Otalgia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Searching PubMed
otalgia referred ear pain diagnosis management
I now have comprehensive content. Let me compile the full answer.
Otalgia (Ear Pain)
Otalgia is pain perceived in or around the ear. It is classified into two fundamental types: primary (otogenic) otalgia - arising from disease within the ear itself - and secondary (referred) otalgia - arising from pathology elsewhere that shares the ear's nerve supply.
Anatomy: Why Referred Pain Occurs
The sensory innervation of the ear is supplied by four cranial nerves and two cervical nerves, making it one of the richest convergence zones in the head and neck. Any pathology residing within this sensory network can be perceived as ear pain:
| Nerve | Supplies | Remote structures served |
|---|---|---|
| CN V (Trigeminal) - auriculotemporal br. | Lateral TM, EAC, lateral pinna above meatus | Teeth, TMJ, sinuses, nasopharynx, infratemporal fossa |
| CN VII (Facial) - auricular br. | Posteroinferior TM, posteroinfo. meatal skin, concha | Geniculate ganglion, parotid |
| CN IX (Glossopharyngeal) - Jacobson's nerve | Middle ear mucosa, Eustachian tube | Oropharynx, tonsil, tongue base, posterior 1/3 tongue |
| CN X (Vagus) - Arnold's nerve | Posteroinferior EAC, pinna | Larynx, hypopharynx, oesophagus |
| C2-C3 (greater auricular + lesser occipital) | Cranial surface of pinna, lateral pinna below meatus | Cervical spine, upper neck |
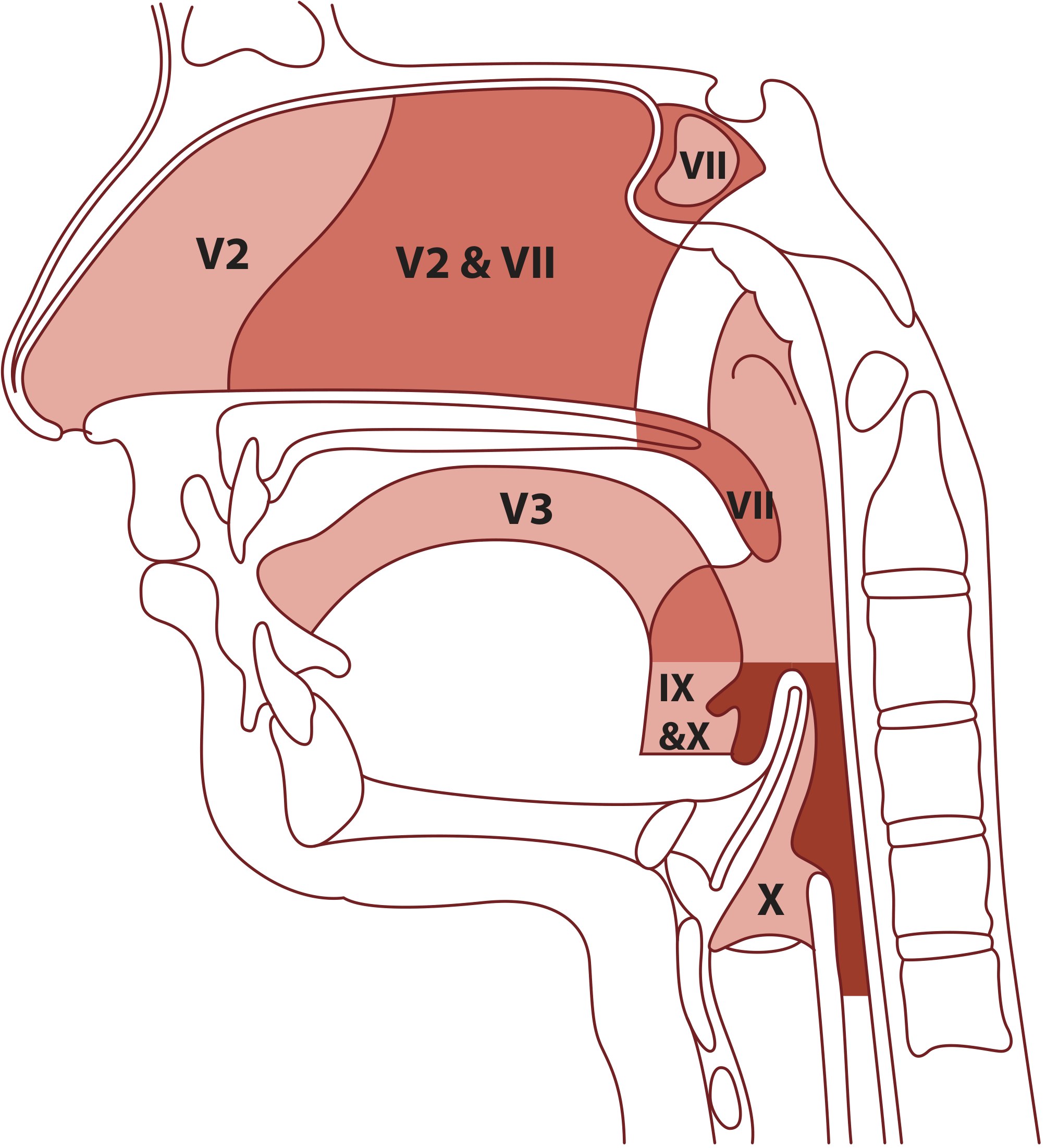
Figure: Otalgia arising from head and neck sources. Pathology in any zone innervated by CNs V, VII, IX, X or upper cervical nerves C2-C3 can refer pain to the ear. (Scott-Brown's Otorhinolaryngology, Vol. 2)
Key epidemiological point: In children, otalgia is far more frequently otogenic; in adults, referred otalgia is the more common cause. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 1185
Primary (Otogenic) Otalgia
Primary otalgia is usually accompanied by hearing loss and/or otorrhoea. The absence of these features should prompt consideration of a referred source.
Causes by site:
| Site | Conditions |
|---|---|
| Pinna | Chondrodermatitis nodularis helicis, perichondritis (chronic relapsing), trauma/haematoma, cellulitis, herpes zoster oticus, malignancy |
| External canal | Otitis externa (acute, chronic, necrotising/malignant), furuncle, bullous myringitis, keratosis obturans, canal cholesteatoma, trauma, herpes zoster oticus, malignancy |
| Middle ear | Acute otitis media (AOM), otitis media with complications, cholesteatoma, mastoiditis, malignancy |
| Inner ear | Noise discomfort (hyperacusis) |
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 1186
Referred (Secondary) Otalgia
When otoscopy is normal and there is no discharge or hearing loss, referred otalgia must be actively sought. The nerve-by-nerve framework helps structure the differential:
1. Via CN V (Trigeminal) - Dental and TMJ
Dental disorders are the most common cause of referred otalgia. This includes:
- Dental caries, abscesses, periodontal disease
- Erupting/impacted third molars (wisdom teeth)
- Post-extraction pain
- Temporomandibular joint (TMJ) dysfunction / CSDD (craniomandibular-cervical disorders):
- Bruxism, clenching, TMJ osteoarthritis, musculoskeletal pain of the muscles of mastication
- TMJ imaging may be abnormal in ~20% of asymptomatic individuals, so results must be interpreted alongside clinical findings
- First-line treatment: conservative - analgesia and physiotherapy
2. Via CN IX / CN X - Pharyngeal, Laryngeal, and Oesophageal
- Tonsillitis / peritonsillar abscess - classic, easily recognized
- Head and neck malignancy - a critical not-to-miss diagnosis:
- Oropharyngeal carcinoma (tonsil, tongue base) - referred via CN IX; may be the sole presenting symptom
- Isolated unilateral otalgia without otoscopic findings is a red flag for occult aerodigestive tract malignancy
- Hypopharyngeal and supraglottic carcinoma - otalgia and odynophagia are common presenting features via CN X (Arnold's nerve)
- Nasopharyngeal carcinoma - otalgia reported in up to 14% of cases
- Infratemporal fossa tumours (adenoid cystic carcinoma, SCC, osteogenic sarcoma) - referred via CN V, Arnold's or Jacobson's nerve
- Laryngopharyngeal reflux (LPR) - implicated in both children and adults; upper airway mucosa is more sensitive to acid damage than oesophageal epithelium, so otalgia can occur without typical reflux symptoms
3. Via CN X - Vagus (cardiac)
- Cardiac pain can present as otalgia - an important consideration in older patients
4. Via C2-C3 - Cervical
- Cervical spondylosis / musculoskeletal neck disorders
- Cervical lymphadenopathy, thyroid disease, neck masses
5. Neuralgias (diagnoses of exclusion)
- Glossopharyngeal neuralgia: Severe, transient, stabbing pain in the ear, base of tongue, tonsillar fossa, or beneath the angle of the jaw. Incidence: 0.2-0.7/100,000/year. Triggered by swallowing, coughing, yawning, or talking. Two types: tympanic (mainly ear pain) and oropharyngeal (mainly throat pain). Paroxysmal, lasting seconds to minutes, with remission periods. Often misdiagnosed due to rarity.
- Herpes zoster oticus (Ramsay Hunt syndrome): Severe acute otalgia from geniculate ganglion involvement, preceding vesicle eruption; can persist as post-herpetic neuralgia
- Trigeminal neuralgia: Otalgia is an infrequent but possible feature
- Great auricular neuralgia, carotidynia
All primary neuralgias are diagnoses of exclusion; MRI of the affected cranial nerve is indicated.
Clinical Assessment
History - key questions:
- Pain characteristics: acute vs. chronic, nociceptive vs. neuropathic
- Associated otological symptoms: hearing loss, otorrhoea, tinnitus, fullness
- Systemic red flags: dysphagia, voice change, weight loss, odynophagia, oral lesions, neck mass
- Social history: tobacco and alcohol use (aerodigestive malignancy risk)
- Dental/jaw symptoms: pain on chewing, jaw clicking, bruxism
- Prior treatments and opioid use (for chronic pain)
Physical examination:
- Full otoscopy (EAC, TM, middle ear)
- Pinna and periauricular inspection
- Cranial nerve examination
- Oral cavity, oropharynx
- Flexible nasendoscopy (pharynx, larynx, nasopharynx) - essential in unexplained otalgia
- Neck examination (lymph nodes, salivary glands, thyroid)
- TMJ and dental examination
- Cervical spine assessment
Key clinical rules (Best Practice):
- Otalgia with normal otoscopy, no discharge, and no hearing loss = presumed referred until proven otherwise
- Expert dental/TMJ examination should be part of the workup
- Full upper aerodigestive tract evaluation is mandatory in unexplained otalgia
- Isolated unilateral otalgia = red flag for occult aerodigestive malignancy
Investigation
| Indication | Investigation |
|---|---|
| Suspected malignancy | Flexible nasendoscopy + MRI/CT head and neck |
| Infratemporal fossa lesion suspected | MRI with gadolinium enhancement |
| Temporal bone pathology | CT temporal bones |
| TMJ dysfunction | Orthopantomogram (OPG), MRI TMJ |
| Neuralgia suspected | MRI of affected cranial nerve; neurology opinion |
| Cardiac otalgia | ECG, cardiac workup |
- Cummings Otolaryngology Head and Neck Surgery, p. 2635
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 1187-1189
Summary: Differential at a Glance
OTALGIA
│
├── Otoscopy ABNORMAL → Primary otalgia
│ ├── Otitis externa / furuncle / bullous myringitis
│ ├── Otitis media (AOM / chronic / with complications)
│ ├── Cholesteatoma / mastoiditis
│ ├── Herpes zoster oticus (Ramsay Hunt)
│ └── Ear canal / middle ear malignancy
│
└── Otoscopy NORMAL → Referred otalgia (work up systematically)
├── Dental / TMJ (most common in adults)
├── Oropharyngeal / tonsillar (tonsillitis, peritonsillar abscess)
├── Head and neck malignancy ⚠ (red flag)
├── Laryngeal / hypopharyngeal pathology
├── Laryngopharyngeal reflux (LPR)
├── Cervical spine disease
├── Cardiac pain ⚠
└── Neuralgias (glossopharyngeal, post-herpetic, geniculate)
→ Diagnoses of exclusion; MRI cranial nerve required
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, Chapter 92 (Otalgia), pp. 1185-1189
- Cummings Otolaryngology Head and Neck Surgery, Chapter 137, pp. 2634-2635
- Tintinalli's Emergency Medicine: A Comprehensive Study, Chapter 242, p. 966
Otalgia from book bailey and love
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the Bailey & Love content on otalgia. Let me compile the complete answer.
Otalgia - Bailey & Love's Short Practice of Surgery (28th Edition)
Sensory Nerve Supply of the Ear and Basis for Referred Otalgia
Bailey & Love grounds its discussion of otalgia in the rich, complex sensory innervation of the ear:
"This complicated and rich sensory innervation means that referred otalgia is common and may originate from the normal area of distribution of any of the above nerves. A classic example is the referred otalgia caused by cancer of the larynx or hypopharynx."
Nerves supplying the ear:
| Nerve | Region Supplied |
|---|---|
| Auriculotemporal branch of CN V (Trigeminal) | External ear |
| Greater auricular nerve (C2/3) | External ear |
| Lesser occipital nerve (C2) | External ear |
| CN VII (Facial) - small sensory branches | External ear |
| CN IX (Glossopharyngeal) | Middle ear |
| CN X (Vagus) - small sensory branches | External ear |
Summary box (Bailey & Love, Ch. 51 - Applied anatomy):
- The skin on the outer surface of the eardrum migrates outwards so the ear canal is "self-cleaning"
- Infection of the middle ear and mastoid can easily spread to the cranial cavity
- The facial nerve pursues a tortuous course through the middle ear
- The ear has a rich sensory innervation so that 'referred otalgia' is common
- Cancer of the larynx or lower pharynx can present with otalgia
History Taking in Otalgia
Bailey & Love (Table 51.1) lists the following in the history of a patient with ear symptoms:
- Earache, pain and itch
- Hearing loss
- Discharge: type, quantity and smell
- Tinnitus
- Vertigo
- Facial weakness
- Speech and development (in children)
- Past history: head injury, baro- or noise trauma, ototoxics, family history, previous ear surgery
Referred Otalgia - Specific Clinical Contexts in Bailey & Love
1. Acute Tonsillitis
"This common condition is characterised by a sore throat, fever, general malaise, dysphagia, enlarged upper cervical nodes and sometimes referred otalgia."
- ~50% bacterial (Group A Streptococcus), ~50% viral (including EBV/glandular fever)
- Throat swab + blood for EBV testing recommended
- Treatment: Paracetamol, analgesia, saline gargles, phenoxymethylpenicillin (penicillin V); ampicillin avoided (risk of rash in EBV)
2. Post-Tonsillectomy Otalgia
"Patients are allowed home on the same or following day and are warned that they may experience otalgia as a result of referred pain from the glossopharyngeal nerve..."
- Referred pain via CN IX after tonsillectomy is an expected post-operative finding
- Patients are counselled preoperatively about this
- Complications of tonsillectomy also listed as: haemorrhage (immediate or late), infection, pain/otalgia, postoperative airway obstruction, velopharyngeal insufficiency
3. Hypopharyngeal Carcinoma
"The diagnosis of hypopharyngeal carcinoma should be considered in all patients presenting with dysphagia, hoarseness or referred otalgia, particularly if they have a history of smoking or significant alcohol consumption."
- Fibreoptic endoscopy in clinic may show only subtle signs (oedema, unilateral pooling of saliva in piriform fossa)
- Not well visualised on flexible gastroscopy
- Preferred investigation: direct rigid pharyngoscopy + oesophagoscopy with biopsy under GA
- MRI or CT of neck + CT thorax/upper abdomen for staging
- Alcohol and tobacco are the two principal carcinogens (for non-HPV tumours)
4. Nasopharyngeal Carcinoma (NPC)
Listed local presenting features of NPC include:
- Hearing loss (unilateral serous otitis media)
- Otalgia
- Nasal obstruction, bloody discharge, epistaxis
- Cranial nerve palsies (especially CN III-VI then IX-XII)
- Trismus
Regional: Cervical lymphadenopathy (often the first presentation)
5. Oral Cavity Neoplasm (Late-Stage)
From Table 53.4 - Signs and Symptoms of Oral Cavity Neoplasm:
| Signs | Symptoms |
|---|---|
| Non-healing ulcer (>2 weeks) | Sensory nerve deficit |
| Persistent neck mass/lymphadenopathy | Chronic otalgia |
| Lesion with progressive increase in size | Trismus of unknown aetiology |
| Persistent red or white lesion | Dysphagia |
| Unexplained tooth mobility |
"Reduced tongue movement, sensory nerve deficit, trismus, otalgia and dysphagia are all in keeping with late-stage disease."
Key Teaching Points from Bailey & Love on Otalgia
- Referred otalgia is common due to the ear's complex multi-nerve sensory supply (CN V, VII, IX, X + cervical nerves C2/3)
- Any pathology within the distribution of these nerves can cause ear pain - this is the fundamental mechanism
- Cancer of the larynx or hypopharynx is the classic red-flag cause of referred otalgia - always consider in smokers/alcohol users presenting with ear pain + dysphagia/hoarseness
- Post-tonsillectomy otalgia via the glossopharyngeal nerve is a normal expected finding - patients must be warned
- Acute tonsillitis commonly produces referred otalgia via CN IX
- Chronic otalgia is a symptom of late-stage oral cavity malignancy
- Nasopharyngeal carcinoma can present with otalgia as part of its local symptom complex
Source: Bailey and Love's Short Practice of Surgery, 28th Edition - Chapters 51 (Ear, Nose and Throat), 52 (Head and Neck), and 53 (Head and Neck Oncology)
This is a shared conversation. Sign in to Orris to start your own chat.