling, or de-addiction programmes if appropriate
- Use non-judgmental language: "I understand stopping is not easy. Even reducing your intake significantly will help your stomach heal faster."
5. Dietary Advice
- Alcohol (any form)
- NSAIDs and aspirin (over-the-counter painkillers) - use paracetamol for pain instead
- Spicy, highly salted, pickled, and smoked foods
- Fatty and fried foods
- Caffeine (coffee, strong tea, energy drinks) - stimulates acid
- Carbonated drinks
- Citrus juices (orange, lemon) - irritate inflamed mucosa
- Large heavy meals
- Small, frequent meals (4-6 small meals rather than 2-3 large ones) - reduces acid peaks
- Bland, easily digestible foods during the healing phase
- Adequate water intake
- Yoghurt and fermented foods (probiotics) - may reduce side effects of antibiotics and support gut recovery
- Cooked vegetables, soft foods, lean proteins
6. Lifestyle Modifications
- Stop smoking - smoking impairs mucosal healing, increases acid, and is a co-factor in progression to gastric cancer with H. pylori
- Stress management - adequate sleep, regular gentle exercise, relaxation techniques (deep breathing, yoga, mindfulness). Stress does not cause gastritis directly but worsens symptoms and impairs recovery
- Avoid NSAIDs - for any pain or fever, use paracetamol (acetaminophen) instead. If you must take NSAIDs for a medical reason, always inform your doctor so protective medicines can be co-prescribed
- Maintain good hand hygiene - H. pylori spreads via the faecal-oral route. Wash hands before eating and after using the toilet
- Do not share utensils or food - particularly relevant in households where H. pylori infection is suspected
7. Warning Signs - When to Return Immediately
| Warning Sign | What It May Mean |
|---|---|
| Vomiting blood (bright red or dark "coffee-ground" vomit) | Active upper GI bleeding - emergency |
| Black, tarry, foul-smelling stools (melena) | Digested blood in stools - GI bleeding |
| Severe or worsening abdominal pain | Ulcer perforation or significant worsening |
| Dizziness, fainting, rapid heartbeat | Significant blood loss |
| Unexplained weight loss | Possible malignancy |
| Persistent vomiting | Obstruction or severe disease |
| Difficulty swallowing | Alarm symptom - needs urgent evaluation |
| Pale skin, breathlessness, extreme tiredness | Anaemia from ongoing bleeding |
8. Confirm Eradication (H. pylori Specific)
- After completing the antibiotic course, a test of cure is mandatory
- The recommended tests are the urea breath test or the stool antigen test - performed at least 4 weeks after finishing antibiotics and 2 weeks after stopping the PPI
- Serology (blood antibody test) should NOT be used to confirm eradication - antibodies persist in blood for months to years after the infection is gone, giving a false positive
- If eradication fails: a second-line course is needed. Failure after two attempts requires H. pylori culture and sensitivity testing
- Convey clearly: "The test after treatment is not optional - it is the only way to know the infection is gone. Feeling better does not confirm cure."
9. Follow-Up and Surveillance
- Return for a scheduled review 4-8 weeks after completing treatment
- If erosive gastritis was confirmed on endoscopy, a follow-up endoscopy may be scheduled to confirm mucosal healing - comply with this appointment
- Patients who develop atrophic gastritis (a possible progression in long-standing H. pylori disease) require surveillance endoscopy every 3 years given the increased gastric cancer risk - Schwartz's Principles of Surgery states: "Patients stratified as stage 3 or 4 gastritis and those with pernicious anemia may benefit from surveillance endoscopy every 3 years"
- Report any new or returning symptoms promptly
10. Psychosocial and Motivational Points
- Reinforce that this condition is reversible with adherence to treatment and lifestyle change
- Acknowledge that stopping alcohol is hard and offer empathy, not blame
- Involve family members (with patient consent) to provide a support system for dietary and alcohol changes
- Emphasise "test of cure" as a positive milestone to work toward - frame it as proof of recovery
- Remind the patient that untreated H. pylori + ongoing alcohol use is a combination that significantly raises gastric cancer risk long-term - this is a motivational reason to act now
Summary Card for Patient (Simplified Take-Home Points)
✔ Take ALL your medicines for the full course - don't stop when you feel better ✔ Avoid alcohol completely while on treatment (and reduce long-term) ✔ Stop NSAIDs/ibuprofen - use paracetamol instead ✔ Eat small, frequent, bland meals ✔ Come back for your "test of cure" 4 weeks after finishing antibiotics ✔ Return immediately if you vomit blood, pass black stools, or feel faint ✔ Quit smoking ✔ Keep your follow-up appointment
Pathophysiology of erosive gastritis by h.pylori in flowchart it should be small
A clean, compact vertical flowchart titled "Pathophysiology of Erosive Gastritis by H. pylori" with the following sequential steps connected by downward arrows, on a white background with minimal design: 1. Box: "H. pylori colonizes gastric mucosa (antrum)" 2. Arrow down 3. Box: "Produces urease → NH3 (ammonia) + CO2 — neutralizes local acid, enables survival" 4. Arrow down 5. Box: "Virulence factors released: CagA, VacA toxins — disrupt epithelial tight junctions" 6. Arrow down 7. Box: "Direct epithelial cell damage + increased mucosal permeability" 8. Arrow down 9. Box: "Triggers host immune response — neutrophils & macrophages recruited" 10. Arrow down 11. Box: "Pro-inflammatory cytokines released (IL-1β, IL-6, IL-8, TNF-α)" 12. Arrow down 13. Box: "Chronic mucosal inflammation — damages surface epithelium" 14. Arrow down 15. Box: "↑ Gastric acid secretion (gastrin ↑, somatostatin ↓) — worsens mucosal injury" 16. Arrow down 17. Box: "Mucosal barrier disruption — mucus layer depleted, bicarbonate secretion ↓" 18. Arrow down 19. Box (red/pink highlight): "EROSIVE GASTRITIS — superficial mucosal erosions, bleeding, pain" Style: professional medical diagram, compact, clear sans-serif font, light blue boxes with dark text, bold red final box, clean white background, no extra decorations
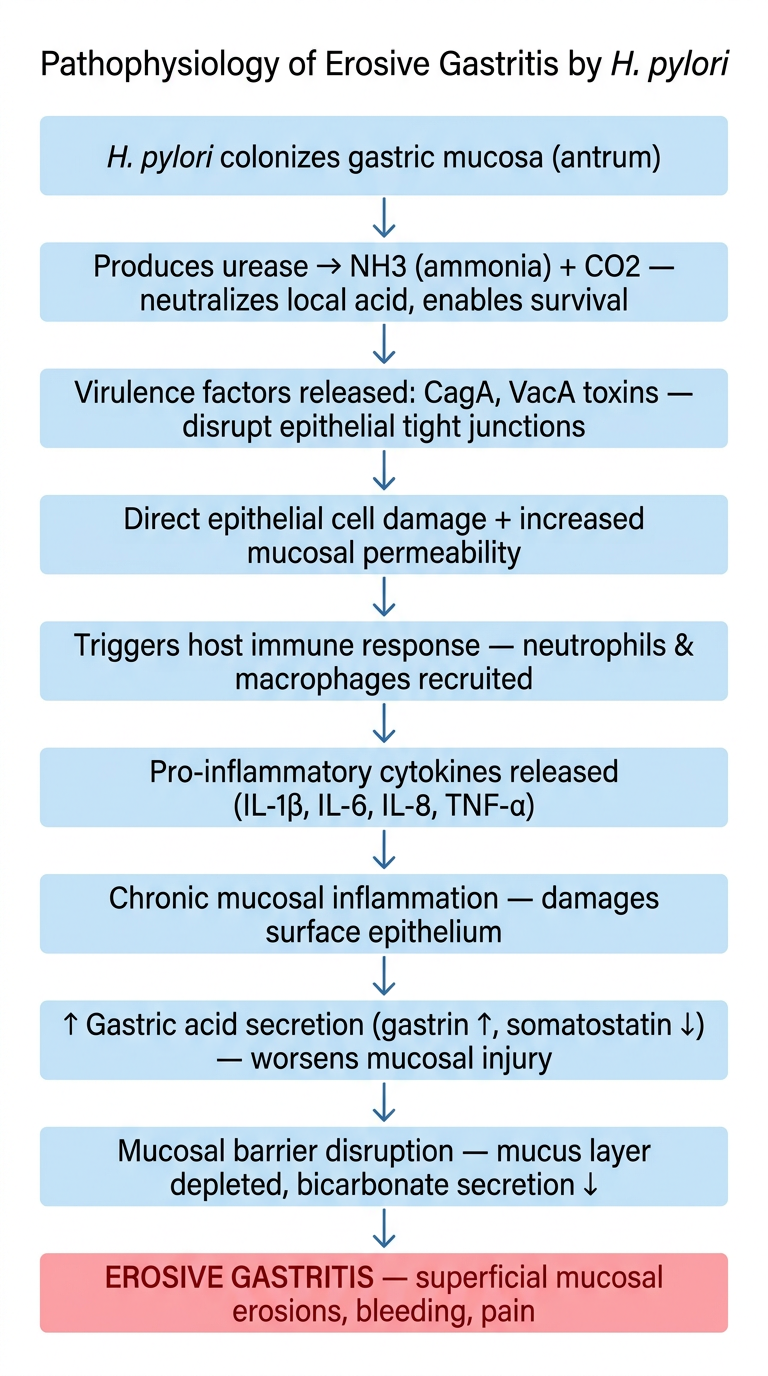
- H. pylori colonises the gastric antrum - survives the acidic environment using urease to generate ammonia
- Virulence factors (CagA, VacA) - directly damage epithelial cells and disrupt tight junctions
- Host immune activation - neutrophils, macrophages, and pro-inflammatory cytokines (IL-1β, IL-8, TNF-α) are recruited
- Chronic mucosal inflammation - ongoing epithelial injury
- Hormonal imbalance - gastrin rises, somatostatin falls → increased acid secretion
- Mucosal barrier failure - mucus layer depleted, bicarbonate secretion reduced
- End result: Erosive Gastritis - superficial erosions, bleeding potential, pain