Physiology of Urinary System
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from the textbooks. Let me compile the full answer:
Physiology of the Urinary System
The urinary system - primarily the kidneys - performs three fundamental functions: glomerular filtration, tubular reabsorption, and tubular secretion. The net result is:
Urinary Excretion = Glomerular Filtration - Tubular Reabsorption + Tubular Secretion
- Guyton and Hall Textbook of Medical Physiology, p. 347
1. Renal Blood Flow and Clearance
The kidneys receive ~20-25% of cardiac output (~1100 mL/min). Renal plasma flow (RPF) is measured using PAH (para-aminohippuric acid) clearance, because the kidneys extract nearly all PAH from arterial blood via filtration + secretion:
Effective RPF = C_PAH = (U_PAH × V) / P_PAH ≈ 625 mL/min
Renal blood flow (RBF) is calculated from RPF:
RBF = RPF / (1 - Hematocrit)
- Costanzo Physiology, p. 266
2. Glomerular Filtration
Glomerular filtration is the first step in urine formation. Blood entering the glomerular capillaries is filtered into Bowman's space, producing an ultrafiltrate that contains water and small solutes but not proteins or blood cells.
The Glomerular Filtration Barrier (3 Layers)
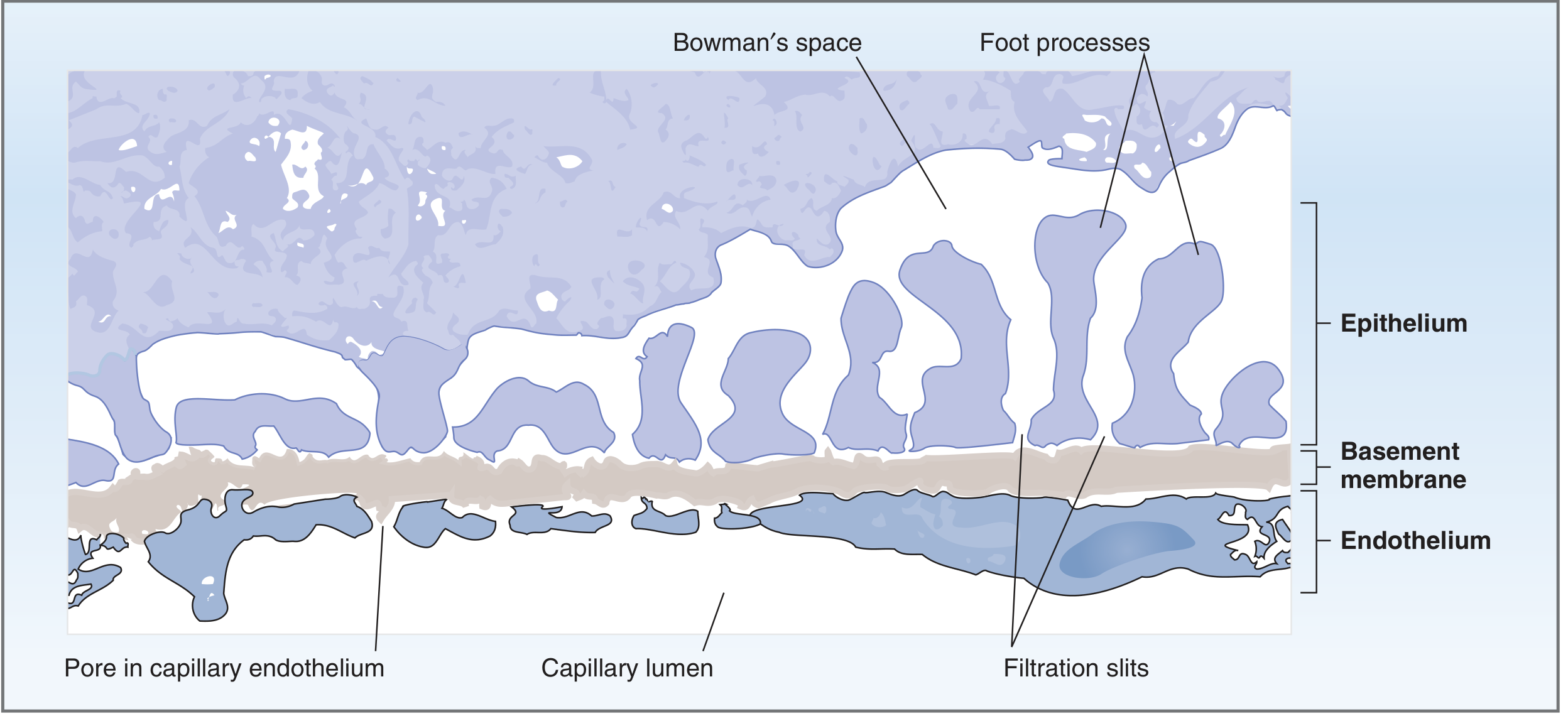
Fig: Structure of the glomerular capillary wall (Costanzo Physiology, p. 267)
| Layer | Feature | Function |
|---|---|---|
| Endothelium | Pores 70-100 nm diameter | Blocks blood cells; allows proteins |
| Basement membrane | Lamina rara interna, lamina densa, lamina rara externa | Main protein barrier; blocks plasma proteins |
| Epithelium (podocytes) | Foot processes with filtration slits (25-60 nm) | Secondary protein barrier |
Charge barrier: Fixed negative charges (glycoproteins) line all three layers, repelling negatively charged plasma proteins and restricting their filtration. In glomerular disease, loss of these negative charges causes proteinuria.
Starling Forces Governing GFR
GFR = K_f × [(P_GC - P_BS) - π_GC]
-
P_GC = Glomerular capillary hydrostatic pressure (~60 mmHg) - favors filtration
-
P_BS = Bowman's space hydrostatic pressure (~18 mmHg) - opposes filtration
-
π_GC = Glomerular capillary oncotic pressure (~32 mmHg) - opposes filtration
-
K_f = Filtration coefficient (hydraulic conductivity × surface area)
-
Net filtration pressure ≈ 10 mmHg (favors filtration)
-
Normal GFR ≈ 125 mL/min (180 L/day)
-
Costanzo Physiology, p. 268
Measuring GFR - Inulin Clearance
GFR is measured by the clearance of inulin (freely filtered, not reabsorbed or secreted) or estimated clinically using creatinine clearance:
C_inulin = (U_inulin × V) / P_inulin = GFR
3. Tubular Reabsorption and Secretion
As filtrate flows through the nephron segments, the kidney reclaims nearly all useful substances and eliminates wastes.
Key Numbers (per day at GFR 180 L/day)
| Substance | Filtered | Reabsorbed | Excreted |
|---|---|---|---|
| Water | 180 L | 178.5 L | 1.5 L |
| Glucose | 180 g | 180 g | 0 |
| NaCl | ~630 g | ~628 g | ~2 g |
| Urea | 54 g | ~32 g | ~22 g |
Key point: Tubular reabsorption is quantitatively enormous and highly selective. A mere 10% reduction in tubular reabsorption could increase urine volume from 1.5 to ~19 L/day.
- Guyton and Hall, p. 347-348
Reabsorption by Nephron Segment
| Segment | What is Reabsorbed | Key Mechanism |
|---|---|---|
| Proximal tubule | ~67% Na+, Cl-, H2O, HCO3-; 100% glucose & amino acids | Na+/K+-ATPase basolaterally; cotransporters (SGLT) apically |
| Thin descending loop of Henle | Water (passively) | Permeable to water, impermeable to solutes |
| Thick ascending loop of Henle | Na+, K+, 2Cl- (via NKCC2) | Impermeable to water - critical for concentration |
| Distal convoluted tubule | Na+, Cl- (via NCC) | Regulated by aldosterone |
| Collecting duct | Na+ (ENaC); water (aquaporins) | ADH-dependent water reabsorption |
Tubular Secretion
Key secreted substances include:
- K+ (principal cells in collecting duct - aldosterone-regulated)
- H+ (intercalated cells - acid-base balance)
- Organic anions/cations (creatinine, PAH, drugs)
4. Urine Concentration and Dilution - The Countercurrent System
The kidney can produce urine ranging from 50 mOsm/L (maximum dilution) to 1200-1400 mOsm/L (maximum concentration).
Countercurrent Multiplier (Loop of Henle)
The thick ascending limb actively pumps NaCl into the medullary interstitium but is impermeable to water, creating a hyperosmotic medulla. This is the basis of the countercurrent multiplier:
- The ascending limb pumps Na+/K+/2Cl- out → medullary interstitium becomes hyperosmotic
- The descending limb (water-permeable) loses water to the concentrated interstitium → filtrate becomes concentrated as it descends
- This concentrated filtrate then enters the ascending limb, allowing more solute to be pumped out
- Urea reabsorbed from the inner medullary collecting duct also contributes to medullary osmolarity
The medullary osmolarity gradient increases from ~300 mOsm/L at the corticomedullary junction to ~1200 mOsm/L at the papilla.
- Guyton and Hall, pp. 938-989
Countercurrent Exchange (Vasa Recta)
The vasa recta (hairpin capillaries) run parallel to the loop of Henle. They prevent washout of the medullary osmotic gradient by equilibrating with interstitial fluid on both descending and ascending passes.
ADH (Antidiuretic Hormone / Vasopressin) - Master Regulator
| Condition | ADH Level | Effect |
|---|---|---|
| High plasma osmolarity (> ~280 mOsm/L) | High | Inserts aquaporin-2 in collecting duct → water reabsorption → concentrated urine |
| Low plasma osmolarity / excess water | Low | Aquaporin-2 removed → dilute urine excreted |
ADH acts via V2 receptors → cAMP → PKA → aquaporin-2 insertion into collecting duct apical membrane.
- Guyton and Hall, p. 840-847
5. Regulation of Sodium and Volume - RAAS
The renin-angiotensin-aldosterone system (RAAS) is central to Na+ and ECF volume regulation:
- Decreased renal perfusion / low Na+ delivery to macula densa → JGA releases renin
- Renin cleaves angiotensinogen → Angiotensin I
- ACE converts Ang I → Angiotensin II
- Ang II: vasoconstriction, stimulates aldosterone release, increases Na+ reabsorption in proximal tubule
- Aldosterone → upregulates ENaC and Na+/K+-ATPase in collecting duct → Na+ retention, K+ excretion
6. Acid-Base Balance
The kidneys regulate blood pH by:
- Reabsorbing filtered HCO3- (mainly proximal tubule, via H+ secretion / carbonic anhydrase)
- Generating new HCO3- by excreting titratable acid (H2PO4-) and ammonium (NH4+) in the distal nephron
- In acidosis: H+ secretion increases, more new HCO3- generated, urine becomes acidic
- In alkalosis: HCO3- secretion increases, less H+ secreted, urine becomes alkaline
7. Micturition (Voiding)
Urine passes from the collecting ducts → renal pelvis → ureters → bladder → urethra.
- Filling phase: Detrusor muscle relaxes (sympathetic β3 stimulation); internal urethral sphincter closes (sympathetic α1); external urethral sphincter remains contracted (somatic/pudendal nerve)
- Voiding phase: Parasympathetic (pelvic nerve) stimulates detrusor contraction; somatic inhibition allows external sphincter to relax; micturition reflex coordinated by pontine micturition center
Normal bladder capacity ~400-600 mL. First urge to void at ~150-200 mL.
Summary: Key Physiological Values
| Parameter | Normal Value |
|---|---|
| GFR | ~125 mL/min (180 L/day) |
| Renal plasma flow (RPF) | ~625 mL/min |
| Renal blood flow (RBF) | ~1100 mL/min |
| Filtration fraction (GFR/RPF) | ~0.20 (20%) |
| Urine output | 1-2 L/day |
| Maximum urine osmolarity | 1200-1400 mOsm/L |
| Minimum urine osmolarity | ~50 mOsm/L |
| Plasma osmolarity | ~285-295 mOsm/L |
Sources: Costanzo Physiology 7th Ed, pp. 266-268 | Guyton and Hall Textbook of Medical Physiology, pp. 347-989
This is a shared conversation. Sign in to Orris to start your own chat.