Type 1 hypersensitivity reaction
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks plus two excellent diagrams. Let me compile the full response.
Type I Hypersensitivity Reaction (Immediate Hypersensitivity)
Type I hypersensitivity is an IgE-mediated immune reaction that occurs within seconds to minutes of re-exposure to an antigen (allergen) in a previously sensitized individual. It is the most prevalent type of hypersensitivity and encompasses conditions like anaphylaxis, allergic asthma, allergic rhinitis (hay fever), urticaria, and atopic dermatitis.
Overview: Sequence of Events
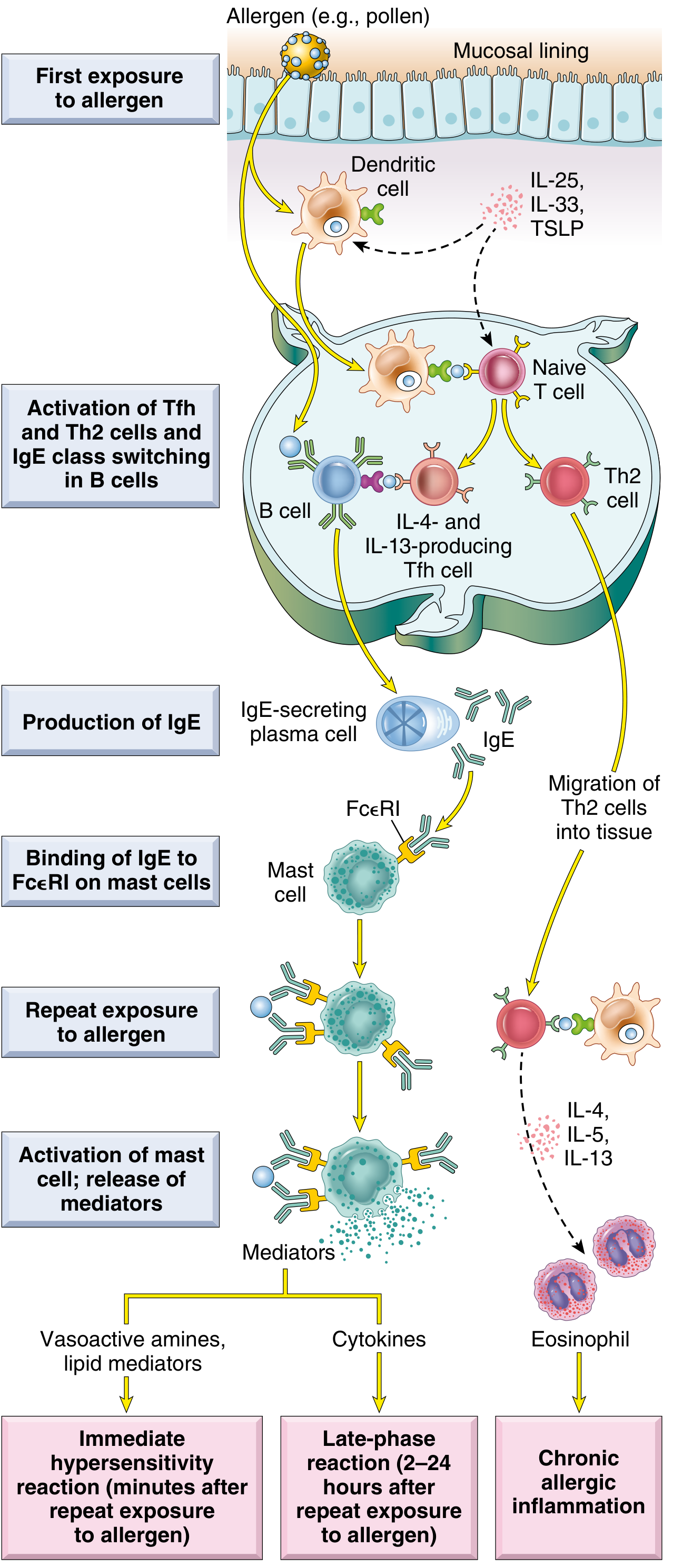
Fig. 6.14 - Robbins, Cotran & Kumar Pathologic Basis of Disease
Step 1: Sensitization Phase (First Exposure)
When an allergen (e.g., pollen, house dust mite proteins, bee venom, peanut proteins) enters the body for the first time:
- Antigen presentation: Dendritic cells process and present allergen peptides to naive CD4+ T cells. Epithelial cytokines - IL-25, IL-33, and TSLP - promote a type 2 immune environment.
- Th2 differentiation: Naive T cells differentiate into Th2 cells and T follicular helper (Tfh) cells, which produce IL-4 and IL-13.
- IgE class switching: IL-4 and IL-13 drive B cells to undergo class-switch recombination, producing allergen-specific IgE from plasma cells.
- Mast cell sensitization: IgE binds via its Fc portion to high-affinity FcεRI receptors on mast cells and basophils. These IgE-coated cells are now "sensitized" and ready to react.
- Cellular and Molecular Immunology, p. 1303-1307
Key point: No clinical symptoms occur at this stage. The individual has no adverse reaction on first exposure (with rare exceptions).
Step 2: Elicitation Phase (Re-exposure - "Challenge")
On re-exposure to the same allergen:
- The allergen (being multivalent) cross-links adjacent IgE antibodies on the mast cell surface.
- This brings the underlying FcεRI receptors together, triggering intracellular signal transduction cascades.
- The result: mast cell activation and degranulation - release of preformed and newly synthesized mediators.
"IgE-coated mast cells are said to be sensitized because they react to subsequent encounters with antigen. If the antigen is multivalent, it binds to and cross-links adjacent IgE antibodies, bringing the underlying Fce receptors together." - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 200
Mast Cell Mediators
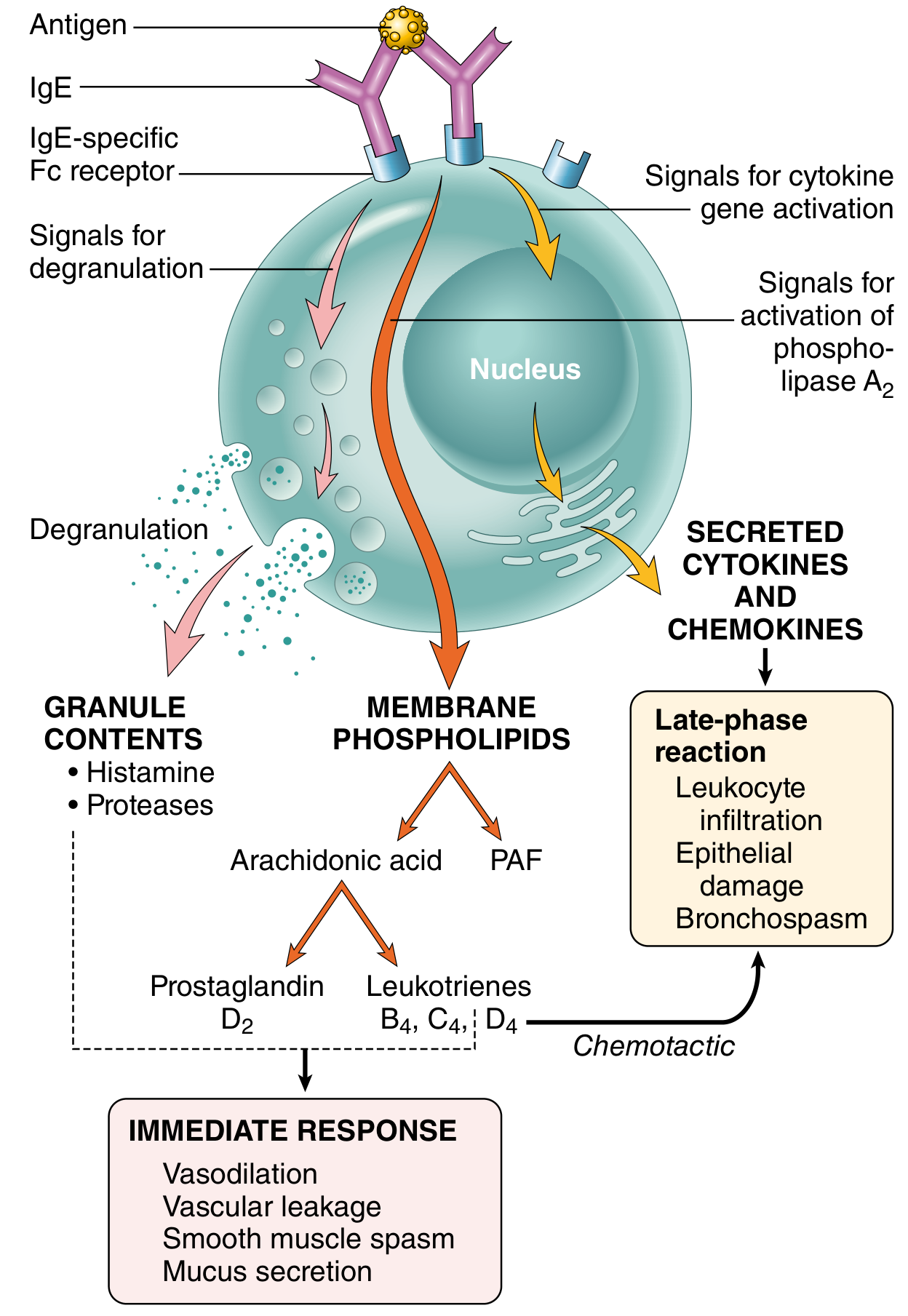
Fig. 6.15 - Robbins, Cotran & Kumar Pathologic Basis of Disease
A. Preformed Granule Mediators (Released within seconds)
| Mediator | Action |
|---|---|
| Histamine | Vasodilation, increased vascular permeability, smooth muscle contraction, mucus secretion |
| Tryptase / Chymase (neutral proteases) | Tissue damage; generate kinins and C3a from precursors |
| Heparin / Chondroitin sulfate (proteoglycans) | Package and store amines in granules; anticoagulant |
| Serotonin | Vasoactive effects |
Plasma histamine peaks ~10 minutes after anaphylaxis onset; returns to normal within 1 hour. Serum tryptase is elevated in anaphylaxis (and chronically elevated in systemic mastocytosis). Urinary histamine may remain elevated for 24 hours. - Quick Compendium of Clinical Pathology
B. Newly Synthesized Lipid Mediators (Produced within minutes)
Mast cell activation triggers phospholipase A2, converting membrane phospholipids to arachidonic acid, which feeds two pathways:
-
Cyclooxygenase pathway → Prostaglandin D2 (PGD2): Most abundant mast cell cyclooxygenase product; causes intense bronchospasm and increases mucus secretion.
-
5-Lipoxygenase pathway → Leukotrienes:
- LTC4 and LTD4: Most potent vasoactive and spasmogenic agents known; thousands of times more active than histamine on a molar basis in causing bronchospasm and increasing vascular permeability.
- LTB4: Highly chemotactic for neutrophils, eosinophils, and monocytes.
-
Platelet-activating factor (PAF): Derived directly from membrane phospholipids; contributes to vascular and bronchospastic effects.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 200-201
C. Cytokines (Produced over hours)
| Cytokine | Role |
|---|---|
| TNF, IL-1, chemokines | Promote leukocyte recruitment (late-phase reaction) |
| IL-4 | Amplifies Th2 response |
| IL-5 | Most potent eosinophil-activating cytokine |
Phase Breakdown: Immediate vs. Late-Phase Reaction
Immediate Reaction (seconds to ~1 hour)
- Driven by histamine, LTC4, LTD4, PGD2
- Manifestations: vasodilation, vascular leakage, smooth muscle spasm, mucus secretion
- Clinically: bronchospasm, urticaria, rhinorrhea, anaphylaxis
Late-Phase Reaction (2-24 hours after allergen exposure)
-
Leukocytes (especially eosinophils) are recruited by eotaxin and mast cell-derived chemokines.
-
IL-5 from Th2 cells activates eosinophils, which release:
- Proteolytic enzymes
- Major basic protein (MBP) and eosinophil cationic protein - cause tissue damage
- Galectin-10 - forms Charcot-Leyden crystals (seen in sputum of asthmatics)
-
The late-phase reaction is a major driver of symptoms in asthma - this is why antihistamines alone are insufficient for asthma; corticosteroids are required.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 201
Atopy and Genetic Predisposition
Atopy = hereditary predisposition to mount IgE responses against common environmental antigens. Features:
- Elevated serum IgE levels
- More IL-4-producing Th2 cells than general population
- Positive family history in ~50% of atopic individuals
- Genetic linkage to polymorphisms in IL-3, IL-4, IL-5, IL-9, IL-13, GM-CSF genes, and HLA loci on chromosome 6
- The atopic triad (atopic march): atopic dermatitis (infancy) → allergic rhinitis → asthma (childhood)
"A positive family history of allergy is found in almost 50% of atopic individuals." - Robbins, Cotran & Kumar Pathologic Basis of Disease
Nature of Allergens
Allergens are typically proteins or chemicals bound to proteins (e.g., pollen, house dust mite proteins, animal dander, shellfish, peanuts, penicillin as a hapten). Characteristics:
-
Molecular weight: 5-70 kD
-
Stable, glycosylated, soluble in body fluids
-
Many are enzymes (e.g., cysteine protease of house dust mite, PLA2 in bee venom)
-
T cell-independent antigens (polysaccharides) cannot elicit type I reactions unless protein-conjugated
-
Cellular and Molecular Immunology, p. 1306
Clinical Manifestations
| Form | Manifestation |
|---|---|
| Systemic anaphylaxis | Bronchospasm, cardiovascular collapse, shock - potentially fatal |
| Atopic asthma | Bronchospasm, mucus hypersecretion, airway inflammation |
| Allergic rhinitis (hay fever) | Sneezing, rhinorrhea, nasal congestion |
| Urticaria / Angioedema | Whealing, swelling |
| Atopic dermatitis (eczema) | Skin inflammation |
| Food allergy | GI symptoms (abdominal pain, diarrhea), systemic anaphylaxis |
"In the most extreme systemic form, called anaphylaxis, mast cell-derived mediators can restrict airways to the point of asphyxiation and produce cardiovascular collapse leading to shock, which together may result in death." - Cellular and Molecular Immunology, p. 1303
Non-IgE-Mediated (Nonatopic) Triggers
About 20-30% of immediate hypersensitivity reactions are not IgE-mediated and do not involve Th2 cells. Triggers include:
- Temperature extremes (heat, cold)
- Exercise
- Drugs (codeine, morphine, contrast media)
- Complement anaphylatoxins (C3a, C5a)
- Bee venom components (melittin)
These are termed anaphylactoid reactions and are clinically indistinguishable from true anaphylaxis.
Note: Anaphylactoid reactions and hereditary angioedema are NOT classified as Type I hypersensitivity reactions. - Quick Compendium of Clinical Pathology
Diagnosis
| Test | Details |
|---|---|
| Skin prick test | Measures specific IgE attached to skin mast cells; most convenient and specific screening method |
| Serum specific IgE (sIgE) | Safer alternative (no risk of anaphylaxis); valid from 6 weeks of age; preferred in cardiovascular disease or severe sensitivity |
| Serum tryptase | Elevated in acute anaphylaxis; chronically elevated in mastocytosis |
| Plasma histamine | Peaks ~10 min; returns to normal within 1 hour |
| Urinary histamine | Elevated for up to 24 hours post-reaction |
- Tietz Textbook of Laboratory Medicine, p. 3972
Treatment
| Approach | Rationale |
|---|---|
| Epinephrine (adrenaline) | First-line for anaphylaxis; reverses bronchospasm and cardiovascular collapse |
| Antihistamines (H1 blockers) | Effective for rhinitis and urticaria (immediate reaction only); insufficient for asthma |
| Corticosteroids | Target late-phase reaction; required for asthma management |
| Leukotriene receptor antagonists | Block LTC4/LTD4 effects (e.g., montelukast for asthma) |
| Allergen avoidance | Best long-term prevention |
| Allergen immunotherapy (desensitization) | Repeated low-dose allergen exposure to induce tolerance; shifts IgG/IgA response, reduces IgE |
| Anti-IgE (Omalizumab) | Biologic that binds free IgE, reducing mast cell sensitization |
"The best prevention relies on the identification of the antigen (detected by skin test or IgE antibody serology) and subsequent avoidance." - Jawetz, Melnick & Adelberg's Medical Microbiology
Th2 Cytokines and Their Role
| Cytokine | Source | Role in Type I Hypersensitivity |
|---|---|---|
| IL-4 | Th2, Tfh cells | IgE class switching in B cells; Th2 amplification |
| IL-13 | Th2 cells | IgE class switching; mucus production |
| IL-5 | Th2 cells | Eosinophil activation and recruitment |
| IL-10 | Regulatory | Anti-inflammatory; modulates allergic response |
Th2-type responses are associated with promotion of IgE and eosinophilic responses in atopy - Tietz Textbook of Laboratory Medicine
Summary
Type I hypersensitivity is a two-phase process:
- Sensitization: First allergen exposure → Th2/IgE production → mast cell sensitization (no symptoms)
- Elicitation: Re-exposure → IgE cross-linking → mast cell degranulation → immediate reaction (histamine, leukotrienes) + late-phase reaction (eosinophils, cytokines)
The central players are IgE, mast cells, and Th2 cytokines (especially IL-4, IL-5, IL-13). The reaction can range from trivial (mild rhinitis) to fatal (anaphylactic shock).
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Cellular and Molecular Immunology (Abbas et al.) | Jawetz, Melnick & Adelberg's Medical Microbiology | Tietz Textbook of Laboratory Medicine | Quick Compendium of Clinical Pathology
This is a shared conversation. Sign in to Orris to start your own chat.