op Poisoning
Reading File
Finding Sources
Searching PubMed
"organophosphate poisoning"[MeSH Terms] AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Here is a complete review of Organophosphate (OP) Poisoning.
Organophosphate (OP) Poisoning
Mechanism
Organophosphates (OPs) irreversibly inhibit acetylcholinesterase (AChE), preventing the breakdown of acetylcholine (ACh) at synapses. This leads to accumulation of ACh at muscarinic, nicotinic, and CNS receptors, causing overwhelming cholinergic stimulation.
Common sources include agricultural insecticides (parathion, malathion, chlorpyrifos), chemical warfare nerve agents (sarin, soman, tabun, VX), and occupational/industrial exposure.
Clinical Features — The Cholinergic Toxidrome
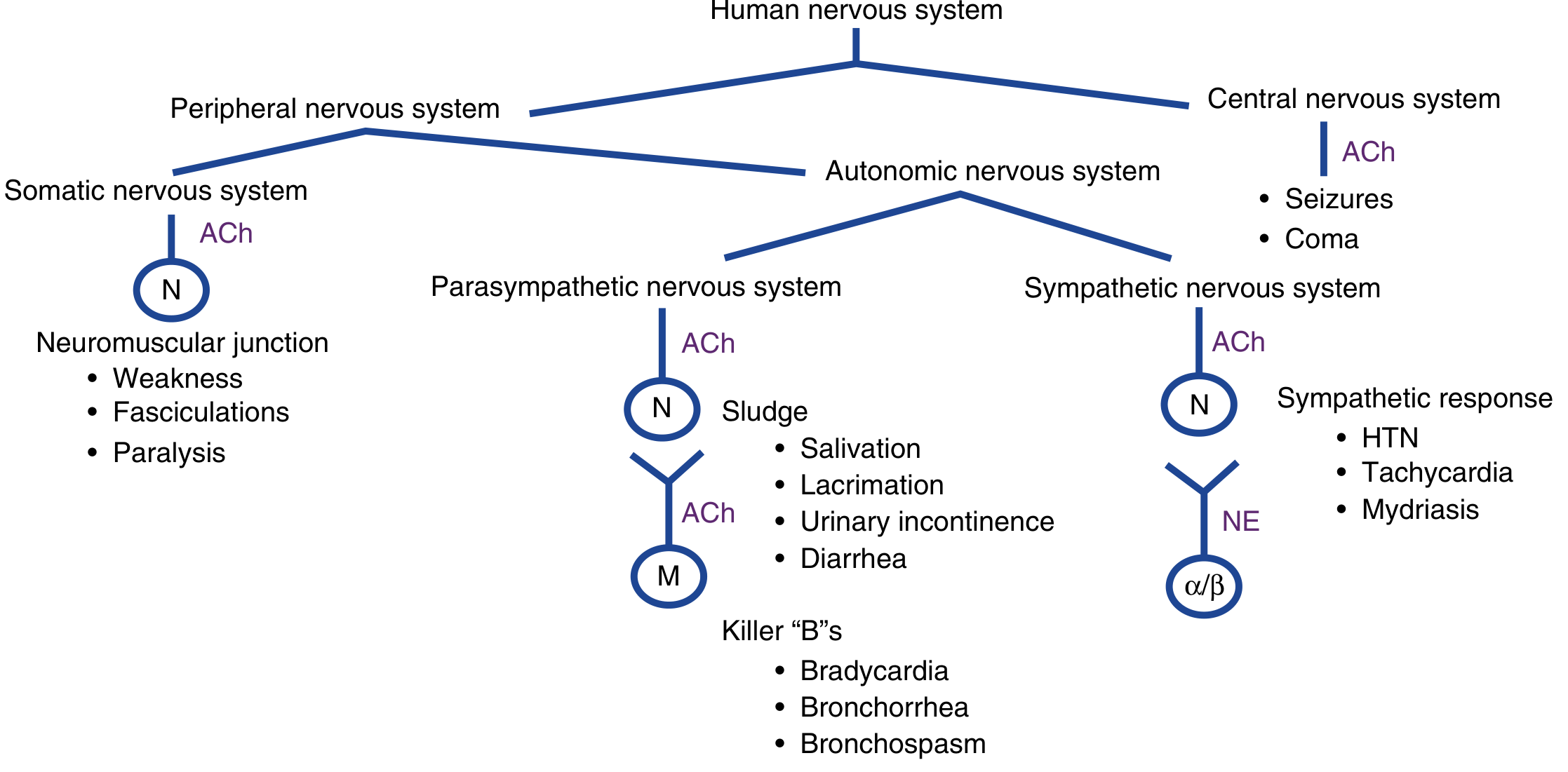
Muscarinic Effects (Parasympathetic — "SLUDGE" + "Killer Bs")
| Mnemonic | Features |
|---|---|
| SLUDGE | Salivation, Lacrimation, Urination, Defecation, GI cramps, Emesis |
| Killer Bs | Bradycardia, Bronchorrhea, Bronchospasm |
| Other | Miosis, diaphoresis, abdominal pain |
Nicotinic Effects (NMJ + Sympathetic ganglia)
- Neuromuscular junction: Muscle fasciculations, weakness, paralysis, areflexia
- Sympathetic stimulation: Tachycardia, hypertension, mydriasis (may mask parasympathetic signs)
CNS Effects
- Anxiety, restlessness, tremor, headache, dizziness
- Confusion, delirium, hallucinations
- Seizures, coma
Death is most commonly due to respiratory failure — a combination of bronchorrhea, bronchospasm, and respiratory muscle paralysis.
Phases of Toxicity
| Phase | Timing | Features |
|---|---|---|
| Acute cholinergic | Minutes–hours | Full SLUDGE/Killer Bs syndrome |
| Intermediate syndrome | 1–5 days (up to 40% of ingestions) | Proximal limb weakness, cranial nerve palsies, neck flexor weakness, respiratory paralysis; no cholinergic signs; may be fatal |
| Delayed neuropathy (OPIDN) | 2–5 weeks | Distal symmetrical sensorimotor polyneuropathy, progressing to atrophy; corticospinal signs (especially with TOCP) |
ECG changes include ST-segment changes, peaked T waves, AV block, and QT prolongation.
Diagnosis
- Clinical diagnosis — do not wait for lab confirmation. History + cholinergic toxidrome is sufficient to initiate treatment.
- A characteristic garlic or hydrocarbon odor may be present.
- RBC cholinesterase (true AChE) and plasma pseudocholinesterase (butyrylcholinesterase) levels confirm exposure but are not needed to start treatment.
- EMG can identify AChE inhibition at neuromuscular junctions.
Management
1. Decontamination
- Remove and discard all clothing (dermal absorption is significant).
- Flush skin thoroughly with water (primary method); dry agents like flour, bentonite, or military resins are alternatives.
- Gastric lavage and activated charcoal are not beneficial — rapid GI absorption and profuse vomiting/diarrhea limit their utility.
- Caregivers must wear Level C PPE (full-face air-purifying mask, chemical-resistant suit, nitrile/butyl rubber gloves).
2. Stabilization & Supportive Care
- Airway is the priority — suction secretions, provide O₂, and initiate ventilatory support early.
- For RSI: prefer rocuronium 1 mg/kg over succinylcholine (succinylcholine is metabolized by cholinesterase and may have prolonged effect of 4–6 hours in OP poisoning).
- Benzodiazepines for seizures and agitation (after airway secured).
- Tachyarrhythmias — treat the underlying cholinergic excess, not with beta-blockers.
- No role for hemodialysis or enhanced elimination.
3. Antidote Therapy
Atropine (Muscarinic Blocker)
- First-line, competitive inhibitor of ACh at muscarinic receptors.
- Dose: 1–3 mg IV (0.05 mg/kg in children); double the dose every 5 minutes until muscarinic effects are controlled.
- Severely poisoned patients may require 200–500 mg in the first hour.
- Once stabilized, initiate infusion at 10–20% of total loading dose per hour.
- Endpoint: Drying of airway secretions, normalized respiratory rate, ease of breathing.
- ⚠️ Atropine does not reverse nicotinic effects (muscle paralysis).
Pralidoxime (2-PAM) — Oxime / AChE Reactivator
- Binds the OP–cholinesterase complex → conformational change → restores AChE function.
- Must be given early, before "aging" (irreversible covalent bonding) occurs.
- Indicated in moderate/severe poisoning: respiratory failure, fasciculations, seizures, dysrhythmias, large atropine requirements.
- Dose: 1–2 g IV (25–50 mg/kg pediatric) over 30 min, may repeat hourly; or 2 g over 20 min followed by 500 mg/h infusion for up to 7 days.
- Does not help the intermediate syndrome or delayed neuropathy.
Benzodiazepines
- For seizures and agitation: adequate dosing is required; do not under-treat.
Summary Treatment Table
| Drug | Adult Dose | Pediatric Dose | Route | Titration |
|---|---|---|---|---|
| Atropine | 1–3 mg | 0.05 mg/kg | IV/IM | Double every 5 min until secretions dry |
| Pralidoxime (2-PAM) | 1–2 g over 30 min | 25–50 mg/kg | IV/IM | Repeat hourly or infusion 500 mg/h |
| Diazepam/Lorazepam | Standard seizure doses | — | IV | Titrate to seizure control |
Special Considerations
- Chemical warfare nerve agents (sarin, soman, VX): Extremely potent; death within minutes. Soman undergoes aging within minutes, leaving little time for oxime administration.
- Intermediate syndrome: Does not respond to atropine or pralidoxime — requires respiratory support.
- Children are at higher risk due to smaller body size and lower baseline cholinesterase activity.
- Chronic low-level exposure (farmworkers, exterminators): Subtle, nonspecific symptoms without the classic cholinergic syndrome.
Key Points
- OP poisoning = irreversible AChE inhibition → ACh accumulation
- Classic toxidrome: SLUDGE + Killer Bs + NMJ effects + CNS effects
- Death = respiratory failure (bronchorrhea + muscle paralysis)
- Antidotes: Atropine (titrate aggressively) + Pralidoxime (early, before aging)
- Prefer rocuronium over succinylcholine for intubation
- Intermediate syndrome occurs days later and does not respond to antidotes
Sources: Rosen's Emergency Medicine, 10e — Tintinalli's Emergency Medicine, 9e — Adams and Victor's Principles of Neurology, 12e
Recent evidence: A 2025 systematic review (PMID 38797902) examined glycopyrrolate as an alternative anticholinergic in OP/carbamate poisoning — this may be relevant when atropine supplies are exhausted or in settings where atropine is scarce.
This is a shared conversation. Sign in to Orris to start your own chat.