Difference between TIVA and TCI for My MD Anaesthesiology exam
Reading File
Finding Sources
Finding Sources
Searching the Web
TIVA vs TCI anaesthesia difference MD exam pharmacokinetics pharmacodynamics
Finding Sources
Finding Sources
Reading Web Page
https://partone.litfl.com/tiva-and-tci.html
Reading File
Reading File
I now have comprehensive material to write an exam-focused answer. Let me compile the full detailed response.
TIVA vs TCI - MD Anaesthesiology Exam Notes
1. Definitions
| TIVA | TCI | |
|---|---|---|
| Full form | Total IntraVenous Anaesthesia | Target Controlled Infusion |
| Definition | A technique in which ALL anaesthetic agents (hypnotic + analgesic + relaxant) are given intravenously, with NO volatile agents | A method of drug delivery that uses a microprocessor and pharmacokinetic (PK) model to achieve and maintain a clinician-specified target drug concentration in a body compartment |
| Key concept | Describes the route of administration | Describes the mode of infusion (PK-controlled) |
| Relationship | TIVA can be performed with or without TCI; TCI is the most precise way to deliver TIVA | TCI is a subset/tool within TIVA |
Important exam point: TCI is NOT synonymous with TIVA. TIVA is a broader concept (all IV anaesthesia). TCI is a delivery method that can be used to achieve TIVA. You can have TIVA without TCI (manual infusion), but TCI in anaesthesia is almost always used as part of TIVA.
2. TIVA - Manual (Non-TCI)
Mechanism
- The anaesthetist manually calculates the drug doses based on body weight (mg/kg) and time
- No real-time knowledge of predicted plasma concentration
- Based on empirical "bolus + infusion" regimens
Classic Propofol Regimen (Roberts 10-8-6 / Bristol model)
- Induction: 1-2 mg/kg IV bolus
- Maintenance: 10 mg/kg/hr for first 10 min → 8 mg/kg/hr for next 10 min → 6 mg/kg/hr thereafter
- This stepwise reduction accounts for peripheral redistribution (tissues becoming saturated over time)
Classic Remifentanil regimen (TIVA)
- 0.25-0.5 mcg/kg/min infusion (constant, because remifentanil does NOT accumulate)
Drawback
- Does not account for individual PK variability
- Risk of drug accumulation with longer cases
- No real-time concentration estimate available
3. TCI - Target Controlled Infusion
Mechanism
TCI uses multicompartment PK models (typically a 3-compartment model) loaded into a microprocessor-controlled pump. The clinician sets a target concentration (plasma Cp or effect-site Ce), and the pump:
- Calculates the current estimated drug concentration
- Adjusts infusion rate in real-time to achieve and maintain that target
- Accounts for elimination, metabolism, redistribution, and accumulation
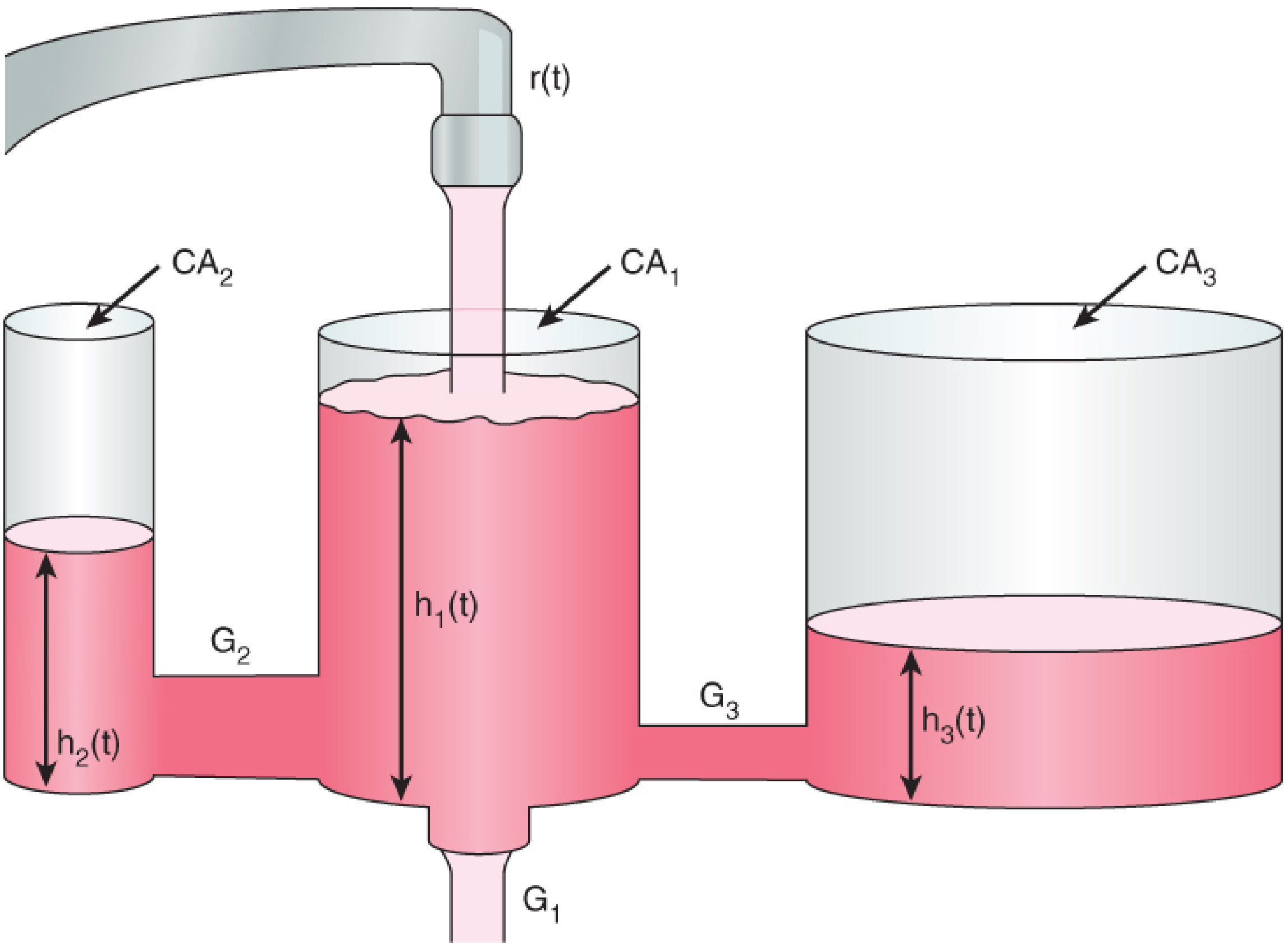
The Three-Compartment Model (basis of TCI)
- Compartment 1 (Central): Blood/plasma - where drug is injected and measured
- Compartment 2 (Rapid peripheral): Well-perfused tissues (muscle, gut)
- Compartment 3 (Slow peripheral): Poorly-perfused tissues (fat)
- Effect compartment (Ce): Biophase - the actual site of drug action (brain). Has a rate constant keo
Targeting: Plasma (Cp) vs Effect-site (Ce)
| Plasma targeting (Cp) | Effect-site targeting (Ce) | |
|---|---|---|
| What is targeted | Drug concentration in blood | Drug concentration at the brain (biophase) |
| Behavior at induction | Target must be deliberately set higher to achieve faster Ce rise; risk of overshoot | Pump auto-overshoots Cp to rapidly drive Ce up - no need to adjust target |
| Steady state | Cp and Ce eventually equilibrate (there is a lag - hysteresis) | More directly correlates with clinical effect |
| Preferred for | Less experienced users; safer in hemodynamically unstable | Preferred clinically; smoother induction |
Hysteresis: The delay between peak plasma concentration and peak effect-site (brain) concentration, because drug must cross the blood-brain barrier.
4. TCI Models for Propofol
Marsh Model
- Based on a 3-compartment model in healthy adults
- Covariates: weight only (does NOT factor age)
- Targets plasma concentration (Cp) by default
- Has a variable, larger V1 (central volume) → gives a larger initial bolus → faster induction
- Modified Marsh uses keo = 1.2 min⁻¹ (vs original 0.26 min⁻¹) for faster Ce equilibration
Schnider Model
- Based on a 3-compartment model with fixed V1 = 4.27 L (fixed central compartment)
- Covariates: weight, age, height, and lean body mass (LBM)
- Targets effect-site concentration (Ce) by default
- V2 and keo are variable (age-dependent)
- Overall uses less propofol and has fewer adverse events
- Limits BMI: < 42 (males), < 35 (females) to prevent absurd LBM calculations
| Feature | Marsh | Schnider |
|---|---|---|
| V1 | Variable (larger) | Fixed 4.27 L |
| Covariates | Weight only | Weight, age, height, LBM |
| Default target | Plasma Cp | Effect-site Ce |
| Induction | Faster (larger V1, larger bolus) | Slower, more controlled |
| Drug use | More propofol | Less total propofol |
| Age adjustment | No | Yes |
Bristol (Manual) Model
- The original first PK model
- Assumes premedication, fentanyl 3 mcg/kg, N₂O
- Target Cp = 3 mcg/mL
- Not a TCI pump model - it's the basis for the manual 10-8-6 regimen
5. TCI Models for Opioids
Remifentanil - Minto Model
- Covariates: age, weight, height, LBM
- Works well in both adults and children (very predictable PK, ester hydrolysis clearance)
- Context-sensitive half-time (CSHT) is constant ~3-4 min regardless of infusion duration
Alfentanil - Maitre & Scott Models
- Available on commercial TCI pumps
- Covariates: weight, age, sex
6. Key Pharmacokinetic Concepts (Exam Must-Knows)
Context-Sensitive Half-Time (CSHT)
- Time for plasma concentration to fall by 50% after stopping an infusion of specified duration
- NOT the same as elimination half-life
- Remifentanil: CSHT ~3-4 min (constant, regardless of duration) - ideal for TIVA
- Fentanyl: CSHT rises dramatically with infusion duration (up to 300 min after 8 hr infusion) - NOT ideal for TIVA
- Propofol: Intermediate - CSHT rises modestly
This is why remifentanil + propofol is the gold standard TIVA combination.
Biophase / Effect Compartment
- The theoretical compartment representing the site of drug action (brain/CNS)
- Ke0 = rate constant for drug equilibration between plasma and effect site
- High Ke0 = faster equilibration (e.g. remifentanil Ke0 ~1.0 min⁻¹)
- Lower Ke0 = slower equilibration (e.g. propofol Ke0 ~0.26-1.2 min⁻¹)
7. Head-to-Head Comparison Table
| Parameter | TIVA (Manual) | TCI |
|---|---|---|
| Basis of dosing | Body weight (mg/kg), empirical | PK model (3-compartment), targets concentration |
| What clinician sets | Infusion rate (mL/hr or mg/kg/hr) | Target concentration (mcg/mL or ng/mL) |
| Real-time Cp/Ce estimate | No | Yes (predicted) |
| Drug accumulation risk | Higher (no auto-correction) | Lower (algorithm corrects continuously) |
| Titration | Manual - requires calculation | Automated - pump adjusts rates |
| Induction | Bolus + start infusion | Pump gives auto-calculated loading bolus |
| Equipment needed | Standard syringe pump | Dedicated TCI pump with PK software |
| Operator skill | Higher (manual calculation needed) | Lower (algorithm does the work) |
| Accuracy | Less (population PK assumptions) | Better but still uses population models |
| Awareness risk | Higher (variable concentrations) | Lower (more stable concentrations) |
| Cost | Lower | Higher |
| Paediatrics | Standard (most children get this) | Limited (adult models valid >16 yr, >30 kg) |
8. Sources of Error in TCI (Exam Favourite)
- Incorrect patient data entry - wrong weight, age, height → wrong model output
- Wrong PK model selected for a given patient population
- Individual PK variability - population models ≠ individual patient
- Failure to account for co-medications (opioids reduce propofol requirement by ~30-50%)
- Hardware errors - syringe size mismatch, infusion line disconnection
- IV line issues - leaks, partial occlusion, extravasation
- No real-time blood concentration measurement - all values are estimated/predicted
9. Indications / When to Use Which
Prefer TCI when:
- Long cases (benefit of accumulation management)
- High-risk patients needing precise titration
- Neuromuscular blocking agents used (pEEG + TCI)
- Trained operator with TCI pump available
Prefer manual TIVA when:
- Paediatrics (no validated TCI model <16 yr / <30 kg for propofol)
- Resource-limited settings
- Short procedures
- No TCI pump available
10. TIVA vs Volatile Anaesthesia (Bonus - Often Asked Together)
| Feature | TIVA | Volatile |
|---|---|---|
| PONV | Much lower | Higher |
| Environment | No pollution | Theatre/gas pollution |
| Awareness | Slightly higher risk | Lower |
| ICP/CBF | Lower (propofol reduces CBF) | May increase (esp. >1 MAC) |
| Malignant hyperthermia | Safe | Triggers MH |
| Recovery | Faster with remifentanil | Variable |
| TIVA monitoring (Expired concentration) | Not measurable | Direct (agent analyser) |
Key Exam Summary (Mnemonics)
- TIVA = Route (all IV); TCI = Method (PK-controlled infusion)
- TCI needs: 3-compartment model + microprocessor pump + target setting (Cp or Ce)
- Marsh = Marsh = Mass (weight only); Schnider = Schnider = Six covariates (weight, age, height, LBM + fixed V1)
- Best TIVA drug pair: Propofol + Remifentanil (shortest/most predictable CSHT)
- pEEG monitoring is mandatory when NMBDs are used with TIVA
Sources: Miller's Anesthesia 10e (p. 3104-3108); Barash's Clinical Anesthesia 9e (p. 1466-1468); LITFL Part One ANZCA Exam Notes; UKZN FCA Part I Pharmacology of TIVA and TCI (2016)
This is a shared conversation. Sign in to Orris to start your own chat.