Ecg format 10 disease
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Here is the complete ECG guide for 10 diseases, sourced from Rosen's Emergency Medicine, Harrison's, Goldman-Cecil, Braunwald's Heart Disease, and other authoritative textbooks:
ECG Patterns in 10 Diseases
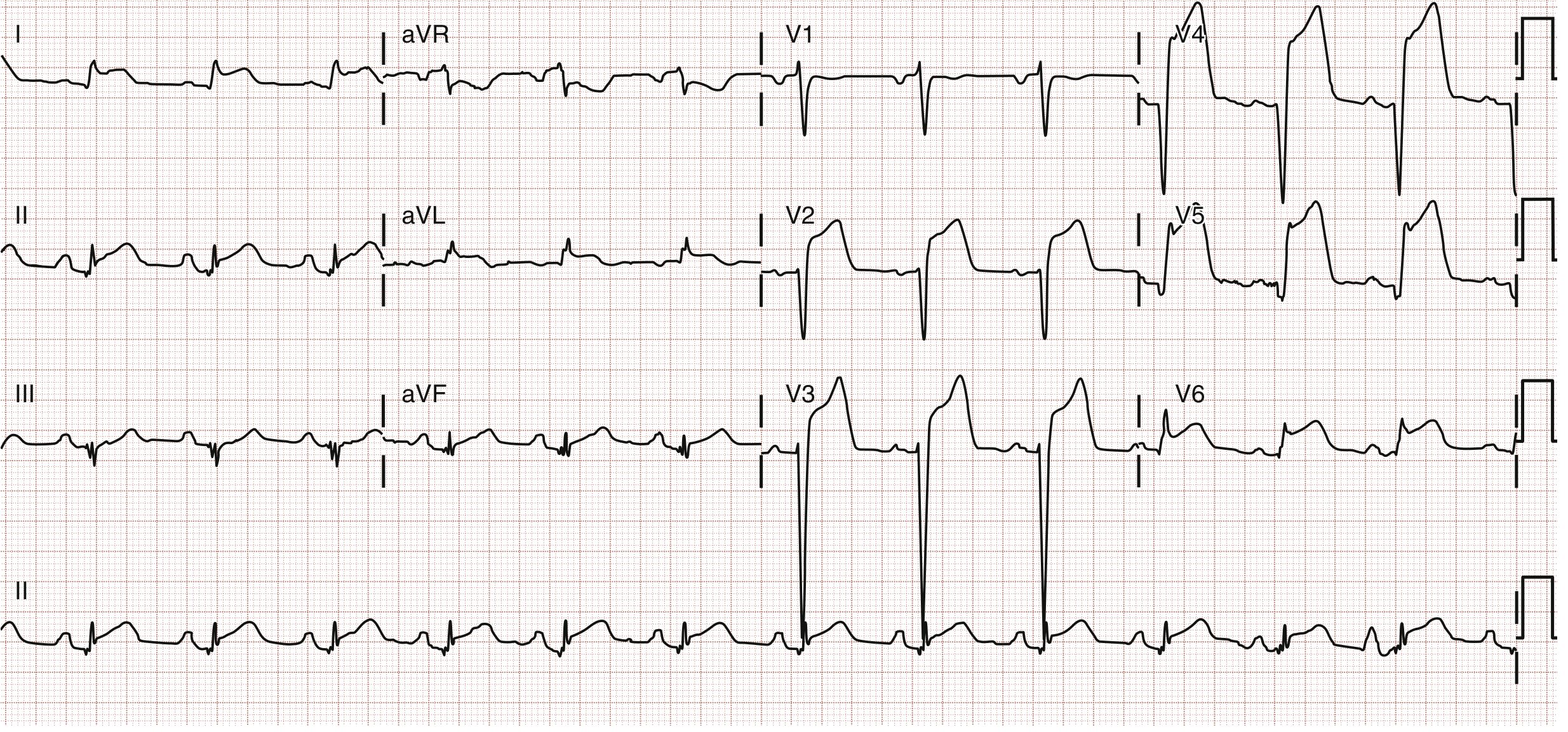
1. STEMI (ST-Elevation Myocardial Infarction)
Anterior STEMI - ST elevation in V1-V4 (LAD territory):
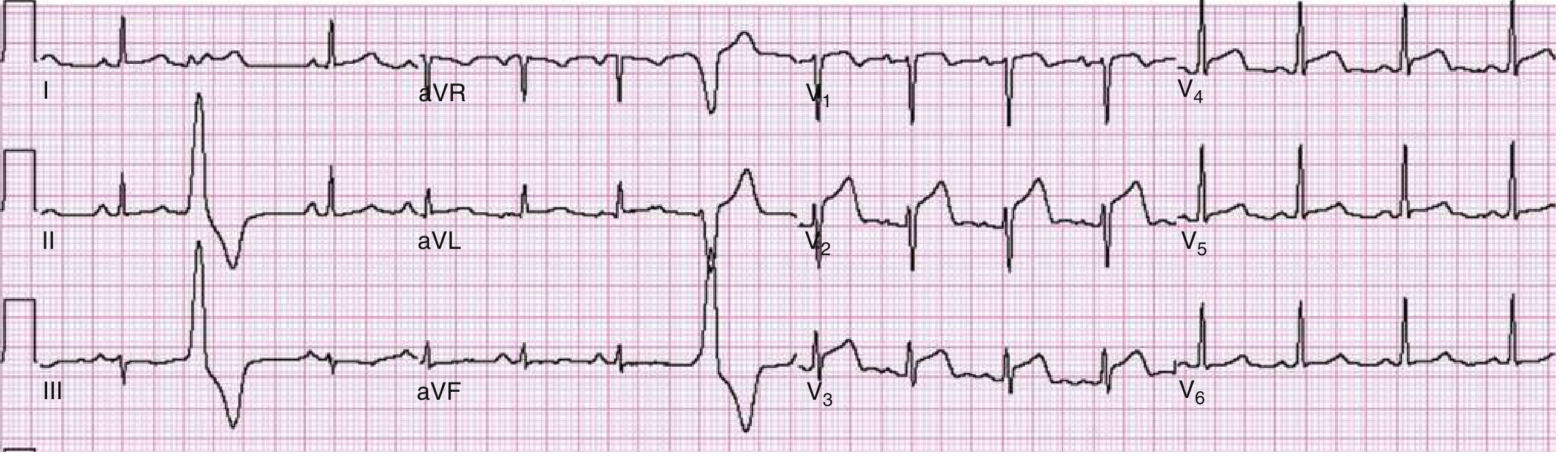
Anterolateral STEMI - ST elevation in V2-V6, I, aVL:
| Territory | Leads with STE | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA / LCx |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | V7-V9 (ST depression V1-V3) | RCA / LCx |
| RV | V3R-V4R | Proximal RCA |
Key features:
- ST elevation (obliquely straight or convex morphology) ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in precordial leads
- Reciprocal ST depression in opposite leads
- Subsequent T-wave inversion and Q-wave formation
- aVR elevation >0.5 mV suggests left main disease (78% sensitive, 83% specific)
- De Winter pattern: J-point depression + prominent T waves in precordials + STE in aVR - indicates proximal LAD occlusion
- Rosen's Emergency Medicine, block 11
2. Left Bundle Branch Block (LBBB)
| Feature | Finding |
|---|---|
| QRS duration | >120 ms (broad) |
| V5/V6 pattern | Broad, notched R wave (M-shape - "plateau") |
| V1 pattern | Deep, broad QS or rS complex |
| Lateral leads (I, V5-V6) | Upright T waves expected (discordant T is abnormal) |
| Septal Q waves | Absent in I, V5-V6 |
New LBBB in the right clinical context is treated as STEMI equivalent. Sgarbossa criteria help identify AMI superimposed on LBBB:
- Concordant ST elevation ≥1 mm in any lead (5 points)
- Concordant ST depression ≥1 mm in V1-V3 (3 points)
- Discordant STE ≥5 mm (2 points) - score ≥3 = AMI
Right Bundle Branch Block (RBBB) features:
- QRS >120 ms
- rSR' ("rabbit ears" / M-shape) in V1
- Wide S wave in I and V6
- ST-T changes discordant with terminal QRS deflection
- Goldman-Cecil Medicine, block 6; Morgan & Mikhail's Clinical Anesthesiology, block 3
3. Atrial Fibrillation (AF)
| Feature | Finding |
|---|---|
| P waves | Absent - replaced by irregular fibrillatory baseline (f-waves) |
| RR intervals | Irregularly irregular |
| QRS morphology | Usually narrow (unless aberrant conduction or WPW) |
| Ventricular rate | Variable (60-200 bpm uncontrolled) |
- No identifiable repeating P-wave morphology
- Baseline shows fine or coarse fibrillatory waves (350-600/min)
- In WPW + AF: rapid, irregular, wide-complex rhythm (pre-excited AF) - life-threatening if rate >200 bpm
- Tintinalli's Emergency Medicine
4. Wolff-Parkinson-White (WPW) Syndrome
The ECG triad during sinus rhythm:
| Feature | Finding |
|---|---|
| PR interval | <120 ms (short) |
| Delta wave | Slurred upstroke on QRS onset |
| QRS duration | >120 ms (broadened by delta wave) |
- Delta wave represents early ventricular activation via the accessory pathway (Bundle of Kent)
- Secondary ST-T changes (discordant to delta wave direction)
- Pseudo-infarct Q waves may occur (mimics inferior or lateral MI)
- Type A WPW: Positive delta waves in V1 (left-sided pathway)
- Type B WPW: Negative delta waves in V1 (right-sided pathway)
- During AVRT: narrow complex tachycardia most common (orthodromic - down AV node, up accessory pathway)
- Tintinalli's Emergency Medicine, block 11
5. Hyperkalaemia
ECG changes progress with rising K⁺ level (Harrison's Principles, 2025):
| Serum K⁺ | ECG Change |
|---|---|
| 5.5-6.5 mM | Tall, peaked (tented), symmetric T waves; shortened QT |
| 6.5-7.5 mM | Loss of P waves; PR prolongation |
| 7.0-8.0 mM | Widened QRS complex |
| >8.0 mM | Sine wave pattern, VF, asystole |
- T waves are narrow-based, symmetric, tall - best seen in precordial leads
- "Sine wave" morphology = impending cardiac arrest
- Treatment: IV calcium gluconate first (membrane stabilization), then insulin/dextrose, sodium bicarbonate, salbutamol
- Harrison's Principles of Internal Medicine 22E, block 6; Miller's Anesthesia, block 12
6. Left Ventricular Hypertrophy (LVH)
Voltage criteria (any one sufficient):
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- R in aVL ≥11 mm
Associated features (increase specificity):
- ST depression + T-wave inversion in lateral leads (V5-V6, I, aVL) = "strain pattern"
- Left axis deviation
- Broad, notched P wave in II (P mitrale) - left atrial enlargement
- Deep S in V1-V2
7. Pulmonary Embolism (PE)
ECG changes reflect acute right heart strain - seen in massive/submassive PE:
| Feature | Significance |
|---|---|
| Sinus tachycardia | Most common finding (~44%) |
| S1Q3T3 | S wave in lead I + Q wave in III + T inversion in III |
| New RBBB | Right ventricular pressure overload |
| Right axis deviation | Acute cor pulmonale |
| P pulmonale | Tall P in II (>2.5 mm) - right atrial strain |
| T-wave inversion V1-V4 | Right ventricular strain |
| ST elevation aVR | Severe RV ischemia |
- S1Q3T3 pattern is classic but only present in ~20% of cases - not sensitive
- Sinus tachycardia is the most common ECG finding
- Normal ECG does not rule out PE
- Creasy & Resnik's Maternal-Fetal Medicine, block 14
8. Complete Heart Block (Third-Degree AV Block)
| Feature | Finding |
|---|---|
| P waves | Present at their own rate (atrial rate, e.g. 70-90 bpm) |
| QRS | Present at slower rate (escape rate 30-60 bpm) |
| PR interval | Completely variable - no relationship between P and QRS |
| QRS morphology | Wide (if ventricular escape) or narrow (if junctional escape) |
- Complete AV dissociation: atria and ventricles beat independently
- Atrial rate always faster than ventricular rate
- Escape QRS morphology indicates the escape pacemaker site:
- Junctional (narrow) escape ~40-60 bpm
- Ventricular (wide) escape ~20-40 bpm - less reliable
- Clinical presentation: bradycardia, syncope, heart failure, hypotension
- Braunwald's Heart Disease, block 8; Goldman-Cecil Medicine, block 6
9. Acute Pericarditis
ECG evolves through 4 classic stages:
| Stage | Timing | ECG Change |
|---|---|---|
| Stage 1 | Days 1-2 | Diffuse concave ST elevation (saddle-shaped) + PR depression - all leads except aVR, V1 |
| Stage 2 | 1-2 weeks | ST returns to baseline; T waves flatten |
| Stage 3 | Weeks | T-wave inversion (diffuse) |
| Stage 4 | Weeks-months | Normalization |
Key distinguishing features from STEMI:
- ST elevation is concave (saddle-shaped) in pericarditis vs. convex in STEMI
- PR segment depression (pathognomonic when present) - best seen in II, V5-V6
- Diffuse (multi-lead, multi-territory) elevation rather than territorial
- No reciprocal ST depression (except aVR and V1 show ST elevation + PR depression)
- No Q waves
- Rosen's Emergency Medicine, block 12
10. Long QT Syndrome
QTc measurement:
- QTc = QT / √RR interval (Bazett's formula)
- Normal QTc: <440 ms (men), <460 ms (women)
- Prolonged: >450 ms (men), >470 ms (women)
- High risk for TdP: >500 ms
| Type | Cause | T-wave morphology |
|---|---|---|
| LQT1 (KCNQ1) | Congenital (autosomal dominant) | Broad-based T wave |
| LQT2 (HERG) | Congenital / drug-induced | Notched / bifid T wave |
| LQT3 (SCN5A) | Congenital | Long isoelectric ST, late peaked T |
| Acquired | Drugs, electrolytes | Variable |
Common causes of acquired long QT:
- Drugs: antiarrhythmics (quinidine, sotalol, amiodarone), antibiotics (azithromycin, fluoroquinolones), antipsychotics (haloperidol, quetiapine), antihistamines
- Electrolytes: hypokalaemia, hypomagnesaemia, hypocalcaemia
- Bradycardia, hypothyroidism, myocarditis
Life-threatening complication: Torsades de Pointes (TdP) - polymorphic VT with twisting QRS axis around the baseline
Quick Reference Summary Table
| Disease | Rate | Rhythm | P Wave | PR | QRS | ST/T |
|---|---|---|---|---|---|---|
| STEMI | Normal | Regular | Normal | Normal | Normal (or with BBB) | ST elevation (convex) ± Q waves |
| LBBB | Any | Regular | Normal | Normal/prolonged | Wide >120ms, M in V5-V6 | Discordant ST-T |
| Atrial Fibrillation | Variable | Irregularly irregular | Absent (fibrillatory) | None | Narrow (usually) | Variable |
| WPW | Any | Regular (sinus) | Normal | Short <120ms | Wide (delta wave) | Secondary changes |
| Hyperkalaemia | Slow-normal | Variable | Absent (severe) | Prolonged | Wide (severe) | Peaked T waves |
| LVH | Normal | Regular | Normal | Normal | Wide/voltage | Lateral strain pattern |
| PE | Tachycardia | Regular | Normal/P pulmonale | Normal | RBBB possible | S1Q3T3, T inv V1-V4 |
| Complete Heart Block | Slow (escape) | Regular (escape) | Present (faster rate) | Completely variable | Wide or narrow | Variable |
| Pericarditis | Normal | Regular | Normal | PR depression | Normal | Diffuse concave STE |
| Long QT | Variable | Regular | Normal | Normal | Normal | Prolonged QT |
Sources: Rosen's Emergency Medicine | Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine | Braunwald's Heart Disease | Tintinalli's Emergency Medicine | Morgan & Mikhail's Clinical Anesthesiology
Image
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.