Facial nerve 5m answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive material for a thorough 5-mark answer. Let me compile it:
Facial Nerve (VII) - 5 Mark Answer
Introduction
The facial nerve is the 7th cranial nerve (CN VII). It is a mixed nerve innervating structures derived from the second branchial arch (Reichert's cartilage). It has three nuclei of origin in the brainstem:
- Motor nucleus - in the caudal pons (special visceral efferents)
- Superior salivatory nucleus - dorsal to motor nucleus (general visceral efferents)
- Nucleus of the solitary tract - in the medulla oblongata (taste/sensory)
Note: The superior portion of the motor nucleus (for frontalis and orbicularis oculi) receives bilateral (crossed + uncrossed) cortical input - this is the anatomical basis for sparing of forehead movements in upper motor neuron (UMN) facial palsy. The inferior portion receives only ipsilateral input, so it is affected in both UMN and LMN lesions.
Fiber Components (5 types)
| Fiber Type | Function |
|---|---|
| Special visceral efferent (SVE) | Muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric |
| General visceral efferent (GVE) | Lacrimal gland (via GSPN + pterygopalatine ganglion); submandibular & sublingual glands (via chorda tympani + submandibular ganglion) |
| Special sensory (taste) | Anterior 2/3 of tongue (via chorda tympani); tonsillar fossae and palate (via GSPN); cell bodies in geniculate ganglion |
| General somatic afferent | Skin of EAC and concha; proprioception from facial muscles |
| Visceral afferent | Mucosa of nose, pharynx, and palate |
Course and Segments
The facial nerve travels through the fallopian canal in the temporal bone, which begins at the fundus of the IAC and ends at the stylomastoid foramen. Five segments are recognized:
1. Intracranial (Cisternal) Segment - 24 mm
- Emerges from the brainstem between the pons and the olive
- Crosses the cerebellopontine angle (CPA) alongside CN VIII
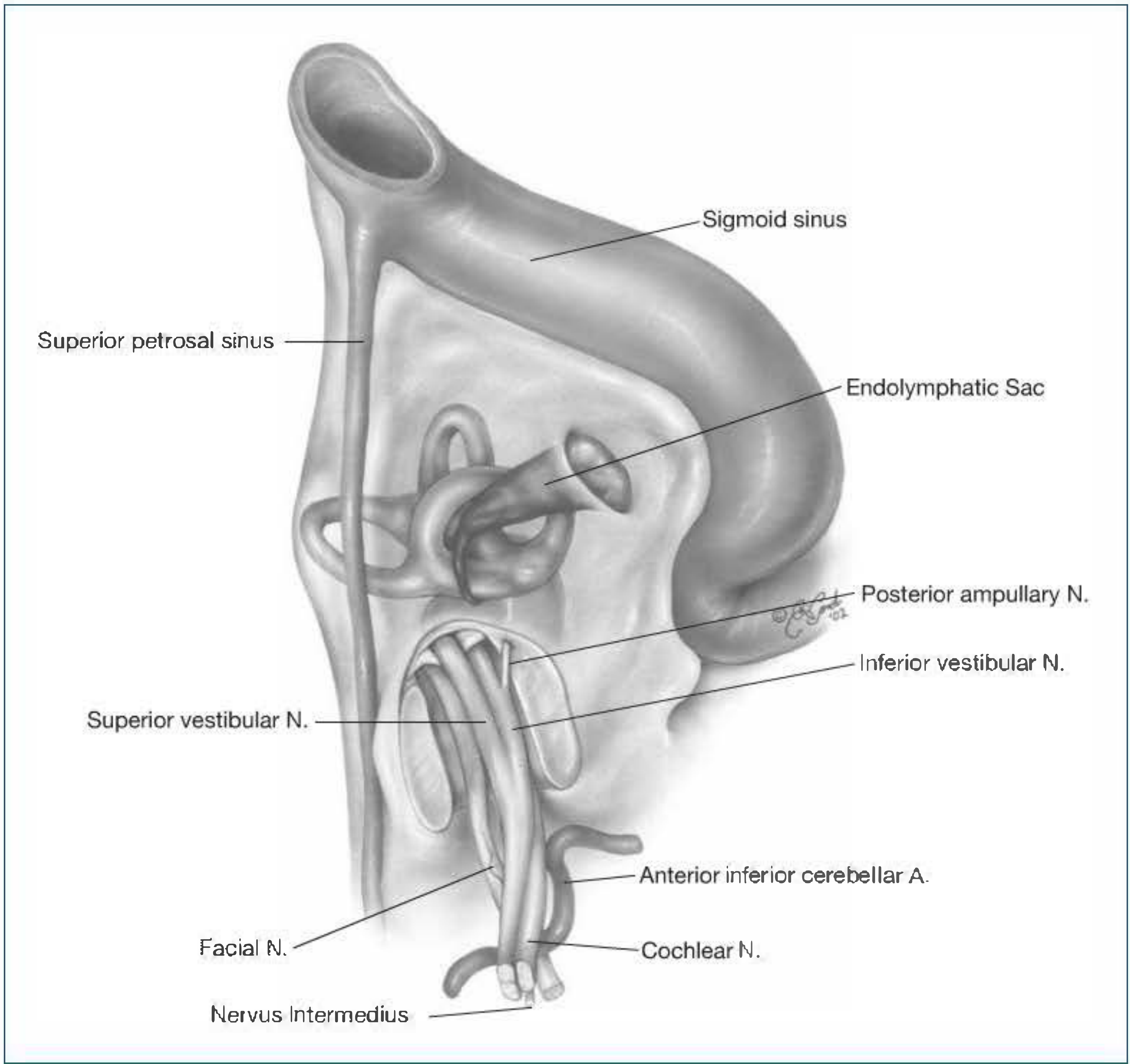
- Enters the internal auditory meatus (IAM) - lies anterosuperiorly in the IAC, above the cochlear nerve (superior and inferior vestibular nerves are posterior)
- The nervus intermedius (nerve of Wrisberg) runs as a separate nerve between facial and superior vestibular nerves in the IAC
2. Intracanalicular (Meatal) Segment
- Traverses the IAC; at the fundus, occupies the anterosuperior quadrant (separated from superior vestibular nerve by the vertical crest / Bill's bar)
- Joined here by the nervus intermedius
3. Labyrinthine Segment - 4 mm (shortest, narrowest)
- Runs from the beginning of the fallopian canal to the geniculate ganglion
- Courses superior to the cochlea, between cochlea and vestibule
- Most vulnerable to compression: no epineurium, watershed blood supply (vertebrobasilar + external carotid systems)
- At the geniculate ganglion (1st genu): the nerve makes an acute posterior turn
- Gives off the greater superficial petrosal nerve (GSPN) - runs in a groove along the middle cranial fossa floor
4. Tympanic (Horizontal) Segment - 13 mm
- Courses in the medial wall of the middle ear (anterior attic), superior to the cochleariform process and oval window
- Ends at the 2nd genu - turns inferiorly just anteroinferior to the lateral semicircular canal
- Most common site of congenital bony dehiscence (especially above the oval window, present in ~25% of ears; bilateral in ~75% of cases)
- Gives off the nerve to stapedius at the pyramidal eminence
5. Mastoid (Vertical) Segment - 20 mm
- Descends from 2nd genu to stylomastoid foramen
- Gives off chorda tympani nerve (~4 mm proximal to stylomastoid foramen)
- Chorda tympani ascends in a canal lateral and anterior to CN VII, enters tympanic cavity at iter chordae posterius, crosses lateral to long process of incus and medial to malleus, exits at iter chordae anterius (canal of Huguier) through the petrotympanic (Glaserian) fissure
- The facial recess (triangular area used in intact-canal-wall mastoidectomy) is bounded by: incudal fossa (superior), facial nerve (medial), chorda tympani (lateral)
Extracranial Course
On exiting the stylomastoid foramen, the nerve gives off:
- Posterior auricular nerve - occipital belly of occipitofrontalis, auricular muscles
- Branch to posterior belly of digastric and stylohyoid
The nerve then enters the parotid gland, divides into upper and lower trunks, and gives five terminal branches via the parotid plexus (pes anserinus):
| Branch | Muscles Innervated |
|---|---|
| Temporal | Frontalis, orbicularis oculi (superior), corrugator supercilii |
| Zygomatic | Orbicularis oculi (inferior), zygomaticus |
| Buccal | Buccinator, muscles of nose and upper lip |
| Marginal mandibular | Depressors of lower lip, mentalis |
| Cervical | Platysma |
Mnemonic: "To Zanzibar By Motor Car" (Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical)
Intratemporal Branches (3)
- Greater superficial petrosal nerve (GSPN) - from geniculate ganglion; preganglionic parasympathetic to lacrimal gland and nasal/palatal glands via pterygopalatine ganglion; also taste from palate
- Nerve to stapedius - from mastoid segment near pyramidal eminence; lesion above this level causes hyperacusis
- Chorda tympani - from mastoid segment; taste from anterior 2/3 tongue + preganglionic parasympathetic to submandibular and sublingual glands via submandibular ganglion
Clinical Significance
Localization of Lesions (by lost function)
| Level of Lesion | Features Lost |
|---|---|
| Brainstem (UMN) | Contralateral lower face palsy; forehead spared (bilateral cortical supply) |
| CPA/IAC | Facial palsy + deafness + vestibular symptoms |
| Geniculate ganglion | All ipsilateral (palsy + loss of lacrimation + hyperacusis + loss of taste anterior 2/3 tongue) |
| Above nerve to stapedius | Palsy + hyperacusis + loss of taste |
| Above chorda tympani | Palsy + loss of taste (no hyperacusis) |
| At/below stylomastoid foramen | Pure motor palsy only |
Bell Palsy
- Most common cause of acute unilateral LMN facial paralysis (idiopathic; likely viral - HSV reactivation)
- Complete paralysis of all ipsilateral facial muscles including forehead
- Managed with oral corticosteroids (and antivirals in severe cases)
- Graded using House-Brackmann (HB) grading system (I = normal, VI = complete paralysis)
Ramsay Hunt Syndrome
- Herpes zoster reactivation in the geniculate ganglion
- Triad: LMN facial palsy + vesicles in EAC/pinna + ipsilateral sensorineural hearing loss
Fallopian Canal Dehiscence
- Most common over the oval window (tympanic segment); present in 25% of ears; 75% bilateral
- Renders the nerve vulnerable to suppurative otitis media and surgical injury
Sources: Shambaugh Surgery of the Ear; Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.