Sickle cell retinopathy
Reading File
Finding Sources
Searching PubMed
"sickle cell retinopathy" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of sickle cell retinopathy based on authoritative ophthalmology textbooks.
Sickle Cell Retinopathy
Pathophysiology
Sickling haemoglobinopathies cause red blood cells to adopt an anomalous shape under physiological stress (hypoxia, acidosis), leading to vascular occlusion. The relevant genotypes are:
| Genotype | Notes |
|---|---|
| HbSC | Most likely to develop severe proliferative retinopathy |
| HbSS (sickle cell disease) | Proliferative retinopathy less common than SC |
| HbS-thalassaemia | Significant risk |
| HbSA (sickle cell trait) | Rare retinopathy; only if co-existing diabetes or inflammation |
⚠️ Carbonic anhydrase inhibitors (CAIs) are contraindicated in all sickling disorders — they precipitate sickling and vascular occlusion. This applies to IOP management in hyphaema as well.
Anterior Segment Findings
- Conjunctiva: Dark red corkscrew- or comma-shaped vessels (typically transient)
- Iris: Patches of ischaemic atrophy from pupillary edge to collarette; occasional rubeosis
- Hyphaema: May be spontaneous or post-traumatic; requires careful IOP control (avoid CAIs)
Non-Proliferative Retinopathy
| Feature | Description |
|---|---|
| Venous tortuosity | Very common; due to peripheral arteriovenous shunting |
| Optic disc sign of sickling | Dark red blots on the disc surface from small vessel occlusion |
| Salmon patches | Orange-red mid-peripheral superficial intraretinal haemorrhages; initiating event is vascular occlusion |
| Black sunbursts | Peripheral RPE hyperplasia and chorioretinal atrophy evolving from salmon patches; variable pigmentation with a pale outer band |
| Arteriolar occlusions | Branch, central, or macular vessels; "silver wiring" of peripheral arterioles = previously occluded; corkscrew vessels |
| Macular depression sign | Oval temporal macular depression from retinal thinning after arteriolar occlusion |
| Iridescent/refractile deposits | Residual deposits after haemorrhage resorption |
| Angioid streaks | Present in up to 6% |
Proliferative Retinopathy — Goldberg Staging
| Stage | Finding |
|---|---|
| 1 | Peripheral arteriolar occlusion |
| 2 | Peripheral arteriovenous anastomoses proximal to non-perfused areas |
| 3 | "Sea fan" neovascularization — at the edge of perfused retina, typically with one feeding arteriole and one draining venule |
| 4 | Vitreous haemorrhage from the NV |
| 5 | Rhegmatogenous or tractional retinal detachment |
The development of proliferative retinopathy is usually insidious and asymptomatic until stage 4 or 5.
Fundus angiography (FA) in stage 3: sea fan filling and peripheral capillary non-perfusion in early phase → leakage from NV in late phase. Wide-field imaging is particularly well-suited to evaluation.
Fundus Images
Fig. 1 — Sickle cell retinopathy: sea fan neovascularization with vitreous haemorrhage (Wills Eye Manual)
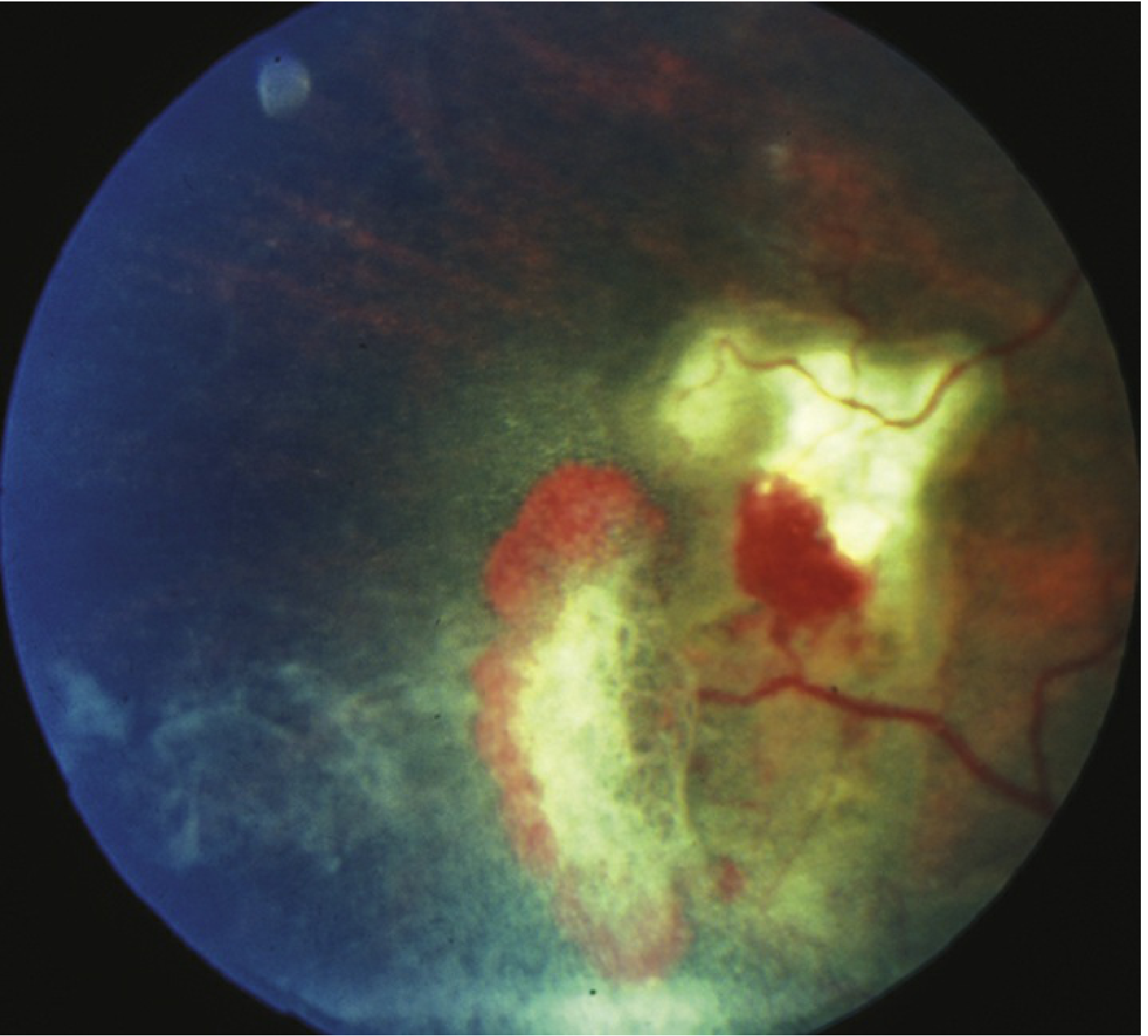
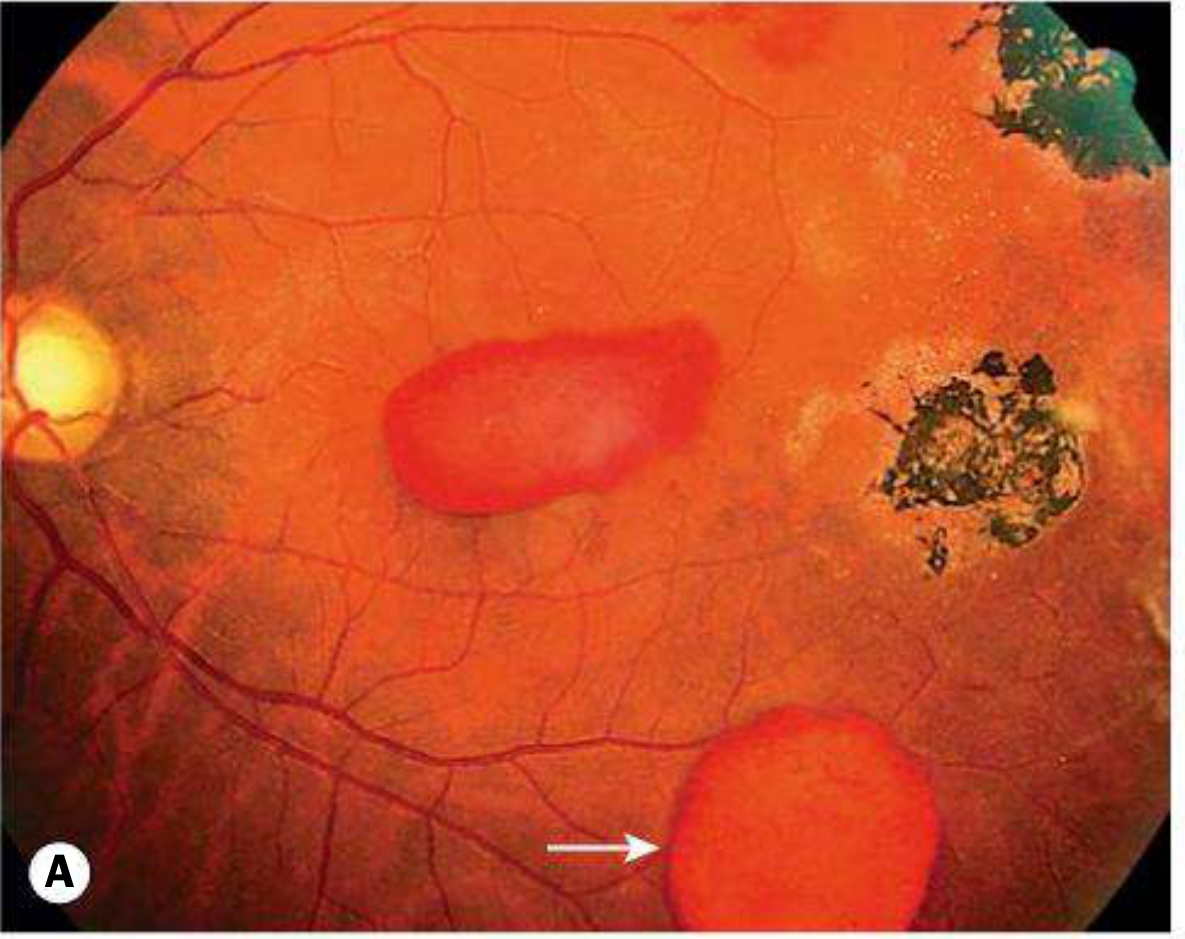
Fig. 2 — Non-proliferative sickle cell retinopathy: salmon patch haemorrhage (arrow) and black sunburst lesion (Kanski's Clinical Ophthalmology)
Differential Diagnosis of Peripheral Retinal Neovascularization
- Sarcoidosis — sea fan NV with uveitis; common in young patients of African descent
- Diabetic retinopathy — posterior pathology predominates; dot-blot haemorrhages
- Eales disease — peripheral vascular occlusion of unknown aetiology (diagnosis of exclusion)
- ROP, FEVR, pars planitis, radiation retinopathy, OIS, collagen vascular disease
- Talc retinopathy — IV drug use history; refractile particles in macular arterioles
Workup
- Full medical and family history (sickle cell disease, diabetes, IV drug use)
- Dilated fundus examination with indirect ophthalmoscopy
- Sickledex, sickle cell preparation, hemoglobin electrophoresis
- Note: HbSC and HbC disease may give a negative Sickledex — electrophoresis is needed
- Widefield IVFA — aids diagnosis and guides treatment planning
- OCT-A — emerging role in monitoring (see recent evidence below)
Treatment
| Situation | Management |
|---|---|
| Stage 3 NV, no VH | Observation acceptable — many sea fans undergo spontaneous auto-infarction; especially in middle-aged/older patients |
| NV with VH | PRP (panretinal photocoagulation) to the avascular area anterior to NV |
| Tractional/persistent VH | Vitrectomy (caution: scleral explant carries high risk of anterior segment ischaemia) |
| Anti-VEGF | May be beneficial but use caution with significant traction |
| Acute arteriolar occlusion | 100% oxygen + exchange transfusion may be considered |
Laser/cryotherapy: Ablation of peripheral non-perfused retina is the optimal approach. Ablation of feeder vessels is now rarely performed due to high rates of subsequent macular NV.
Follow-Up
| Status | Interval |
|---|---|
| No retinopathy | Annual dilated fundus exam |
| Retinopathy present | Every 3–6 months depending on severity |
Recent Evidence
A 2025 systematic review and meta-analysis (PMID: 40404974) found that OCT-angiography (OCTA) is a valuable non-invasive tool for diagnosing and monitoring sickle cell-related eye disease, supporting its use as a complement or alternative to conventional IVFA.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. | Wills Eye Manual, 8th Ed.
It's not in detail , please give from good book with explanations
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
CRVO
Finding Sources
Searching PubMed
"central retinal vein occlusion" AND treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Central Retinal Vein Occlusion (CRVO)
Detailed explanation from Kanski’s Clinical Ophthalmology, 10th ed.
1) What CRVO is and why it matters
CRVO is obstruction of central retinal venous outflow, causing venous stasis, retinal hemorrhage, edema, and variable retinal ischemia.
The two clinically important forms are:
The two clinically important forms are:
- Non-ischemic CRVO (more common, better prognosis)
- Ischemic CRVO (less common, vision-threatening, high neovascular glaucoma risk)
A third category often described is impending (partial) CRVO, a milder early presentation.
2) Impending CRVO (partial CRVO)
Kanski describes this as usually occurring in somewhat younger patients than severe CRVO.
Clinical features
- May be asymptomatic or have mild/transient blur, often worse on waking
- Mild venous dilatation/tortuosity
- Few scattered dot-blot hemorrhages
- Possible mild macular edema
Course
- Often good prognosis
- Some cases progress to ischemic CRVO
- Boundary between impending CRVO and mild non-ischemic CRVO is not always clear
Management
- Evidence base is limited
- Address systemic risk factors, avoid dehydration, optimize ocular perfusion/IOP
- Antiplatelets/anticoagulants/hemodilution have no proven benefit in routine use
3) Non-ischemic CRVO
Symptoms and signs
- Sudden, painless, unilateral vision drop
- VA impairment is variable
- RAPD absent or mild
- Fundus: diffuse venous tortuosity/dilatation in all quadrants, mild-moderate dot/blot/flame hemorrhages, mild cotton-wool spots, disc and macular edema possible
Natural history
- About one-third may convert to ischemic CRVO, often within months
- If not becoming ischemic, about half can recover to near-normal vision
- Initial VA gives prognostic clues:
- Better starting VA -> better outcomes
- Mid-range VA is less predictive
- Very poor baseline VA suggests significant ischemia
4) Ischemic CRVO
This is the severe form with major capillary non-perfusion and retinal hypoxia.
Typical presentation
- Sudden severe painless monocular vision loss
- VA often counting fingers or worse
- RAPD present
- Marked widespread hemorrhages, cotton-wool spots, disc edema/hyperemia
- FA: delayed AV transit, extensive capillary non-perfusion, leakage/staining
Major complications
- Iris/angle neovascularization and neovascular glaucoma (NVG)
- Rubeosis can develop in about half, classically around 2-4 months ("100-day glaucoma")
- Gonioscopy is important because angle NV can occur even without visible pupillary margin NV
- Macular ischemia drives poor visual outcome
Important quantitative risk marker
- More than 10 disc areas of retinal capillary non-perfusion is associated with higher neovascularization risk.
5) Imaging and investigations in CRVO
- OCT: quantifies central macular edema, monitors treatment response
- FA (fluorescein angiography): defines perfusion status, ischemic burden, leakage
- ERG: can reflect ischemia severity in some settings
- Serial anterior-segment exam (pupil margin + gonioscopy) is critical in ischemic disease surveillance
6) Treatment of CRVO complications (Kanski approach)
A) Macular edema (main treatable visual morbidity)
Current standards:
- Intravitreal anti-VEGF
- Intravitreal dexamethasone implant
Kanski trial references:
- CRUISE: ranibizumab improves VA versus sham
- COPERNICUS: aflibercept effective
- GENEVA: dexamethasone implant gives anatomic/visual gains, may need repeat treatment
- COMRADE: ranibizumab showed better VA than dexamethasone at 6 months
- SCORE: intravitreal triamcinolone can improve vision in a subset but with steroid-related risks
Clinical note from Kanski:
- Benefit is less likely in very poor baseline VA (for example, profound ischemic damage)
B) Neovascularization/NVG prevention and treatment
- Close follow-up in ischemic CRVO
- Prompt PRP when indicated for anterior/posterior segment NV
- Manage IOP/NVG per glaucoma protocols
7) Follow-up strategy
- Non-ischemic CRVO: less aggressive than ischemic CRVO; monitor for conversion to ischemia and new NV
- Patients should urgently report:
- New vision decline
- Ocular pain/redness (possible NVG)
- Follow-up intensity depends on severity and response to therapy; many cases are followed over many months to up to 18-24 months
8) Prognosis
Main determinant of chronic visual loss in CRVO:
- Persistent/chronic macular edema
- In ischemic CRVO, additionally macular ischemia + NVG lead to very poor outcomes
Rule-of-thumb prognostic relationship with initial VA:
- Good initial VA -> often remains good
- Intermediate VA -> variable
- Very poor initial VA -> recovery less likely
9) Systemic management in all RVO (including CRVO)
Kanski emphasizes:
- Control cardiovascular risk factors (BP, diabetes, lipids, smoking)
- These measures benefit systemic health and may lower recurrence risk
- Aspirin/antiplatelets are not routinely prescribed solely for RVO unless systemic indication exists
- Review estrogen-containing HRT risk individually
10) Recent evidence update (last 2 years, systematic reviews)
Recent systematic reviews exist on:
- Intravitreal dexamethasone implant long-term efficacy/safety in RVO (PMID: 39678032)
- Anti-VEGF effects on choroidal thickness in RVO (PMID: 41451105)
These are broadly consistent with anti-VEGF/steroid-based contemporary management and do not overturn the Kanski framework.
Key exam-style differentiation: non-ischemic vs ischemic CRVO
| Feature | Non-ischemic | Ischemic |
|---|---|---|
| Visual loss | Mild to moderate | Severe |
| RAPD | None/mild | Present |
| Hemorrhage/CWS burden | Less severe | Extensive |
| Capillary non-perfusion | Limited | Extensive |
| NV/NVG risk | Lower | High |
| Prognosis | Better | Poor |
If you want, I can next give you:
- a one-page viva answer for CRVO,
- a management flowchart (diagnosis -> classify -> treat -> follow-up), or
- a comparison table of CRVO vs BRVO vs ocular ischemic syndrome.
Give this as a 20 mark question
Central Retinal Vein Occlusion (CRVO)
Long answer for a 20-mark ophthalmology question
Introduction
Central retinal vein occlusion (CRVO) is a retinal vascular disorder caused by obstruction of the central retinal vein, resulting in venous congestion, retinal hemorrhages, macular edema, and variable retinal ischemia. It is an important cause of sudden painless monocular visual loss in middle-aged and elderly patients. Visual prognosis depends mainly on the degree of ischemia and development of complications such as chronic macular edema and neovascular glaucoma.
Classification
CRVO is classically divided into:
- Impending (partial) CRVO
- Non-ischemic CRVO (venous stasis type, more common)
- Ischemic CRVO (severe form with extensive capillary non-perfusion)
This classification is clinically important because prognosis and management differ significantly.
Etiopathogenesis and risk factors
The basic mechanism is thrombotic/flow-related obstruction of central retinal venous outflow at or posterior to the lamina cribrosa, producing raised venous pressure, retinal hypoxia, leakage, and edema.
Ocular risk factors
- Primary open-angle glaucoma or ocular hypertension
- Increased IOP and reduced retinal perfusion pressure
Systemic risk factors
- Hypertension
- Diabetes mellitus
- Dyslipidemia
- Smoking
- Hyperviscosity/thrombophilic states (selected cases, especially younger patients)
Clinical features
Symptoms
- Sudden, painless, unilateral blurring/loss of vision
- Severity varies:
- mild in non-ischemic CRVO
- marked in ischemic CRVO
- Some impending CRVO patients may have transient blur, often worse on waking
Signs
- Dilated tortuous retinal veins in all quadrants
- Retinal hemorrhages (dot, blot, flame-shaped)
- Cotton-wool spots
- Optic disc edema/hyperemia
- Macular edema
- Relative afferent pupillary defect (RAPD):
- absent/mild in non-ischemic
- present in ischemic
Types in detail
1) Impending CRVO
- Mild venous dilatation and tortuosity with few scattered hemorrhages
- Mild or no visual symptoms
- Prognosis often good, but some progress to ischemic CRVO
- Management is largely empirical with correction of risk factors and careful follow-up
2) Non-ischemic CRVO
- More common form
- Variable visual reduction
- Fundus changes present but less severe than ischemic type
- Around one-third may convert to ischemic CRVO, often within first few months
- Better overall visual prognosis compared with ischemic CRVO
3) Ischemic CRVO
- Severe retinal non-perfusion and hypoxia
- Marked visual loss (often counting fingers or worse)
- Extensive hemorrhages, cotton-wool spots, disc edema
- High risk of anterior segment neovascularization and neovascular glaucoma
- Worst visual prognosis due to macular ischemia and NVG
Investigations
- Visual acuity and pupillary reactions (look for RAPD)
- Slit-lamp and IOP measurement
- Dilated fundus examination
- Gonioscopy in ischemic/suspected ischemic cases (angle NV may precede obvious iris NV)
- OCT macula
- Quantifies and monitors macular edema
- Fundus fluorescein angiography (FFA)
- Demonstrates delayed venous transit, leakage, and capillary non-perfusion
-
10 disc areas of non-perfusion suggests high NV risk
- Systemic workup
- BP, blood sugar, lipid profile, CBC
- Selected thrombophilia/hyperviscosity tests in young/atypical patients
Complications
- Chronic cystoid macular edema
- Macular ischemia
- Retinal neovascularization
- Iris neovascularization (NVI) and angle neovascularization
- Neovascular glaucoma (classically around 2-4 months in ischemic CRVO)
- Vitreous hemorrhage (less common than BRVO but can occur)
- Epiretinal membrane, RPE changes, opticociliary shunts
Management
A) Ocular management
1. Macular edema (main treatable cause of visual loss)
First-line:
- Intravitreal anti-VEGF agents (ranibizumab/aflibercept/bevacizumab)
- Intravitreal dexamethasone implant in selected cases
Steroids can be effective but need monitoring for:
- IOP rise
- Cataract progression
2. Neovascularization
- Careful serial review for NVI/NVA, especially in ischemic CRVO
- Panretinal photocoagulation (PRP) when neovascularization develops
- Early treatment to prevent/treat neovascular glaucoma
3. Neovascular glaucoma
- Aggressive IOP control
- PRP and anti-VEGF as indicated
- Glaucoma procedures when needed
B) Systemic management
- Control hypertension, diabetes, and dyslipidemia
- Smoking cessation
- Correct dehydration and vascular risk profile
- Antiplatelet/anticoagulant therapy is not routine solely for CRVO unless systemic indication exists
Follow-up
Non-ischemic CRVO
- Initial follow-up in weeks to months depending on severity and edema treatment
- Watch for conversion to ischemic type
Ischemic CRVO
- Frequent follow-up during first 6 months
- Mandatory repeated iris and angle evaluation for neovascularization
Prognosis
Prognosis is largely linked to initial VA and ischemic status:
- Initial VA 6/18 or better: likely to remain good
- 6/24 to 6/60: variable course
- Worse than 6/60: poorer visual recovery
Main causes of poor final vision:
- Chronic macular edema
- Macular ischemia
- Neovascular glaucoma
Conclusion
CRVO is a major retinal vascular emergency with two biologically distinct forms: non-ischemic and ischemic. Early classification, OCT/FFA-based assessment, prompt treatment of macular edema with anti-VEGF or steroids, vigilant surveillance for neovascularization, timely PRP, and systemic risk factor control are essential to preserve vision and reduce complications.
Source: Kanski's Clinical Ophthalmology, 10th ed, retinal vascular disease chapter.
Central retinal arterial occlusion
Central Retinal Artery Occlusion (CRAO)
20-mark long answer format
Introduction
Central retinal artery occlusion (CRAO) is an ophthalmic emergency characterized by sudden, painless, severe monocular vision loss due to interruption of retinal arterial blood flow. It is the retinal equivalent of an ischemic stroke and requires urgent ocular and systemic evaluation.
Etiology and risk factors
CRAO most commonly results from embolic or thrombotic occlusion of the central retinal artery.
Major causes
- Embolic
- Carotid atherosclerotic plaque (cholesterol emboli)
- Cardiac emboli (valvular disease, atrial fibrillation)
- Thrombotic
- Local atherosclerotic disease
- Inflammatory arteritic occlusion
- Giant cell arteritis (GCA), especially in elderly
- Less common
- Hypercoagulable states
- Vasculitis, trauma, iatrogenic causes
Risk factors
- Hypertension
- Diabetes mellitus
- Dyslipidemia
- Smoking
- Carotid/cardiac vascular disease
- Advanced age
Pathophysiology
Acute arterial obstruction causes retinal ischemia, especially of inner retinal layers. Irreversible retinal injury occurs rapidly; therefore treatment window is short and visual prognosis is often poor.
Clinical features
Symptoms
- Sudden, profound, painless unilateral visual loss
- May have history of transient monocular visual loss (amaurosis fugax)
Signs
- Very poor visual acuity (often counting fingers/hand movements or worse)
- Relative afferent pupillary defect (RAPD)
- Fundus:
- Retinal whitening/opacification (ischemic edema)
- Cherry-red spot at fovea
- Attenuated retinal arteries, "box-carring"/segmentation of blood column
- Visible embolus may be seen in some cases
Variants
- Non-arteritic CRAO
- Arteritic CRAO (GCA-related; urgent steroids required)
- CRAO with cilioretinal artery sparing (better central vision possible)
- Transient CRAO
Investigations
Ocular
- Visual acuity, pupil exam (RAPD), slit lamp, IOP
- Dilated fundus examination
- OCT: inner retinal hyperreflectivity/thickening in acute phase
- FFA: delayed/absent arterial filling
Systemic and stroke workup (urgent)
- Blood pressure, glucose, lipid profile, CBC
- ESR, CRP, platelet count (especially to exclude GCA)
- Carotid Doppler/vascular imaging
- Cardiac evaluation (ECG, echocardiography as indicated)
- Neuroimaging and stroke-team referral
CRAO should be managed as a stroke-equivalent event due to high risk of concurrent/future cerebral ischemia.
Management
Immediate measures (time-critical, variable benefit)
- Urgent referral to ophthalmology + stroke services
- Ocular massage (historically used)
- Reduction of IOP (topical/oral/IV agents, anterior chamber paracentesis in selected settings)
- Carbogen/hyperventilation or rebreathing approaches historically described
- Hyperbaric oxygen may help in selected early presenters where available
Evidence for traditional ocular reperfusion maneuvers is limited, but they are sometimes attempted in very early presentation.
Thrombolysis
- Intravenous or intra-arterial thrombolysis remains center-dependent and controversial
- May be considered in selected patients presenting very early within protocolized stroke pathways
Arteritic CRAO (suspected GCA)
- Immediate high-dose systemic corticosteroids (do not delay for biopsy)
- Protects fellow eye and systemic ischemic complications
Secondary prevention
- Treat vascular risk factors aggressively
- Antiplatelet/statin as per stroke physician/cardiology guidance
- Smoking cessation and lifestyle modification
- Manage carotid/cardiac source where identified
Complications
- Permanent severe visual loss/optic atrophy
- Ocular neovascularization (less common than ischemic CRVO but possible)
- Cerebral stroke and other systemic vascular events
Prognosis
- Generally poor visual prognosis in complete CRAO
- Better outcomes in:
- Very early reperfusion
- Incomplete/transient occlusion
- CRAO with cilioretinal sparing
- Final vision depends on duration of ischemia and underlying cause
Differential diagnosis
- Ophthalmic artery occlusion
- Ischemic optic neuropathy
- Severe retinal vasospasm
- CRAO mimics causing sudden vision loss (vitreous hemorrhage, retinal detachment, optic neuritis)
Conclusion
CRAO is a true ocular emergency and a systemic vascular warning sign. Early recognition, immediate stroke-pathway activation, exclusion of giant cell arteritis, and aggressive secondary vascular prevention are the pillars of management. Even when visual recovery is limited, systemic evaluation can be life-saving.
If you want, I can also provide:
- a CRAO vs CRVO 20-mark comparison table, or
- a short note format (5 marks), or
- a recent guideline-based management algorithm.
This is a shared conversation. Sign in to Orris to start your own chat.