Osteotomy around hip joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
osteotomy hip joint preservation
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Osteotomies Around the Hip Joint
The goal of an osteotomy around the hip is to redistribute forces evenly across the joint, eliminating excessive point loading. This is achieved either on the femoral side or the acetabular side, depending on the deformity being corrected. The procedure is ideally suited for a young patient with a good range of motion and little or no degenerative change on imaging.
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 576-577
- Campbell's Operative Orthopaedics 15th Ed. 2026
Classification
Osteotomies around the hip are broadly divided into:
- Femoral osteotomies - correcting abnormalities of the proximal femur
- Pelvic/Acetabular osteotomies - correcting acetabular orientation or coverage
Indications
| Femoral Osteotomy | Periacetabular/Pelvic Osteotomy |
|---|---|
| Perthes' disease | Developmental dysplasia of the hip (DDH) |
| Osteoarthritis (young patient) | Acetabular retroversion (reverse PAO) |
| Slipped capital femoral epiphysis (SCFE) | - |
| Avascular necrosis | - |
I. Femoral Osteotomies
A. Intertrochanteric / Subtrochanteric Osteotomy
Performed at the intertrochanteric region, these can correct:
- Varus (adduction osteotomy) - reduces the neck-shaft angle (e.g., coxa valga)
- Valgus (abduction osteotomy) - increases the neck-shaft angle (e.g., coxa vara)
- Derotation - corrects excessive anteversion or retroversion
- Flexion/Extension - corrects sagittal plane deformities
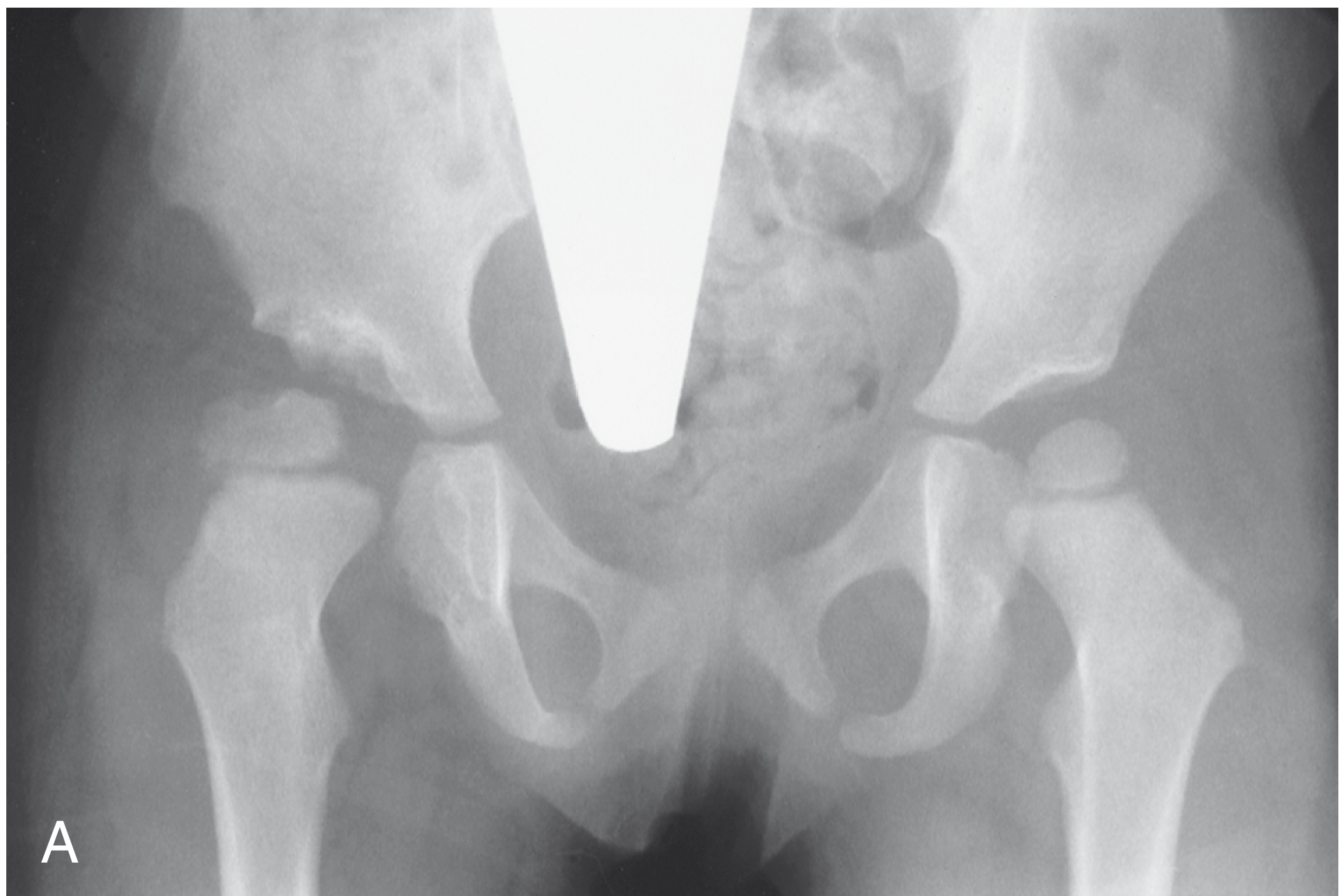
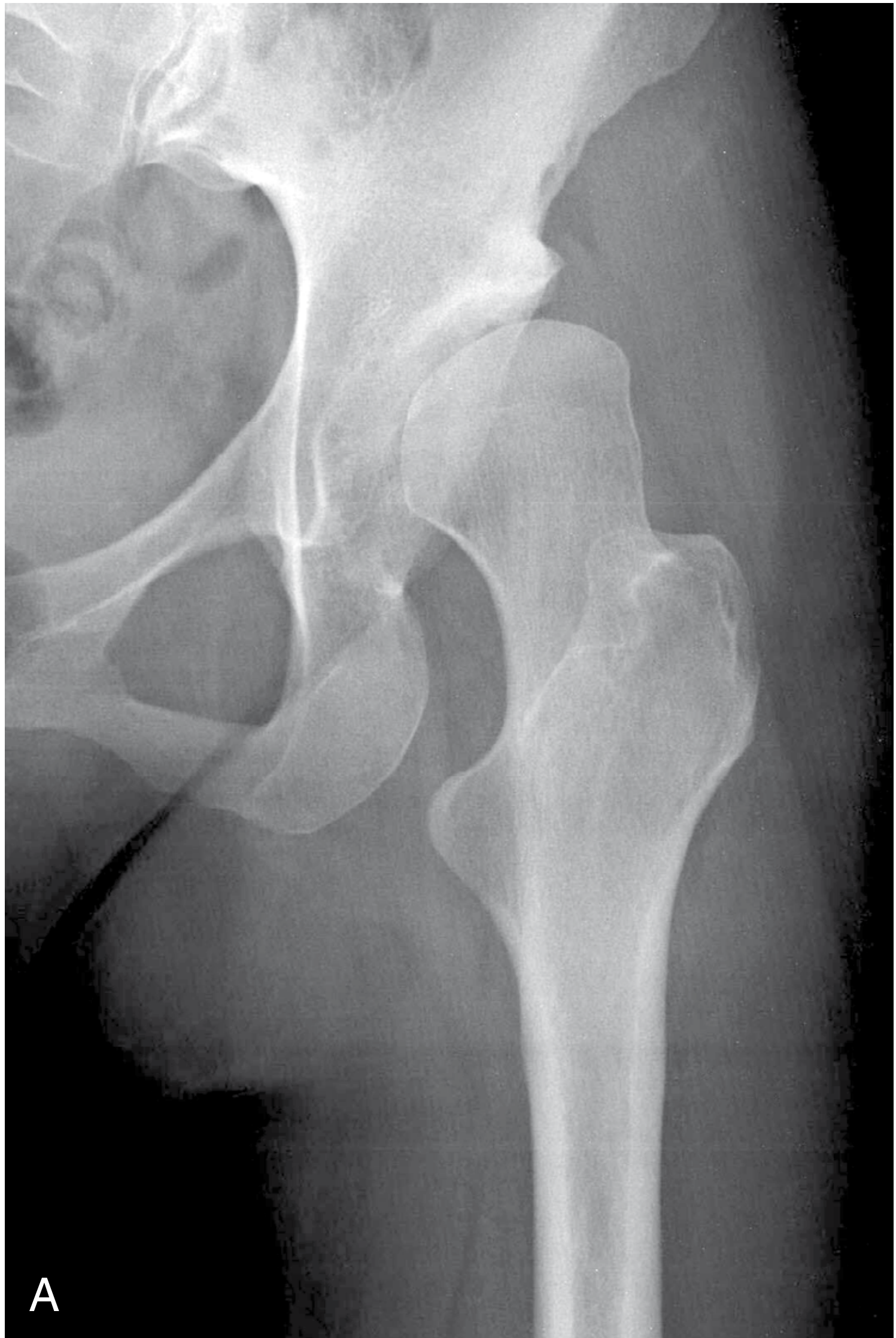
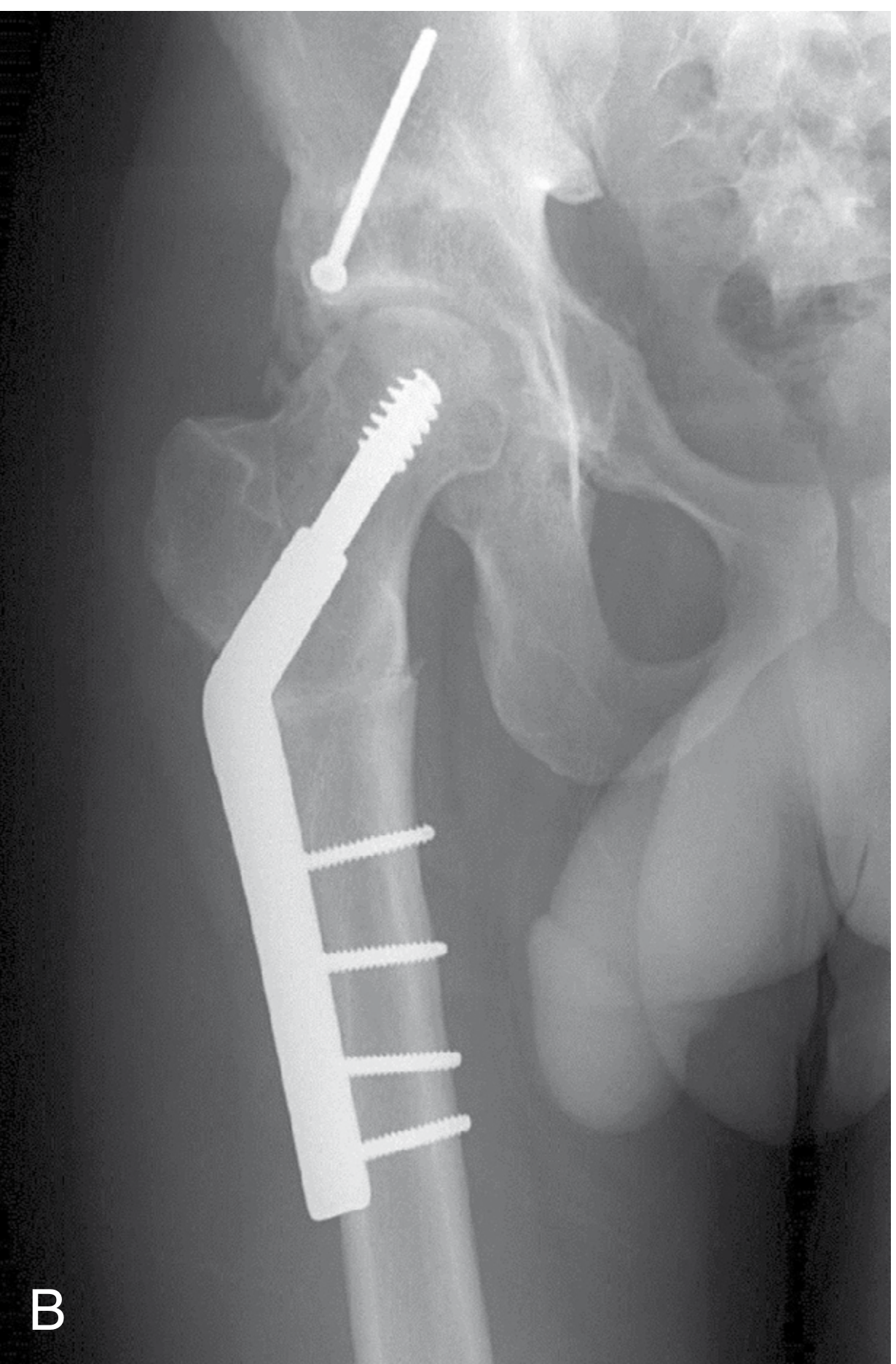
In cerebral palsy hip subluxation, a varus derotation osteotomy (VDRO) combined with femoral shortening is used to reduce the neck-shaft angle to ~120° in ambulatory patients. It is often done with a concurrent acetabular osteotomy.
B. Proximal Femoral Osteotomy for Osteonecrosis
Various proximal femoral osteotomies (flexion, varus, valgus, rotational) have been developed for osteonecrosis with the intent to move the necrotic segment of the femoral head away from the principal weight-bearing area. Best results are achieved in:
- Small/medium lesions (<30% femoral head involvement)
- Patients younger than 55 years
- Idiopathic or posttraumatic cases (better than alcohol/steroid-induced AVN)
Once collapse begins, the hip progresses to end-stage arthritis and arthroplasty is usually required.
C. Brackett Osteotomy
A specific intertrochanteric osteotomy for correcting biplanar deformities (flexion + adduction). The osteotomy is made convex superiorly and medially, starting at the lateral greater trochanter and ending at the lesser trochanter-neck junction. Abduction of the distal fragment corrects the deformity. Advantage: achieves stability without shortening the extremity, though extensive dissection is required.
II. Pelvic (Acetabular) Osteotomies
These are further classified based on whether the acetabulum is redirected (its orientation is changed) or augmented/salvaged (coverage is added without reorientation).
Summary Table (by age/indication)
| Osteotomy | Age | Key Indication |
|---|---|---|
| Salter innominate | 18 months - 6 years | Congruous hip; <10-15° correction of acetabular index needed |
| Pemberton acetabuloplasty | 18 months - 10 years | >10-15° correction needed; small femoral head, large acetabulum |
| Steel triple innominate | Late adolescence (open triradiate cartilage) | Residual acetabular dysplasia, congruous joint |
| Ganz/Bernese PAO | Skeletal maturity (closed triradiate) | Residual dysplasia, congruous joint, symptomatic |
| Shelf / Chiari | Any age; typically older children/adolescents | Incongruous joint; other osteotomies not possible (salvage) |
A. Salter Innominate Osteotomy
Salter observed that in DDH, the entire acetabulum faces more anterolaterally than normal. His osteotomy redirects the entire acetabulum so its roof covers the femoral head anteriorly and superiorly. The cut is made with a Gigli saw from the sciatic notch to just above the anterior inferior iliac spine. The entire acetabulum (with pubis and ischium) rotates as a unit using the symphysis pubis as a hinge. A full-thickness bone wedge from the iliac crest is inserted to hold the correction open anterolaterally.
- Contraindicated in non-concentric hips or severe dysplasia
- Provides mainly anterior and superior coverage
- Postoperative spica cast for 6-8 weeks
B. Pemberton Acetabuloplasty (Pericapsular Osteotomy)
Indicated when more correction (>10-15° of acetabular index) is needed than Salter can provide, or when a small femoral head sits in a large acetabulum. The osteotomy is made through the full thickness of ilium from just above the anterior inferior iliac spine posteriorly to the triradiate cartilage, which acts as a hinge. The acetabular roof is rotated anteriorly and laterally. This procedure decreases the volume of the acetabulum and produces joint incongruity that requires remodeling (unlike Salter). It can only be performed while the triradiate cartilage remains open.
C. Steel Triple Innominate Osteotomy
Cuts through the ischium, superior pubic ramus, and ilium superior to the acetabulum, freeing the acetabulum as a mobile segment with attached articular cartilage. Indicated for older children and adolescents with residual dysplasia when the triradiate cartilage is still open. Can provide more correction than Salter. The Steel procedure is preferred for open triradiate cartilage; the Ganz osteotomy for closed triradiate cartilage.
D. Bernese Periacetabular Osteotomy (PAO) - Ganz
The gold-standard hip-preserving procedure for symptomatic hip dysplasia in skeletally mature adults. It frees the acetabulum via multiple cuts around the acetabulum while preserving the posterior column of the pelvis (maintaining pelvic ring stability). The acetabular fragment is then reoriented to optimize femoral head coverage.
Surgical approach: The original technique used a Smith-Petersen approach. A modified abductor-sparing variant (Murphy-Millis) or a rectus-sparing approach (for patients without cam deformity or labral pathology) may also be used. A bikini-type skin incision can be used in thin females for cosmesis.
Outcomes: At 11-year follow-up, good-to-excellent results with no evidence of OA were reported (Siebenrock et al.). Longer-term studies show hip preservation rates of 73-76% at >9 years, 60% at 20 years, and 29% at 30 years. After PAO, if varus deformity of the proximal femur develops causing impingement, a secondary proximal femoral valgus osteotomy may be needed.
PAO is also used (reverse PAO) for acetabular retroversion, where the acetabulum is rotated in the opposite direction (anteverting the acetabulum to treat pincer-type femoroacetabular impingement).
E. Shelf Procedure (Staheli)
An augmentation (non-redirectional) procedure. An extra-articular shelf of bone is added to the lateral edge of the acetabulum, providing additional coverage. Indicated at any age when the joint is incongruous or when redirectional osteotomies are not feasible. The shelf acts as a load-bearing extension of the acetabular roof.
F. Chiari Medial Displacement Osteotomy
A salvage procedure. The osteotomy is made through the ilium just above the joint capsule, and the distal fragment (containing the hip joint) is displaced medially. The cut surface of the proximal fragment then acts as a roof, but because there is no articular cartilage, the intervening joint capsule undergoes fibrocartilaginous metaplasia to serve as the new articulating surface. Indicated in incongruous joints where better options are not available.
III. Combined Pelvic + Femoral Osteotomy
In older children with both femoral and acetabular abnormalities, a combined pelvic and varus femoral osteotomy may be required to address both deformities simultaneously, such as in DDH with associated high neck-shaft angle, or in cerebral palsy with combined coxa valga + acetabular dysplasia.
Preoperative Planning
Thorough preoperative planning is essential. Increasingly:
- 3D CT scans are used for planning
- 3D printing is used to understand the deformity
- Computer navigation and robotics are emerging adjuncts for accurate correction
The desired correction must be simulated preoperatively to confirm it is achievable.
Key Principles Summary
| Principle | Detail |
|---|---|
| Best candidate | Young patient, good ROM, minimal/no OA |
| Goal | Redistribute joint forces, delay arthroplasty |
| Femoral osteotomy | Corrects neck-shaft angle, anteversion |
| Redirectional acetabular osteotomy | Reorients acetabulum (Salter, Pemberton, Steel, Ganz PAO) |
| Salvage osteotomy | Adds coverage without true reorientation (Shelf, Chiari) |
| Fixation | Internal fixation (blades, plates, screws) + cast in children |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., p. 576-577; Campbell's Operative Orthopaedics 15th Ed. 2026, Chapters 7, 12, 13, 15; Miller's Review of Orthopaedics 9th Ed.
Carpal joint dislocation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, well-structured answer.
Carpal Joint Dislocation
Overview
Carpal dislocations are significant wrist injuries that represent a spectrum of ligamentous and bony disruption. They are most commonly caused by a fall on an outstretched hand (FOOSH) with forced dorsiflexion, ulnar deviation, and intercarpal supination. The most commonly involved carpal bone is the lunate. These injuries are frequently missed at initial presentation (approximately 16-25% missed), and delayed diagnosis worsens prognosis significantly.
Classification
A. Carpal Instability Classification (Campbell's / Taleisnik)
| Type | Name | Description |
|---|---|---|
| CID | Carpal Instability Dissociative | Instability within a carpal row (e.g., scapholunate or lunotriquetral dissociation) |
| CIND | Carpal Instability Non-Dissociative | Instability between carpal rows or between radius and proximal row (radiocarpal or midcarpal) |
| CIC | Carpal Instability Combined | Combination of CID and CIND (e.g., perilunate dislocations) |
| Adaptive | Adaptive Carpus | Carpal malalignment secondary to malunion (e.g., distal radius malunion, scaphoid non-union) |
Radiographic patterns: DISI = dorsal intercalated segment instability; VISI = volar intercalated segment instability; UT = ulnar translation; PT = proximal translation
B. Perilunate Injuries: Lesser Arc vs. Greater Arc
| Arc | Type | Pattern |
|---|---|---|
| Lesser arc | Pure ligamentous | Force transmitted circumferentially around lunate through ligaments only |
| Greater arc | Fracture-dislocation | Ligament rupture combined with fractures of the carpus (radial styloid, scaphoid, capitate, triquetrum) |
Greater-arc injuries are twice as common as lesser-arc injuries.
Mayfield Stages of Progressive Perilunate Instability
This describes sequential ligamentous disruption propagating in a circular arc around the lunate (from radial to ulnar), caused by hyperextension-supination-ulnar deviation force.
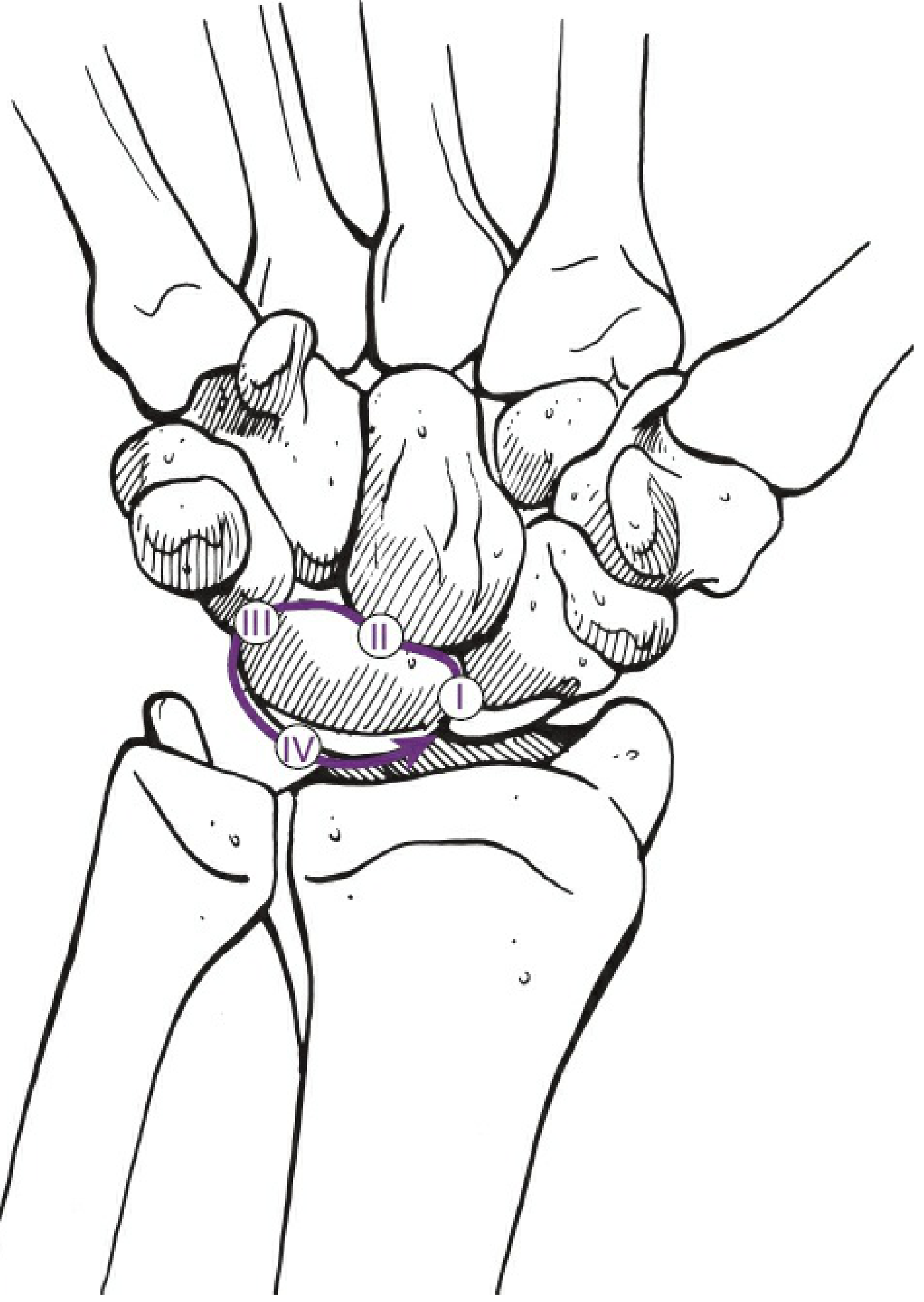
| Stage | Injury | Radiographic Pattern |
|---|---|---|
| I | Scapholunate ligament disruption (SLD) or scaphoid fracture | Increased scapholunate gap (>3mm); DISI; signet ring sign |
| II | Lunocapitate dislocation (capitate dislocates dorsally through Space of Poirier) | Capitate dorsal to lunate on lateral view; perilunate dislocation |
| III | Lunotriquetral ligament disruption | Midcarpal dislocation; entire proximal row except lunate displaced |
| IV | Lunate dislocation (lunate displaces volarly off the radius) | Triangular lunate on PA ("piece of pie"); "spilled teacup" on lateral |
The Space of Poirier - a weak region between the extrinsic volar ligament arcades - opens with wrist dorsiflexion and is the site through which the capitate dislocates.
Specific Injury Types
1. Scapholunate Dissociation (Mayfield Stage I / CID)
The most common carpal dissociation injury and most frequently missed.
Mechanism: Forced wrist extension ruptures the scapholunate interosseous ligament, causing the scaphoid to flex (rotating out of the radial fossa) while the lunate remains in place.
Clinical features:
- Pain and swelling over dorsal wrist
- Positive Watson scaphoid shift test: upward pressure on scaphoid tuberosity while moving hand from ulnar to radial deviation produces a painful clunk as the scaphoid subluxes over the dorsal rim of the radius
Radiographic findings:
- Terry Thomas sign (= David Letterman sign): gap between scaphoid and lunate on PA view >3mm (normal <2mm); 4mm+ confirms dissociation
- Signet ring sign: scaphoid appears shortened/end-on due to rotatory subluxation - the distal pole cortex creates a ring shadow
- Best accentuated on clenched fist AP view in ulnar deviation
- DISI pattern on lateral: dorsiflexed lunate (capitolunate angle >30°, scapholunate angle >60°)

Management:
- ED: Splinting in neutral to 10-15° dorsiflexion; urgent hand surgery referral
- Definitive: K-wire fixation + ligament repair; late cases may need ligament reconstruction
2. Perilunate Dislocation (Mayfield Stage II-III)
Definition: Posterior (dorsal) dislocation of the carpus around the lunate, while the lunate maintains its articulation with the distal radius.
Mechanism: High-energy trauma (fall from height, MVA, sports) - 61-65% associated with scaphoid fracture, 26% associated with polytrauma.
Clinical features:
- Young males predominantly
- Pain, swelling, tenderness over dorsum of wrist
- Gross deformity often absent despite severe injury
- Median nerve symptoms in ~16% of cases (acute carpal tunnel syndrome from volar lunate displacement)
- Ulnar neuropathy, arterial injury, or tendon disruption may also be present
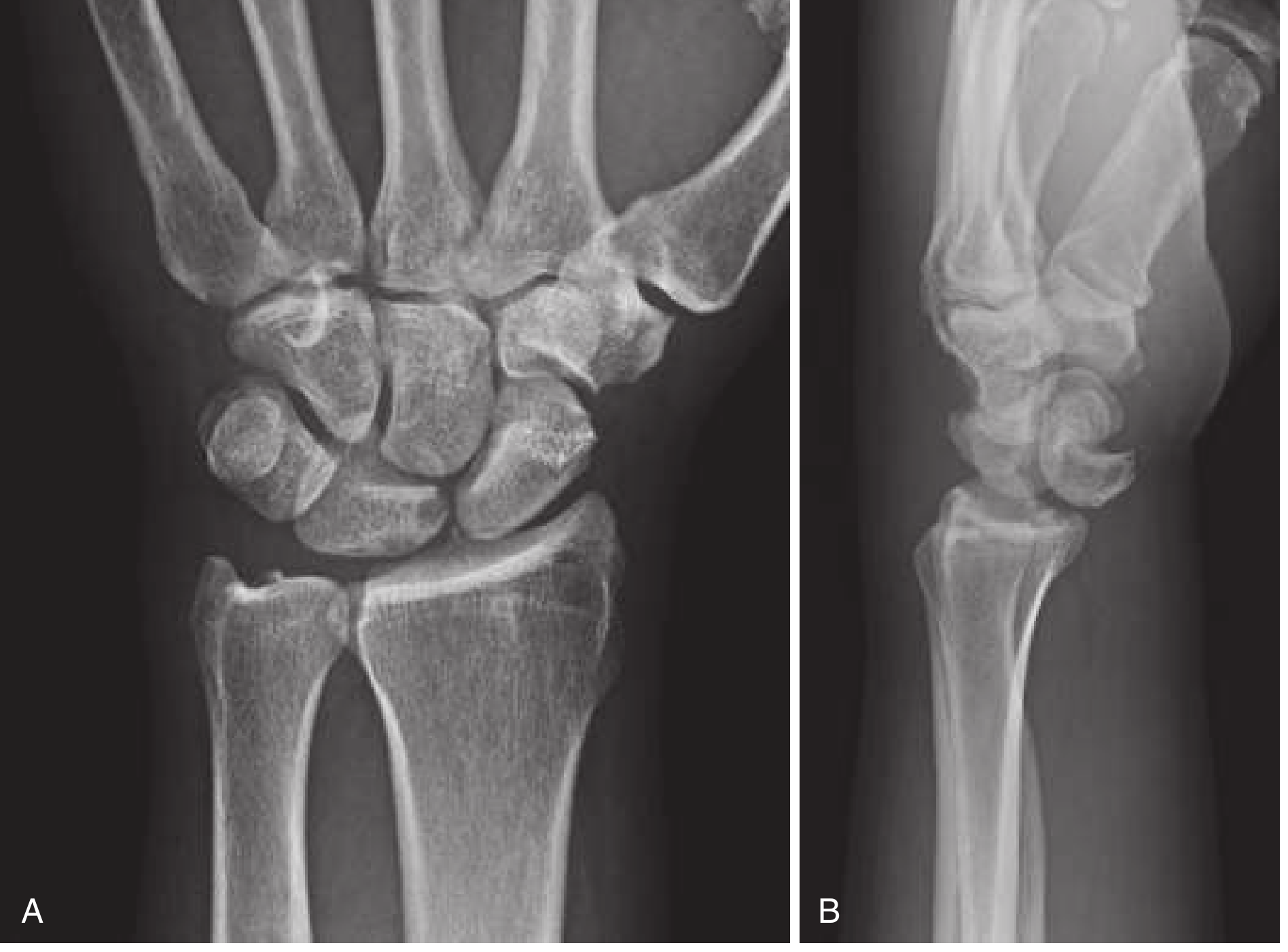
Radiographic findings:
On PA view:
- Disruption of Gilula's three carpal arcs - overlapping carpal bones
- Obliterated capitolunate joint space
- Scapholunate and triquetrolunate spaces may be widened or obliterated
- Shortened scaphoid (rotary subluxation/fracture)
- Increased ulnocarpal translation (>50% uncovering of lunate)
On lateral view:
- "Three C's" sign disrupted - capitate (third C) displaced dorsal to lunate
- Lunate retains contact with radius
- Increased scapholunate angle (>60°) and capitolunate angle (>30°)

PA view shows disrupted carpal arcs with overlapping bones; Lateral view shows capitate dorsal to lunate - Rosen's Emergency Medicine, Fig. 43.22
3. Lunate Dislocation (Mayfield Stage IV)
Definition: The lunate itself dislocates volarly (palmarly) off the distal radius, while the rest of the carpus may rebound and re-articulate with the radius.
Pathomechanism: The dorsally displaced capitate rebounds and pushes the lunate anteriorly off the radius, rupturing the dorsal radiocarpal ligament.
Radiographic findings:
On PA view:
- Lunate assumes a triangular shape ("piece of pie" sign) due to palmar rotation
On lateral view:
- "Spilled teacup" sign: the cup-shaped lunate is rotated with its concavity facing anteriorly (palmarly), resembling a cup spilling its contents into the palm
- Capitate may rebound and rest on radius
- Disrupted three C's sign - lunate (middle C) is pushed off the radius
Key distinction from perilunate dislocation:
| Feature | Perilunate Dislocation | Lunate Dislocation |
|---|---|---|
| Lunate position | Stays in radial fossa | Dislocates volarly off radius |
| Capitate | Dorsally displaced | May rebound onto radius |
| Lateral view | Capitate dorsal to lunate | "Spilled teacup" - lunate tipped palmarly |
| PA view | Disrupted arcs | Triangular lunate ("piece of pie") |
4. Transscaphoid Perilunate Dislocation (Greater Arc Injury)
The most common greater-arc (fracture-dislocation) pattern. A scaphoid waist fracture occurs, and the distal scaphoid dislocates with the distal carpal row, while the proximal scaphoid and lunate remain in near-normal position. Often the scapholunate ligament is spared (force goes through bone instead). The prefix "trans-" is added to the fractured bone name (e.g., transscaphoid perilunate dislocation, transcapitate, transradial styloid, etc.).
The scaphocapitate syndrome occurs when both scaphoid and capitate fracture, with the capitate fragment rotated 180°. Both fragments are devascularized.
5. Mid-Carpal Dislocation
An intermediate injury where the lunate is subluxed (not fully dislocated) volarly, and the carpus is displaced posteriorly. This is thought to represent partial spontaneous realignment following a perilunate dislocation.
6. Radiocarpal Dislocation
Extremely rare, high-energy injury. The entire carpus dislocates from the distal radius. Ulnar translation is far more common than radial translation. Extensive soft tissue damage and neurovascular compromise are common. Always requires ORIF.
Radiological Assessment Summary
Normal Lateral Alignment (Three C's sign):
A straight line through the center of the radius should pass through the center of the lunate and the capitate. This alignment is lost in all forms of carpal dislocation.

Normal Gilula's Arcs (PA view): Three smooth arcs along the proximal and distal articular surfaces of the proximal carpal row, and the proximal surfaces of the distal row. Disruption of any arc indicates intercarpal injury.
Management
Emergency Department
- Immediately recognize - high index of suspicion; ~1 in 4 are missed on initial evaluation
- Immediate closed reduction - a patient should not leave the ED with an unreduced perilunate dislocation
- CT scan after reduction to assess associated fractures (may be obtained pre-operatively if reduction not possible)
- Emergent hand surgery consultation
- Splinting in long-arm cast/splint after reduction
Closed Reduction (Tavernier Maneuver)
- Requires complete relaxation under general or regional anesthesia (local anesthesia is inadequate)
- Traction applied to the hand and wrist
- Capitate is locked into the distal concavity of the lunate
- Wrist extended to reduce the capitate beneath the lunate, then wrist flexed to maintain reduction
Definitive Treatment
| Scenario | Treatment |
|---|---|
| Reducible, stable (rare) | Closed reduction + long-arm splint/cast; urgent operative follow-up |
| Reducible but unstable (most cases) | Closed reduction + percutaneous K-wire fixation; formal ORIF |
| Irreducible or acute carpal tunnel syndrome | Emergent surgery - open reduction via dorsal and/or volar approach + ligament repair + K-wire or screw fixation |
| Greater-arc (fracture-dislocation) | ORIF with cannulated screw fixation of scaphoid + ligament repair |
| Chronic (>6 weeks) | Open reduction if feasible; salvage procedures (proximal row carpectomy - PRC, or total wrist arthrodesis) for late cases |
Median Nerve Management
- Most cases resolve after closed reduction
- Immediate carpal tunnel decompression generally not required unless symptoms fail to resolve
- Severe/increasing median or ulnar neuropathy = absolute indication for surgical exploration
K-wire vs. Screw Fixation
- K-wires: traditional, but risk of infection and stiffness; kept 8 weeks, cast for 3 months
- Temporary screw fixation: advocated by some to reduce these risks
Complications
- Acute carpal tunnel syndrome (median nerve compression by volarly displaced lunate)
- Avascular necrosis of the lunate or proximal scaphoid
- Chronic carpal instability and carpal collapse
- Posttraumatic osteoarthritis (7-92% range; mean ~38% in fracture-dislocations)
- Stiffness and permanent reduction in grip strength
- Tendon rupture (late, in neglected cases)
- Missed diagnosis leading to delayed, more difficult treatment
Prognosis
The prognosis is guarded even with optimal treatment. Studies show:
- Good patient satisfaction rates, but high rates of loss of reduction
- Up to 50% develop posttraumatic arthritis in longer follow-up
- Return to employment is common but complete restoration of function is rare
- Poor prognostic indicators: manual workers, poor initial reduction, combined volar-dorsal surgical approach
- Delay between injury and treatment uniformly worsens outcomes
Sources: Rockwood & Green's Fractures in Adults 10th Ed. 2025; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Bailey & Love's Short Practice of Surgery 28th Ed.; Grainger & Allison's Diagnostic Radiology; Campbell's Operative Orthopaedics 15th Ed. 2026; Miller's Review of Orthopaedics 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.