Describe about decubitus ulcer
Reading File
Finding Sources
Searching PubMed
"pressure ulcer" OR "decubitus ulcer" prevention management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have all the information needed for a thorough response. Let me now compile the full answer.
Decubitus Ulcer (Pressure Ulcer / Bedsore)
Definition and Terminology
A decubitus ulcer (from the Latin decubitus, meaning "lying down") is a localized area of tissue necrosis that develops when soft tissue is compressed between a bony prominence and an external surface for a prolonged period. The term "decubitus ulcer" is now considered outdated - the currently preferred term is pressure ulcer or pressure injury. Previous synonyms include bedsore and pressure sore.
- Andrews' Diseases of the Skin, p. 53
- Swanson's Family Medicine Review, p. 682
Epidemiology
- Approximately 1.5-3 million people in the US are affected annually, at a treatment cost of up to $5 billion/year.
- Prevalence in acute care hospitals: 7-9%; in long-term care facilities: 11% (up to 23% in some reports).
- Among patients confined to bed or chair for at least 1 week, prevalence of stage II and greater ulcers can reach 28%.
- 70% of pressure ulcers occur in patients over age 70.
- 95% develop on the lower body: 65% in the pelvic area, 30% on the legs.
- Common anatomic sites: sacrum, ischial tuberosities, greater trochanters, heels, lateral malleoli, and occiput.
- Dermatology 2-Volume Set 5e, p. 2211; Swanson's Family Medicine Review, p. 682
Risk Factors
Immobility-related:
- Spinal cord injury
- Dementias (Alzheimer's, vascular)
- Parkinson disease
- Congestive cardiac failure
- Any disease limiting activity or repositioning
Nutritional:
- Hypoalbuminemia, cachexia
- Inadequate protein, vitamins, minerals, or caloric intake
- Decreased body weight, decreased triceps skinfold thickness
Physiologic/local:
- Incontinence (increases risk fivefold due to moisture)
- Diabetes mellitus, peripheral vascular disease, cerebrovascular disease
- Sepsis, hypotension, anemia
- Moist skin (from perspiration, urine, or feces)
Over 100 risk factors have been identified in total.
- Swanson's Family Medicine Review, p. 682-683; Andrews' Diseases of the Skin, p. 53
Pathophysiology
Four major etiologic factors drive pressure ulcer formation:
1. Pressure
- Interstitial pressures >32 mmHg (normal capillary pressure range is 12-32 mmHg) compromise oxygenation and microcirculation.
- There is an inverse time-pressure curve: slow ulcer formation at low pressures, rapid formation at high pressures (>70 mmHg).
- Because subcutaneous tissue is most susceptible to ischemic damage, deep tissue trauma can occur with little superficial warning.
2. Shearing Forces
- Result from sliding and relative displacement of two opposing surfaces.
- When the head of a supine patient is raised >30 degrees, shear forces occur in the sacral/coccygeal area - vessels in the superficial fascia angulate and thrombose, producing the characteristic undermining seen clinically.
3. Friction
- Occurs when a bedridden patient is dragged across bed sheets.
- Damages the stratum corneum, compromising the skin barrier and accelerating ulcer formation.
4. Moisture
- Perspiration from fever, urine, or feces increases risk of pressure ulcer formation fivefold.
Pathophysiologic Sequence of Events:
- Pressure on tissues overlying bony prominence
- Ischemia from occlusion of blood vessels and lymphatics
- Endothelial cell swelling and vessel leak
- Plasma leakage into interstitial space
- Increased distance between skin cellular elements and blood vessels
- Hemorrhage
- Non-blanchable erythema of skin
- Continued accumulation of edema fluid, blood, inflammatory cells, toxic wastes, and bacteria
- Death of muscle, subcutaneous tissue, and epidermal skin
- Dermatology 2-Volume Set 5e, p. 2211; Swanson's Family Medicine Review, p. 683; Schwartz's Principles of Surgery 11e
Staging (NPUAP Classification)
The National Pressure Ulcer Advisory Panel (NPUAP) staging system is the standard classification. Importantly, ulcers do not necessarily progress sequentially from stage I to IV, nor do they heal in reverse order.
| Stage | Description |
|---|---|
| Suspected Deep Tissue Injury | Intact skin with localized area of purple/maroon discoloration or blood-filled blister from underlying soft tissue damage |
| Stage I | Intact skin with non-blanching redness of a localized area, usually over a bony prominence. In darkly pigmented skin: warmth, edema, discoloration, or induration may be the only clues |
| Stage II | Partial-thickness skin loss involving epidermis and/or dermis. Presents as a shallow open ulcer with a red-pink wound bed (no slough), or as a blister or erosion |
| Stage III | Full-thickness tissue loss. Subcutaneous fat may be visible but bone, tendon, or muscle is NOT exposed. Slough may be present. May include undermining and tunneling |
| Stage IV | Full-thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be present. Often includes undermining and tunneling |
| Unstageable | Full-thickness tissue loss where the wound base is covered by slough or eschar, preventing determination of true depth |
- Washington Manual of Medical Therapeutics; Andrews' Diseases of the Skin; Schwartz's Principles of Surgery 11e
Histopathology
- Stage I (blanching erythema): Dilated superficial dermal capillaries and venules; mild papillary dermal edema; mild perivascular lymphocytic infiltrate; epidermis and dermis remain normal.
- Stage I (non-blanching erythema): Engorgement of capillaries with RBCs, platelet thrombi, and hemorrhage in papillary dermis; sweat gland and subcutaneous fat degeneration.
- Early ulcers: Loss of epidermis; acute inflammation of papillary and reticular dermis.
- Chronic ulcers: Diffusely fibrotic dermis; loss of adnexa; hemorrhagic crust or coagulation necrosis.
- Black eschar stage: Full-thickness skin destruction; general dermal architecture preserved but cellular details obliterated.
- Dermatology 2-Volume Set 5e, p. 2212
Complications
| Complication | Notes |
|---|---|
| Sepsis | Most serious complication; in-hospital death rates 23-36% |
| Osteomyelitis | Especially with deeply undermined or stage IV ulcers |
| Local cellulitis/infection | Polymicrobial; common organisms: Pseudomonas aeruginosa, Proteus spp., S. aureus, B. fragilis, Providencia spp. |
| Peritonitis | If ulcer penetrates into abdominal cavity |
| Fistulas | May develop with deep stage IV ulcers |
| Squamous cell carcinoma (SCC) | Rare, but recognized complication of chronic pressure ulcers (Marjolin's ulcer equivalent) |
| Antibiotic-resistant reservoir | Infected ulcers serve as nosocomial reservoirs for organisms like MRSA |
- Swanson's Family Medicine Review, p. 682; Andrews' Diseases of the Skin
Prevention
- Formal risk assessment using validated tools such as the Braden Scale for all at-risk patients.
- Frequent repositioning:
- Highest-risk patients: every 2 hours
- Lower-risk patients: 2-4 times daily
- Position at 30-degree angle to support surface (not directly on the trochanter)
- Pressure-reducing devices: Static air mattresses, alternating air mattresses, gel mattresses, water mattresses (sheepskins and 2-inch foam pads are insufficient alone)
- Lifting devices (not dragging) during transfers to minimize friction and shear
- Nutrition optimization: Adequate protein, calories, Vitamin C, zinc
- Moisture and incontinence management
- Education of all healthcare providers, patients, family, and caregivers
- Swanson's Family Medicine Review, p. 683; Dermatology 2-Volume Set 5e
Treatment
Treatment is most effective as a multidisciplinary approach involving physicians, nurses, dietitians, physical therapists, and nutritionists.
Systemic Measures
- Vitamin C supplementation: up to 84% reduction in ulcer surface area reported
- Nutritional support: Address hypoalbuminemia, caloric deficit
- Air-fluidized bed therapy: Major improvement over conventional beds
- Treat underlying diseases (CHF, diabetes, vascular disease)
Local Wound Care
- Cleansing: Normal saline is the agent of choice; AVOID povidone-iodine, hypochlorite, acetic acid, and hydrogen peroxide (cytotoxic to healing tissue)
- Debridement: Required to remove necrotic tissue; methods include:
- Sharp/surgical (most efficient)
- Mechanical (wet-to-dry dressings with normal saline)
- Enzymatic (e.g., collagenase/Santyl) - use only until wound bed is clean
- Autolytic (occlusive dressings)
- Exception: Stable dry heel eschars do NOT require debridement
- Moist wound environment: Once clean, maintain moisture with appropriate dressings
Dressing Selection
| Dressing Type | Indication |
|---|---|
| Hydrocolloid / Occlusive | Stage II ulcers; improve healing rates |
| Transparent films | Stage II (light drainage only) |
| Foams | Stage II-III |
| Hydrogels | Dry wounds needing moisture |
| Hydrofibers/Alginates | Full-thickness Stage III-IV |
| Gauze soaked in normal saline | Stage III and IV |
Antibiotic Therapy
- Mild infection: Cephalexin, clindamycin, amoxicillin-clavulanate, or moxifloxacin (x2 weeks); linezolid for MRSA
- Moderate infection: Clindamycin + ciprofloxacin, or ciprofloxacin + ceftriaxone IV, or vancomycin IV for MRSA (x2-4 weeks)
- Severe/bone involvement: Piperacillin-tazobactam, imipenem IV, meropenem IV, or clindamycin + gentamicin IV (x2-12 weeks depending on osteomyelitis); rule out osteomyelitis if clinically suspected
- Drug combination of choice for serious infection: clindamycin + gentamicin (monitor renal function)
Surgical Treatment
- Indicated when necrotic tissue cannot be removed by other means, or when septicemia risk is present
- Flap reconstruction (e.g., myocutaneous gluteus maximus flap for sacral ulcers, V-Y flap for trochanteric ulcers) for stage IV ulcers
- Recurrence rates are high due to the underlying patient population
Adjunctive Therapies (investigational/limited evidence)
-
Negative-pressure wound therapy (promising for Stage III/IV)
-
Electrical stimulation (may accelerate healing)
-
Hyperbaric oxygen, ultrasound, laser, UV radiation
-
Growth factors (PDGF), cultured keratinocyte grafts, skin substitutes
-
Radiant heat, platelet-derived growth factor (Regranex)
-
Topical metronidazole eliminates odor from anaerobic colonization within 36 hours
-
Andrews' Diseases of the Skin, p. 53-54; Swanson's Family Medicine Review, p. 683; Schwartz's Principles of Surgery 11e; Washington Manual of Medical Therapeutics
Key Clinical Pearls
- A small untreated pressure ulcer can develop into a large stage IV ulcer in as little as 1-2 days under high-pressure conditions.
- The sacrum is the single most common site (65% of pelvic girdle ulcers).
- The medial malleolus is the least common site among the major bony prominences.
- Moisture from incontinence increases pressure ulcer risk fivefold.
- Anemia, hypoalbuminemia, and inadequate nutrition are major modifiable risk factors.
- Failure of a pressure ulcer to heal is associated with a significantly higher mortality rate in nursing home residents.
- In-hospital death rates with pressure ulcers range from 23-36% (mostly attributable to severe underlying disease).
Recent evidence: A 2024 systematic review on pressure injury prevention in orthopaedic patients (PMID 39463024) and a 2024 meta-analysis on head-of-bed elevation and pressure ulcer risk in ventilated patients (PMID 39300424) are consistent with current guidelines - routine repositioning, appropriate support surfaces, and careful positioning (head-of-bed angle) remain the cornerstone of prevention.
Image
It looks like your image didn't come through — no attachment was included in your message.
Could you please re-upload the image? Once I can see it, I'll analyze it for you right away.
Why the potassium level decreases with increase in insulin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-based explanation:
Why Insulin Lowers Serum Potassium
The Core Concept: A Shift, Not a Loss
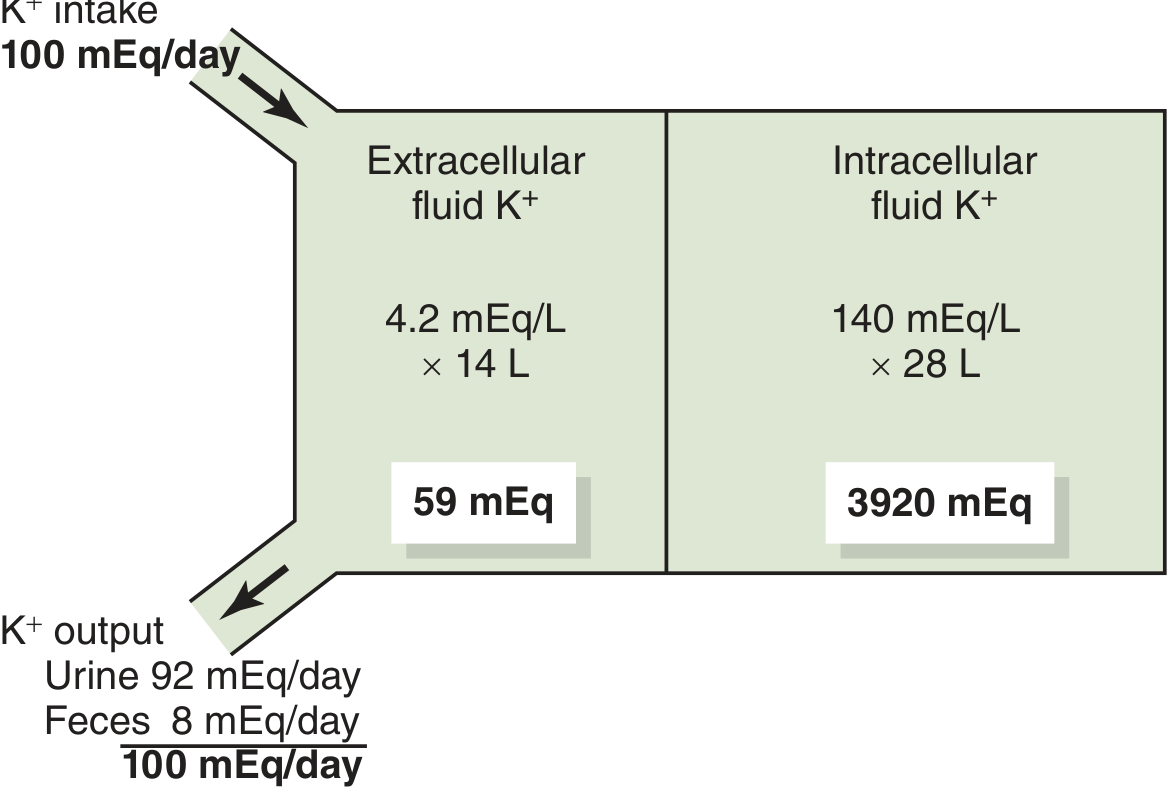
When insulin levels rise, serum (extracellular) potassium falls - but this does not mean potassium leaves the body. It is a transcellular shift: K⁺ moves from the extracellular fluid (ECF) into cells, primarily skeletal muscle and liver. Total body potassium remains unchanged.
This diagram from Guyton illustrates why this shift matters so much - the ECF contains only ~59 mEq of K⁺ total, while cells contain ~3,920 mEq. Even a small redistribution between compartments produces a large change in serum K⁺:
The Molecular Mechanism: Na⁺/K⁺-ATPase Stimulation
Insulin binds to its receptor on skeletal muscle and liver cells, triggering a signaling cascade that directly stimulates membrane-bound Na⁺-K⁺-ATPase (the sodium-potassium pump).
This pump:
- Uses ATP to actively transport 3 Na⁺ out and 2 K⁺ in per cycle
- By increasing its activity, insulin forces more K⁺ from the blood into cells
- This occurs independently of insulin's effect on glucose transport - it is a separate action
Acutely, the effect is driven by increased Na⁺/K⁺-ATPase activity. Chronically (with sustained high insulin), there is also increased abundance of Na⁺/K⁺-ATPase pumps in the plasma membranes of muscle cells.
- Goldman-Cecil Medicine, Internal Potassium Balance
- Morgan & Mikhail's Clinical Anesthesiology 7e, p. 2169
- Guyton and Hall Medical Physiology
Why This Makes Physiological Sense
After every meal, dietary K⁺ is absorbed and enters the ECF. Without a rapid buffering mechanism, this would cause dangerous hyperkalemia before the kidneys (which respond slowly, over hours) can excrete the excess.
The body's solution: a feedback loop between K⁺ and insulin.
- K⁺ rises after a meal → stimulates β-cells of the pancreatic islets to release insulin
- Insulin drives K⁺ into cells → serum K⁺ is rapidly normalized
- Kidneys then slowly excrete the excess K⁺ over the next several hours
This rapid cellular buffering is so important that in insulin-deficient diabetes mellitus, the postprandial rise in serum K⁺ is much greater than normal.
- Goldman-Cecil Medicine
Factors That Also Shift K⁺ Into Cells (Lower Serum K⁺)
| Factor | Mechanism |
|---|---|
| Insulin | Stimulates Na⁺/K⁺-ATPase in muscle and liver |
| Aldosterone | Increases Na⁺/K⁺-ATPase activity in extrarenal tissues + kidneys |
| β₂-adrenergic stimulation | Increases Na⁺/K⁺-ATPase via ↑intracellular cAMP |
| Alkalosis | K⁺ enters cells as H⁺ exits to buffer pH |
In contrast, acidosis, insulin deficiency, β-blockade, and cell lysis all shift K⁺ out of cells and raise serum K⁺.
- Guyton and Hall Medical Physiology, Table 30.1
Clinical Consequences
1. Diabetic Ketoacidosis (DKA) - A Classic Example
In DKA, insulin is absent. Hyperglycemia causes hyperosmolality, driving K⁺ out of cells. The patient may appear normokalemic or even hyperkalemic on admission, despite being total-body K⁺ depleted (K⁺ has been lost in urine). When insulin is administered to treat DKA:
- K⁺ rapidly shifts back into cells
- Serum K⁺ can plummet to dangerously low levels within hours
- This is why K⁺ must be checked before giving insulin in DKA, and why potassium replacement is started early in treatment
- NKF Primer on Kidney Diseases 8e
2. Treatment of Hyperkalemia
Insulin (10 units IV regular insulin, given with 50g dextrose to prevent hypoglycemia) is a first-line treatment for acute hyperkalemia. Onset of action is less than 15 minutes, making it one of the fastest ways to lower serum K⁺.
- Rosen's Emergency Medicine
3. Parenteral Nutrition
Patients receiving TPN with high glucose loads get large amounts of endogenous insulin secretion, which can drive K⁺ into cells and cause hypokalemia. As much as 240 mEq/day of potassium replacement may be required. Importantly - if hypokalemia is seen in this setting, the answer is more potassium, not insulin.
- Schwartz's Principles of Surgery 11e
Summary
Insulin ↑ → Na⁺/K⁺-ATPase activity ↑ in skeletal muscle and liver → K⁺ shifts from ECF into cells → Serum K⁺ ↓
This is a transcellular shift (no change in total body K⁺), is independent of insulin's glucose-lowering effect, occurs within minutes, and is physiologically essential for buffering postprandial potassium loads before the kidneys respond.
This is a shared conversation. Sign in to Orris to start your own chat.