Explain each and everything about the anterior abdominal wall with help of diagrams. I want each minor detail about that topic. Also explain the clinical correlates along the content
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the diagrams and detailed content needed. Let me compile the comprehensive answer.
The Anterior Abdominal Wall - Complete Anatomy with Clinical Correlates
1. Overview and Boundaries
The anterior abdominal wall extends from the thoracic cage superiorly (costal margins and xiphoid process) to the pelvic brim and inguinal ligaments inferiorly. Laterally it blends with the flank (posterolateral wall). It is a multi-layered structure whose components - skin, fascia, muscles, aponeuroses, and peritoneum - interact to protect abdominal viscera, permit trunk movement, assist in breathing, voiding, and childbirth, and resist raised intra-abdominal pressure.
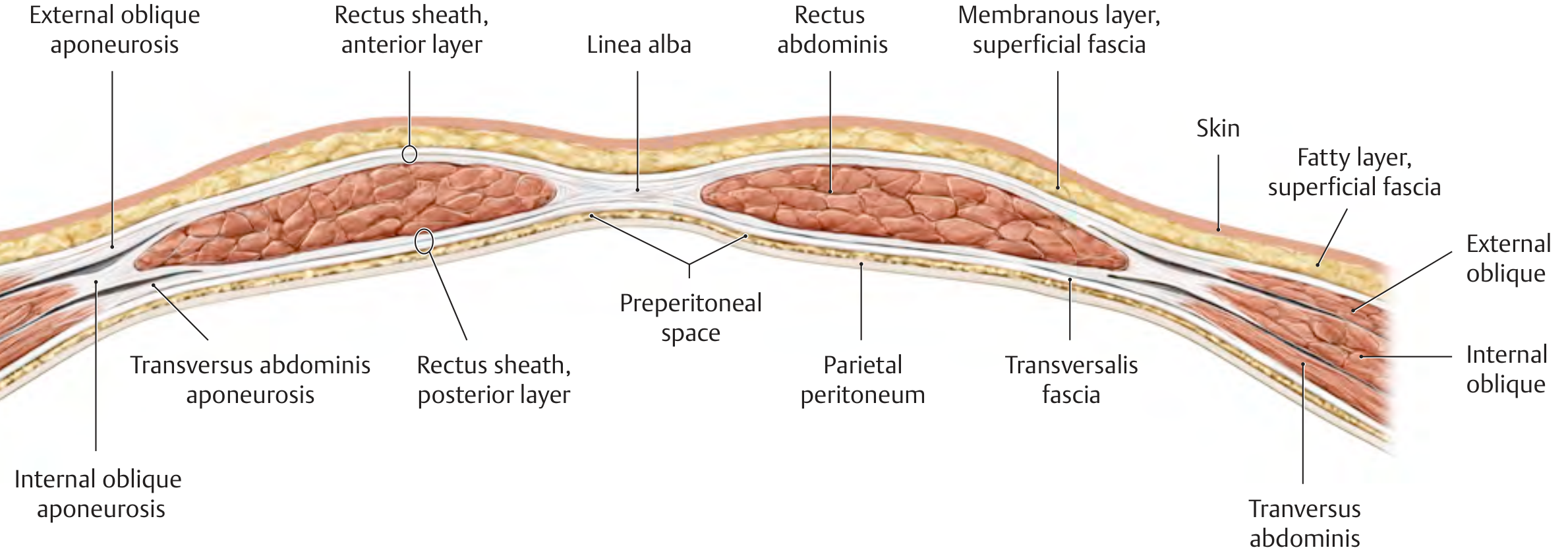
2. Layers of the Anterior Abdominal Wall (Superficial to Deep)
From outside inward, the layers are:
- Skin
- Superficial fascia (Camper's + Scarpa's)
- External oblique muscle and aponeurosis
- Internal oblique muscle and aponeurosis
- Transversus abdominis muscle and aponeurosis
- Transversalis fascia
- Extraperitoneal (preperitoneal) fat
- Parietal peritoneum
The cross-sectional diagram below shows these layers clearly:
3. Fascial Layers
3.1 Camper's Fascia (Fatty Layer)
The most superficial layer of the abdominal wall below the skin. It is a fatty layer (panniculus adiposus) that can accumulate enormous amounts of adipose tissue in obese individuals. It is continuous inferiorly with the outer layer of perineal and genital fascia, and contains the dartos muscle fibers of the scrotum. The major vessels in this layer are the superficial epigastric and superficial circumflex iliac vessels - tributaries of the femoral vessels.
- Lymphatics drain inferiorly to the inguinal lymph nodes. Lymphatics cross the inguinal ligament, which is why they enter the surgical field during open hernia repair.
3.2 Scarpa's Fascia (Membranous Layer)
A deep membranous condensation of the superficial fascia, described as the deep fascia of Scarpa. It forms:
- The fundiform ligament of the penis (suspensory ligament of the clitoris in females)
- Continues onto the penis/scrotum, ultimately fusing with the superficial perineal fascia (Colles' fascia)
- Fuses with the fascia innominata investing the external oblique, which is bound inferiorly to the inguinal ligament and pubis, then blends with the fascia lata of the thigh
Clinical Correlate - Extravasation of Urine: When the anterior urethra ruptures (e.g., straddle injury), urine follows the planes of Scarpa's fascia. Because Scarpa's fascia fuses with the fascia lata below the inguinal ligament (preventing spread into the thigh) and with Colles' fascia in the perineum, extravasated urine spreads: upward under Scarpa's fascia onto the anterior abdominal wall, into the scrotum/labia, and into the perineum - but NOT into the thigh or gluteal region. This creates the classic butterfly bruising of the perineum.
3.3 Transversalis Fascia
A continuous sheet lining the deep surface of the transversus abdominis muscle. It is part of the endoabdominal fascia. It has key surgical landmarks:
- The deep inguinal ring is an oval opening in the transversalis fascia
- The inferior epigastric vessels run just medial to this ring
- Below the arcuate line, transversalis fascia is the only layer posterior to rectus abdominis (no aponeurotic posterior sheath exists here)
3.4 Extraperitoneal (Preperitoneal) Fat
Contains variable fat between the transversalis fascia and the peritoneum. Important in the context of laparoscopic hernia repair (the preperitoneal space - the "space of Retzius" anteriorly and the "space of Bogros" laterally - is the plane used in the TEP and TAPP approaches).
4. Muscles of the Anterior Abdominal Wall
The anterior wall muscles divide into two groups:
A. Lateral (Flat) Muscles - three muscle layers with aponeuroses that decussate at the midline:
- External oblique
- Internal oblique
- Transversus abdominis
B. Anterior (Straight/Strap) Muscles:
- Rectus abdominis
- Pyramidalis

4.1 External Oblique
| Feature | Detail |
|---|---|
| Origin | Lower 8 ribs (5th-12th), interdigitating with serratus anterior and latissimus dorsi |
| Insertion | Anterior iliac crest, pubic tubercle; aponeurosis forms anterior rectus sheath, inguinal ligament, lacunar ligament |
| Fiber direction | Inferiomedially ("hands in pockets" direction) |
| Action | Compresses abdomen; contralateral trunk rotation; assists in raising intraabdominal pressure |
| Innervation | Intercostal nerves T7-T12 |
Inguinal Ligament: The inferior free margin of the external oblique aponeurosis folds back on itself to form the inguinal (Poupart's) ligament, running from the ASIS to the pubic tubercle. This is the floor of the inguinal canal.
Superficial Inguinal Ring: An inverted V-shaped gap in the external oblique aponeurosis just above and lateral to the pubic tubercle. Its medial and lateral crura are connected by intercrural fibers. The spermatic cord (or round ligament of the uterus) passes through it.
Lacunar (Gimbernat's) Ligament: The rolled-under medial portion of the inguinal ligament that fans out to attach to the pectineal line of the pubis. It forms the medial wall of the femoral ring and is the sharp edge responsible for strangulation of femoral hernias.
Pectineal (Cooper's) Ligament: Formed by the periosteum of the superior pubic ramus plus the lacunar ligament. Used as a strong fixation point in hernia repairs (e.g., McVay repair).
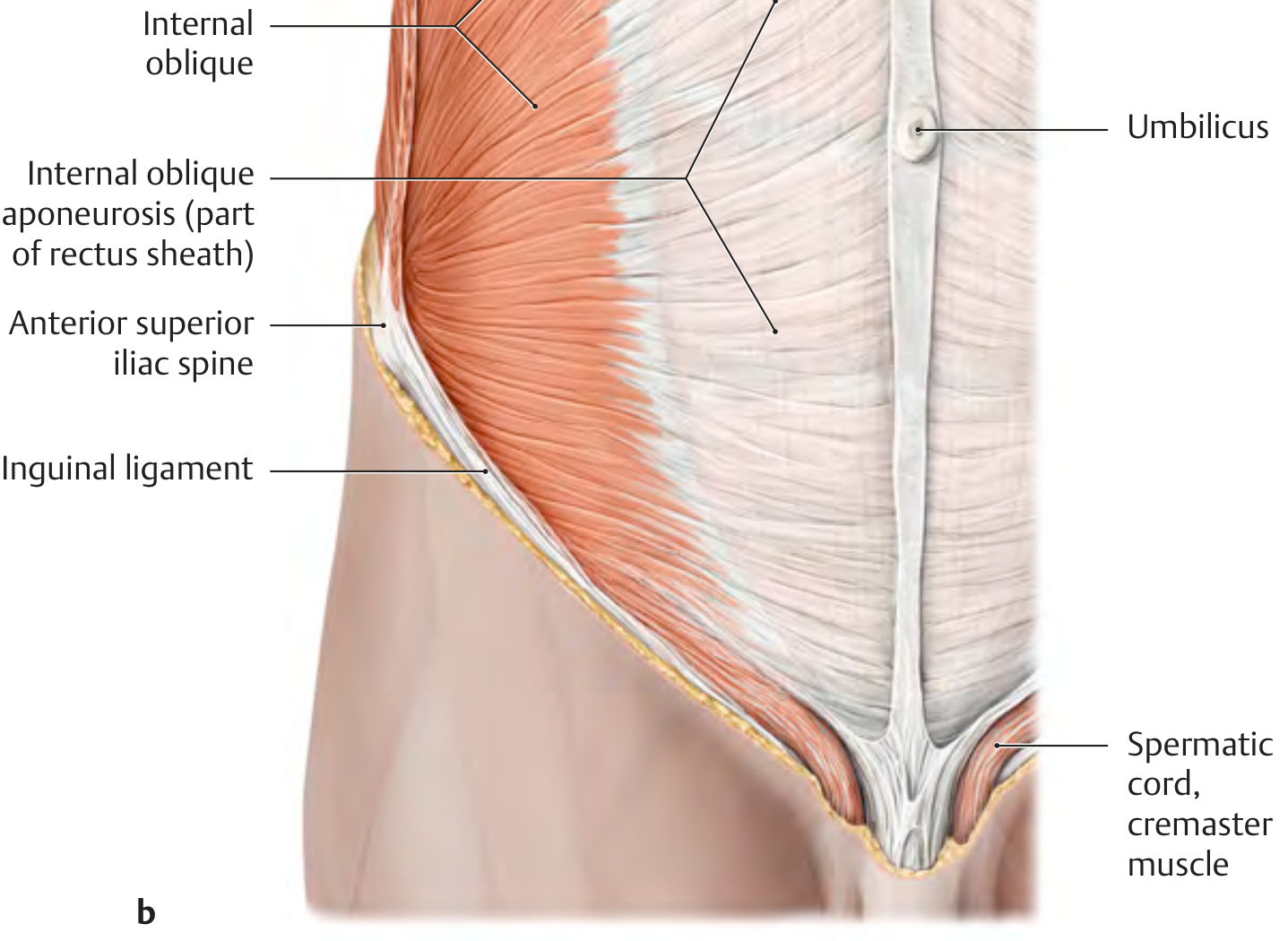
4.2 Internal Oblique
| Feature | Detail |
|---|---|
| Origin | Thoracolumbar fascia, anterior iliac crest, lateral inguinal ligament |
| Insertion | Lower 3-4 costal cartilages; aponeurosis forms both layers of rectus sheath (it splits); pubic crest |
| Fiber direction | Superomedially (perpendicular to external oblique) |
| Action | Compresses abdomen; ipsilateral trunk rotation |
| Innervation | Intercostal nerves T7-T12, iliohypogastric, ilioinguinal (L1) |
The inferior free border of the internal oblique arches over the deep inguinal ring with the transversus abdominis fibers, forming the conjoint tendon (falx inguinalis) where they fuse and insert on the pubic crest and pectineal line.
Cremaster Muscle: The inferior fibers of the internal oblique extend onto the spermatic cord as the cremaster muscle, innervated by the genitofemoral nerve (L1, L2). Contraction elevates the testis.
Clinical Correlate - Cremasteric Reflex: Stroking the inner thigh causes reflex elevation of the testis (via the genitofemoral nerve). This reflex is absent or diminished in upper motor neuron lesions above L1. It must be distinguished from testicular torsion - in torsion the cremasteric reflex is typically absent ipsilaterally. Loss of the reflex in an acute scrotum strongly suggests torsion and requires urgent surgical exploration.
4.3 Transversus Abdominis
| Feature | Detail |
|---|---|
| Origin | Thoracolumbar fascia, inner surface of lower 6 costal cartilages, anterior iliac crest, lateral inguinal ligament |
| Insertion | Aponeurosis to linea alba; lower fibers: pubic crest, pectineal line (conjoint tendon with internal oblique) |
| Fiber direction | Horizontal (transversely) |
| Action | Primary compressor of abdominal contents; maintains intra-abdominal pressure; stabilizes lumbar spine |
| Innervation | Intercostal nerves T7-T12, iliohypogastric, ilioinguinal (L1) |
The transversus abdominis activation concept is central to physiotherapy for low back pain - it acts as an internal corset stabilizing the lumbar spine.
4.4 Rectus Abdominis
| Feature | Detail |
|---|---|
| Origin | Xiphoid process, cartilages of ribs 5-7 |
| Insertion | Pubic symphysis, pubic crest (between pubic tubercle and symphysis) |
| Action | Flexes lumbar spine, compresses abdomen, stabilizes pelvis, assists expiration |
| Innervation | Intercostal nerves T5-T11, subcostal nerve (T12) |
- Divided by 3 (occasionally 4) fibrous tendinous intersections that are fused to the anterior rectus sheath but NOT the posterior sheath - this allows the muscle to be elevated from its posterior sheath in operations like the TRAM flap.
- The tendinous intersections are what create the "six pack" in well-muscled individuals.
- The semilunar line (Spigelian line) is the curved vertical depression marking the lateral edge of rectus abdominis, corresponding to the lateral convergence of the three aponeuroses.
Clinical Correlate - Rectus Sheath Hematoma: Sudden shearing forces (coughing, sneezing, strenuous exercise, anticoagulation) can rupture the inferior epigastric artery or its branches within the rectus sheath, producing a painful tender mass. Above the arcuate line, the posterior sheath is intact and the hematoma is contained. Below the arcuate line, there is no posterior sheath - blood can spread freely within the preperitoneal space, causing a larger, potentially life-threatening bleed. On CT it appears as a hyperattenuating mass within the rectus muscle/sheath.
4.5 Pyramidalis
| Feature | Detail |
|---|---|
| Origin | Pubis, anterior to rectus abdominis insertion |
| Insertion | Linea alba (runs within the inferior part of the rectus sheath) |
| Action | Tenses the linea alba |
| Innervation | Subcostal nerve (T12) |
| Variability | Absent in 10-25% of individuals (bilateral absence most common) |
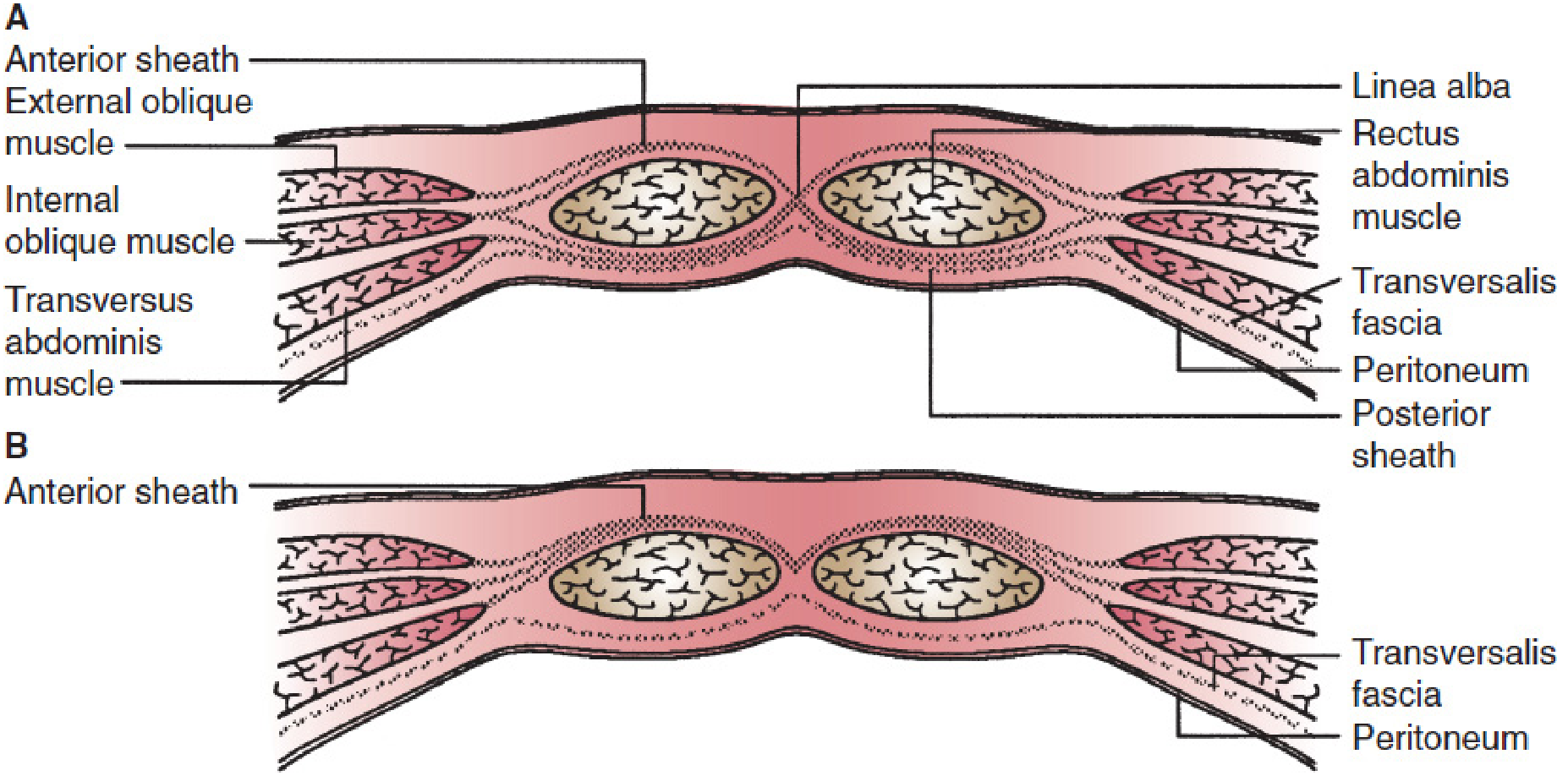
5. The Rectus Sheath
The rectus sheath is the aponeurotic compartment formed by decussation of the three lateral muscle aponeuroses around the rectus abdominis. Its composition varies at two levels:
Above the Arcuate Line (Upper 3/4 of rectus)
| Layer | Composition |
|---|---|
| Anterior sheath | External oblique aponeurosis + anterior lamina of internal oblique aponeurosis |
| Posterior sheath | Posterior lamina of internal oblique aponeurosis + transversus abdominis aponeurosis |
The transversalis fascia and peritoneum lie deep to the posterior sheath.
Below the Arcuate Line (Lower 1/4 of rectus)
All three aponeuroses transfer to the anterior surface, forming a thick anterior sheath. There is no posterior sheath - the rectus abdominis rests directly on the transversalis fascia.
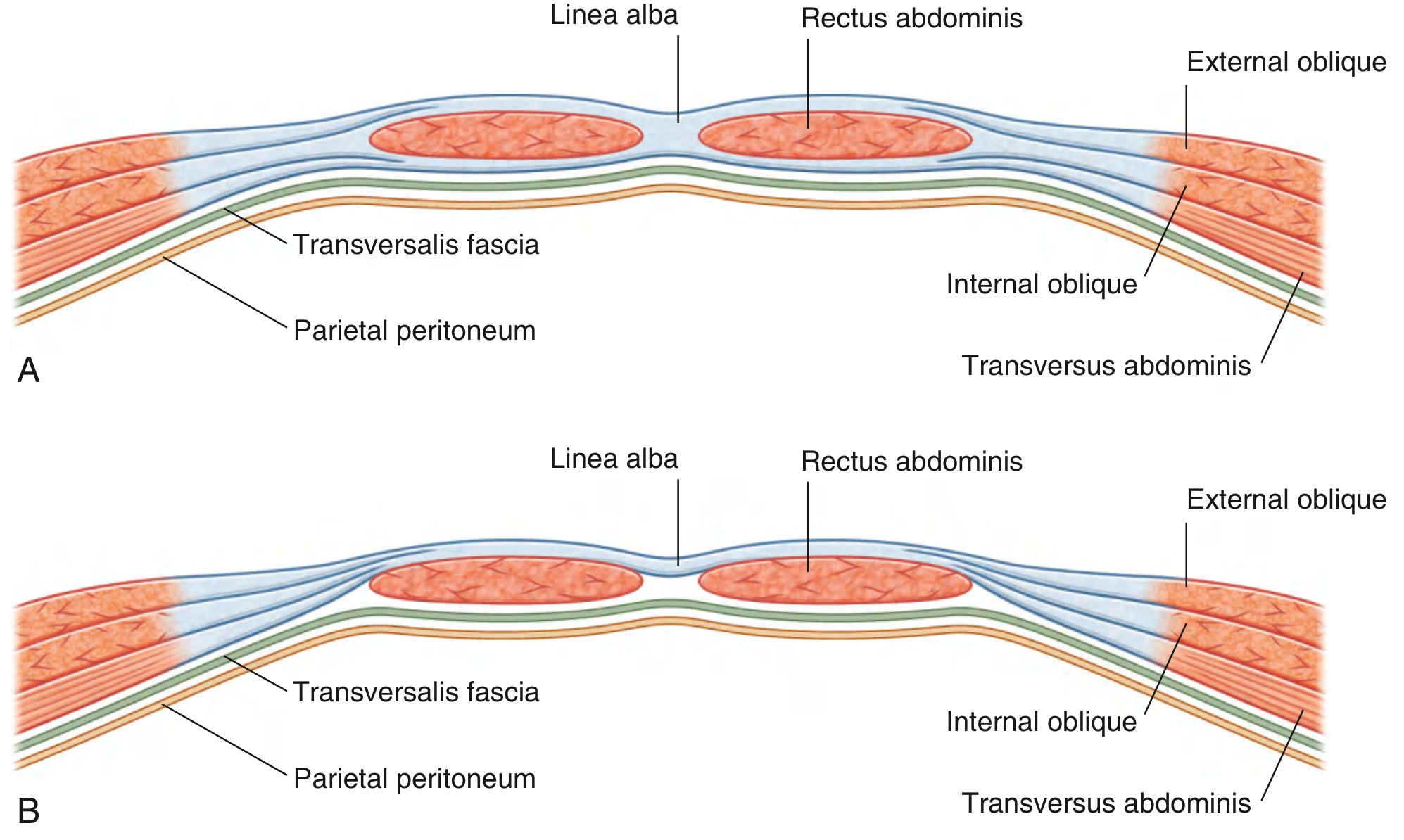
The Arcuate Line (Line of Douglas): Located approximately halfway between the umbilicus and pubic symphysis (often at the level of the anterior superior iliac spines). It marks the inferior free curved edge of the posterior rectus sheath. It is not a sharp line - the aponeurotic fibers attenuate gradually rather than ending abruptly.
The Linea Alba: The midline confluence of the aponeuroses of both rectus sheaths and the three lateral abdominal muscles. It extends from the xiphoid process to the pubic symphysis, being wide superiorly (~1-2 cm above the umbilicus) and narrowing to a knife-edge below the umbilicus.
Clinical Correlate - Epigastric Hernia: Defects in the linea alba above the umbilicus allow preperitoneal fat (and occasionally peritoneum) to herniate. These occur where vessels penetrate the linea alba, creating areas of relative weakness. They are usually small (1-2 cm), present as a midline epigastric nodule, and can be acutely painful if the fat pad strangulates. Treatment is surgical repair.
Clinical Correlate - Umbilical Hernia: The umbilicus is a natural scar where the linea alba is weakest. In adults, factors that increase intra-abdominal pressure (obesity, pregnancy, ascites, chronic cough) predispose to umbilical herniation. Umbilical hernias in adults rarely close spontaneously and often require repair when symptomatic.
Clinical Correlate - Diastasis Recti: Widening of the linea alba from separation of the two rectus muscles. Commonly seen in multiparous women and obese individuals. The widened gap allows the abdominal wall to bulge midline on Valsalva, resembling a hernia but without a true fascial defect or sac. Management is mainly physiotherapy (transversus abdominis strengthening); repair is rarely needed unless symptomatic.
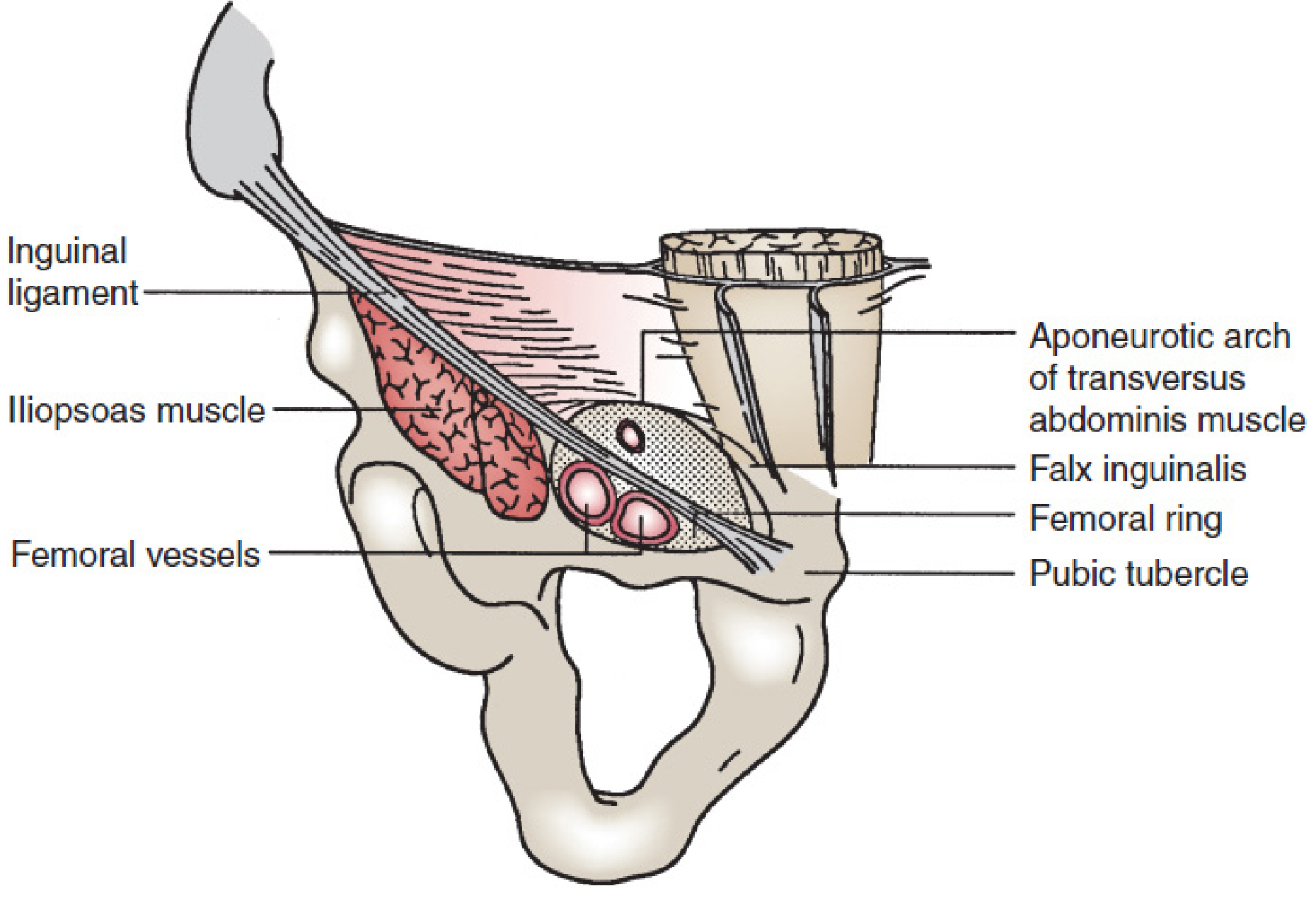
6. The Inguinal Canal
The inguinal canal is a 4 cm oblique passage through the anterior abdominal wall. It runs from the deep inguinal ring to the superficial inguinal ring, directed downward and medially. It is created embryologically by the descent of the testis (and processus vaginalis) through the abdominal wall layers.
Walls of the Inguinal Canal
| Wall | Structure |
|---|---|
| Anterior | External oblique aponeurosis (whole length); internal oblique muscle (lateral 1/3) |
| Posterior (floor of posterior wall) | Transversalis fascia (whole length); conjoint tendon (medial 1/3) |
| Roof | Arching fibers of internal oblique and transversus abdominis |
| Floor | Inguinal ligament (rolled inferior edge of external oblique aponeurosis); lacunar ligament medially |
Deep Inguinal Ring
- An oval opening in the transversalis fascia
- Located midway between the ASIS and pubic tubercle, ~1.25 cm above the midinguinal point
- The inferior epigastric vessels run just medial to it (this is the key landmark separating direct from indirect hernias)
Superficial Inguinal Ring
- An inverted V-shaped gap in the external oblique aponeurosis
- Located just above and lateral to the pubic tubercle
- Bounded by medial and lateral crura and intercrural fibers
Contents of the Inguinal Canal
In Males:
- Spermatic cord (ductus deferens, testicular artery, pampiniform venous plexus, genital branch of genitofemoral nerve, cremasteric artery, artery to the ductus deferens, lymphatics)
- Ilioinguinal nerve (runs on the surface of the cord, not within)
In Females:
- Round ligament of the uterus (derivative of gubernaculum)
- Ilioinguinal nerve

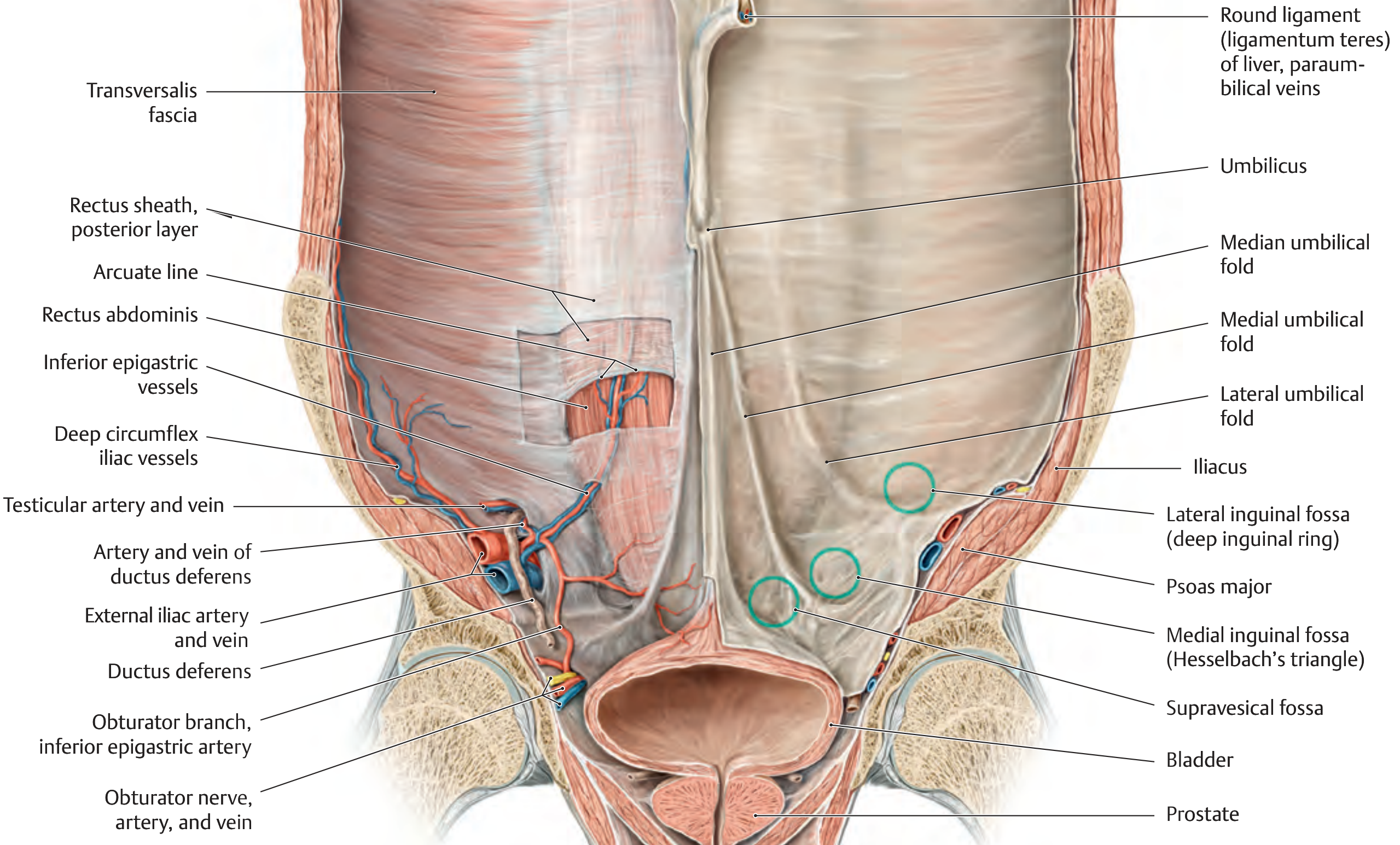
7. Internal Surface of the Anterior Abdominal Wall
Viewed from inside (laparoscopic perspective), the lower abdominal wall shows five peritoneal folds converging toward the umbilicus:
| Fold | Contents |
|---|---|
| Median umbilical fold (1, unpaired) | Obliterated urachus (median umbilical ligament) |
| Medial umbilical folds (2, paired) | Obliterated umbilical arteries |
| Lateral umbilical folds (2, paired) | Inferior epigastric vessels |
Between these folds are three paired fossae - the potential sites of herniation:
| Fossa | Location | Type of Hernia |
|---|---|---|
| Supravesical fossa | Between median and medial folds | Supravesical hernia |
| Medial inguinal fossa (Hesselbach's triangle) | Between medial and lateral folds | Direct inguinal hernia |
| Lateral inguinal fossa | Lateral to lateral umbilical fold (= deep inguinal ring) | Indirect inguinal hernia |
8. Hesselbach's Triangle
This is the key weak zone of the posterior inguinal wall, bounded by:
- Lateral border: Inferior epigastric vessels
- Medial border: Lateral edge of rectus abdominis
- Inferior border: Inguinal ligament (iliopubic tract)
The floor here consists only of transversalis fascia covered by external oblique aponeurosis - making it inherently weak, especially in elderly, obese, or straining individuals.
9. Hernias of the Anterior Abdominal Wall
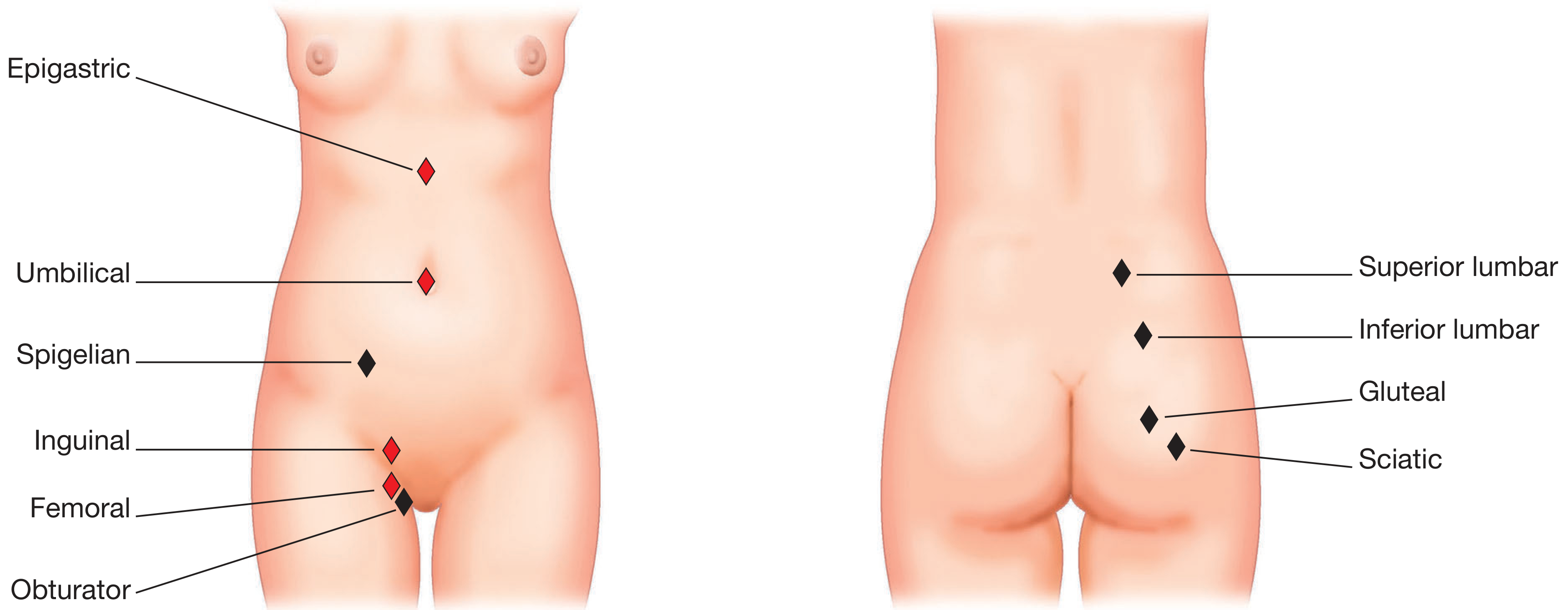
Summary Table of Hernias
| Hernia | Internal Opening | External Opening | Key Features |
|---|---|---|---|
| Indirect inguinal | Lateral inguinal fossa (deep inguinal ring, lateral to inferior epigastric vessels) | Superficial inguinal ring | Congenital (patent processus vaginalis) or acquired; can descend into scrotum; more common in males; can strangulate |
| Direct inguinal | Medial inguinal fossa (Hesselbach's triangle) | Superficial inguinal ring | Always acquired; medial to inferior epigastric vessels; broad base; rarely strangulates; more common in elderly; bladder can herniate into it |
| Femoral | Femoral ring (below inguinal ligament, medial to femoral vein) | Saphenous opening (fossa ovalis) | More common in females; small tight ring with lacunar ligament as medial wall makes strangulation very common (~40%); presents as lump in upper medial thigh |
| Epigastric | Linea alba defect | Palpable subcutaneous | Preperitoneal fat; usually small; painful on palpation |
| Umbilical | Umbilical ring | Umbilical | Patent umbilical ring; in adults associated with raised intra-abdominal pressure |
| Spigelian | Semilunar line / lateral margin of rectus sheath | Interparietal (between muscle layers) | Often occult clinically; may present with pain without visible swelling; requires CT for diagnosis |
| Paraumbilical | Just above or below umbilical ring | Visible protrusion | Very common in obese/multiparous; more likely to strangulate than true umbilical hernias |
Clinical Correlate - Distinguishing Inguinal from Femoral Hernia: The key landmark is the pubic tubercle. An inguinal hernia lies above and medial to the pubic tubercle; a femoral hernia lies below and lateral to it. This distinction is critical preoperatively. Femoral hernias have a 10-fold higher rate of strangulation and need urgent repair.
Clinical Correlate - Sliding Hernia: An acquired indirect hernia where a retroperitoneal organ (commonly caecum on the right, sigmoid on the left, or bladder in direct hernias) forms part of the wall of the hernia sac - there is no true peritoneal sac separating it. This is a hazard at surgery because inadvertent incision of the sac can open into the bowel or bladder. Recognized when the contents of a sac cannot be reduced or when the sac appears "fused" to the hernial contents.
Clinical Correlate - Pantaloon Hernia: Simultaneous direct and indirect inguinal hernias on the same side, straddling the inferior epigastric vessels ("riding astride" like pantaloon trousers). Both hernias emerge through the superficial inguinal ring.
10. Blood Supply
Deep Arterial Supply
| Vessel | Origin | Territory |
|---|---|---|
| Superior epigastric artery | Terminal branch of internal thoracic (mammary) artery | Enters rectus sheath superiorly, supplies upper rectus |
| Inferior epigastric artery | External iliac artery (just above inguinal ligament) | Enters rectus sheath inferiorly, supplies lower rectus; anastomoses with superior epigastric near umbilicus |
| Deep circumflex iliac artery | External iliac artery | Lateral abdominal muscles |
| Lower 3-4 intercostal arteries (T8-T12) | Aorta (posterior intercostal arteries) | Lateral muscles |
| Lumbar arteries | Aorta | Lateral muscles |
The superior and inferior epigastric arteries anastomose within the rectus sheath near the umbilicus - this anastomosis is used in reconstructive surgery (e.g., TRAM flap for breast reconstruction).
Clinical Correlate - TRAM/DIEP Flap for Breast Reconstruction: The deep inferior epigastric perforator (DIEP) flap uses the inferior epigastric vessels as the pedicle. Understanding the anatomy of the rectus sheath and the perforating vessels through the anterior sheath is fundamental to flap harvest. In TRAM flaps, the rectus muscle is sacrificed with the skin/fat, while DIEP flaps spare the muscle.
Clinical Correlate - Inferior Epigastric Artery Injury in Trocar Placement: During laparoscopic surgery, trocars placed without transillumination to identify the inferior epigastric vessels can lacerate them. The inferior epigastric artery runs just medial to the deep inguinal ring. Trocars should be placed lateral to the rectus abdominis (lateral to the visible pulsation) or at the umbilicus to avoid this vessel.
Superficial Arterial Supply
- Superficial epigastric artery - femoral artery branch, runs superiorly toward the umbilicus
- Superficial circumflex iliac artery - femoral artery branch, runs toward the ASIS
- These supply the skin and subcutaneous tissue below the umbilicus
Venous Drainage
- Superior: thoracoepigastric veins drain to axillary veins
- Inferior: superficial epigastric veins drain to femoral veins
- Deep: superior and inferior epigastric veins accompany the arteries
Clinical Correlate - Caput Medusae in Portal Hypertension: In portal hypertension, paraumbilical veins (within the ligamentum teres of the liver) become dilated and visible on the anterior abdominal wall, radiating from the umbilicus - "caput medusae." This occurs because the paraumbilical veins communicate with both the portal system (at the left branch of the portal vein) and the systemic veins of the anterior abdominal wall, forming a portosystemic collateral.
11. Nerve Supply
| Nerve | Level | Territory |
|---|---|---|
| Intercostal nerves (anterior cutaneous branches) | T7-T11 | Abdominal wall skin in parallel bands; T10 corresponds to umbilicus level |
| Subcostal nerve | T12 | Below umbilicus, above groin |
| Iliohypogastric nerve | L1 | Skin above pubis (anterior cutaneous branch), lateral hip (lateral cutaneous branch) |
| Ilioinguinal nerve | L1 | Skin of medial thigh, scrotum (anterior scrotal)/labia majora, pubis |
| Genitofemoral nerve | L1, L2 | Genital branch: cremaster; femoral branch: skin of femoral triangle |
The nerves T7-T12 and L1 travel in a neurovascular plane between the internal oblique and transversus abdominis, then pierce the lateral rectus sheath to enter the muscle.
Dermatomal Landmarks (Clinically Important):
- T7: xiphoid
- T10: umbilicus
- L1: inguinal ligament / groin
Clinical Correlate - Referred Pain from Appendix: Appendicular pain initially presents as periumbilical pain (T10 dermatome, same as the appendix's somatic sensory level) before localizing to the right iliac fossa (when the overlying parietal peritoneum becomes inflamed). This shift from visceral to somatic pain is the classic migration of appendicitis pain.
Clinical Correlate - Ilioinguinal and Iliohypogastric Nerve Injury: These nerves are vulnerable during appendectomy (grid-iron/Lanz incision), inguinal hernia repair, or Pfannenstiel incision. Injury causes hypo- or hyperaesthesia of the groin, scrotum/labia, and medial thigh. "Post-herniorrhaphy pain syndrome" with groin neuralgia is a recognized complication, sometimes requiring neurectomy.
Clinical Correlate - Rectus Sheath Block: The rectus sheath block deposits local anaesthetic between the posterior rectus sheath and the rectus abdominis muscle, blocking the anterior cutaneous branches of T9-T11. It provides excellent analgesia for midline incisions in laparoscopic port-site wounds and umbilical operations.
Clinical Correlate - TAP (Transversus Abdominis Plane) Block: Local anaesthetic injected into the neurovascular plane between the internal oblique and transversus abdominis muscles blocks T10-L1, providing analgesia for the lower abdominal wall. It is increasingly used in laparoscopic surgery, caesarean section, and inguinal hernia repair.
12. Inguinal Region and Groin Development
The inguinal canal forms embryologically as the testis descends from the posterior abdominal wall:
- A gubernaculum develops connecting the gonad to the labioscrotal swelling
- The processus vaginalis is a peritoneal diverticulum that precedes the testis through the abdominal wall
- The testis descends with the processus vaginalis at ~28-32 weeks gestation
- The processus vaginalis normally obliterates leaving the tunica vaginalis testis
- Failure to obliterate = patent processus vaginalis = congenital indirect inguinal hernia (or hydrocele)
In females, the ovaries descend only to the pelvic brim and never pass through the abdominal wall. Only the round ligament of the uterus passes through the inguinal canal.
Clinical Correlate - Cryptorchidism: Failure of testicular descent. The testis may remain anywhere along the line of descent (abdominal, inguinal, or ectopic). Associated with infertility, increased risk of testicular malignancy (5-10x), and torsion. Orchidopexy performed by age 18 months reduces but does not eliminate malignancy risk.
Clinical Correlate - Congenital Inguinal Hernia and Hydrocele: A patent processus vaginalis allows peritoneal fluid (hydrocele) or abdominal contents (hernia) to enter the scrotum. Communicating hydroceles change in size through the day. Hernias in infants require urgent repair due to high strangulation risk.
13. Surface Anatomy and Topographic Divisions
Planes and Regions
The abdomen is divided into 9 regions by two vertical (mid-clavicular) and two horizontal (subcostal, intertubercular) planes:
- Upper: right hypochondrium, epigastrium, left hypochondrium
- Middle: right lumbar, umbilical, left lumbar
- Lower: right iliac, hypogastrium/pubic, left iliac
Or into 4 quadrants by a vertical (midline) and a horizontal (transumbilical) plane.
Key Surface Landmarks
- McBurney's point: 1/3 of the way from ASIS to umbilicus (appendix base)
- Mid-inguinal point: midpoint between ASIS and pubic symphysis (femoral artery pulse)
- Midpoint of inguinal ligament: midpoint between ASIS and pubic tubercle (deep inguinal ring)
Clinical Correlate - McBurney's Point Tenderness: The classic site of maximal tenderness in acute appendicitis. However, the position of the appendix tip is highly variable (retrocaecal most common at 65-70%) so tenderness may be more lateral or posterior.
14. Key Special Ligaments and Structures
| Structure | Description | Clinical Relevance |
|---|---|---|
| Inguinal ligament (Poupart's) | Inferior edge of external oblique aponeurosis, ASIS to pubic tubercle | Forms the floor of the inguinal canal; key landmark in hernia classification |
| Lacunar ligament (Gimbernat's) | Medial part of inguinal ligament folding onto pectineal line | Sharp medial boundary of femoral ring; causes strangulation of femoral hernias |
| Cooper's ligament (pectineal) | Periosteum of superior pubic ramus + lacunar ligament | Used as fixation point in McVay hernia repair and laparoscopic mesh fixation |
| Iliopubic tract | Aponeurotic band parallel to inguinal ligament (deep surface) | Important in laparoscopic hernia anatomy; should not place mesh staples below this line (risk of femoral nerve injury) |
| Conjoint tendon (falx inguinalis) | Fused lower fibers of internal oblique + transversus abdominis | Reinforces posterior inguinal wall medially; used in tension repairs (Bassini) |
15. Summary Diagram of Hernia Types and Their Relationships
The diagram below summarizes the key hernia sites in the anterior abdominal wall, clearly showing where each type of inguinal and femoral hernia originates relative to the inferior epigastric vessels and pubic tubercle:
16. Clinical Correlates Summary Table
| Clinical Entity | Anatomical Basis | Key Point |
|---|---|---|
| Urinary extravasation | Scarpa's fascia fuses below inguinal ligament and with Colles' | Urine spreads onto anterior abdomen and into scrotum/perineum, NOT into thigh |
| Rectus sheath hematoma | Rupture of inferior epigastric vessel within sheath | Below arcuate line: no posterior sheath, blood spreads freely - more dangerous |
| Caput medusae | Paraumbilical vein collaterals in portal hypertension | Radiates from umbilicus; sign of portal hypertension |
| Referred appendix pain | T10 visceral afferents | Initial periumbilical pain shifting to RIF as parietal peritoneum involved |
| Indirect inguinal hernia | Patent processus vaginalis / lateral to inferior epigastric vessels | Congenital; lateral to epigastrics; can reach scrotum; strangulates |
| Direct inguinal hernia | Hesselbach's triangle weakness | Medial to inferior epigastrics; acquired; rarely strangulates; elderly |
| Femoral hernia | Femoral ring below inguinal ligament | Common in females; high strangulation rate; medial to femoral vein |
| Spigelian hernia | Defect at semilunar line | Interparietal; often occult; needs CT |
| Cremasteric reflex absence | Genitofemoral nerve / L1-L2 | Absent in testicular torsion - surgical emergency |
| Ilioinguinal nerve injury | Hernia repair / Pfannenstiel incision | Post-herniorrhaphy groin pain, numbness of scrotum/labia |
| TAP block | Neurovascular plane (IO/TA interface) | Blocks T10-L1 for lower abdominal surgery analgesia |
| Inferior epigastric injury | Trocar placement | Laparoscopic port haemorrhage; avoid by transillumination or lateral placement |
| Epigastric hernia | Linea alba defect, preperitoneal fat herniation | Small, painful midline epigastric mass |
| Diastasis recti | Linea alba widening without true defect | No true hernia sac; prominent midline ridge on Valsalva; mainly cosmetic |
Sources:
- General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy) - Sections 3.6, 3.7, 5.8
- Gray's Anatomy for Students - Chapter 4 (Abdomen), Rectus Sheath, Inguinal Canal
- Mulholland and Greenfield's Surgery, 7th ed. - Chapter 72 (Anterior Abdominal Wall, Fascial Layers, Rectus Sheath, Innervation, Blood Supply)
- Bailey and Love's Short Practice of Surgery, 28th ed. - Chapter 64 (Anatomy of the Inguinal Canal, Inguinal Hernias)
This is a shared conversation. Sign in to Orris to start your own chat.