Image of lavacuator tube
Reading File
Finding Sources
Searching the Web
lavacuator tube image gastric lavage
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I have good images and textbook content. Here is the full answer:
Lavacuator Tube
The Lavacuator (also spelled "lavacuator") is a large-bore, clear plastic orogastric hose specifically designed for gastric lavage. It is the preferred tube for stomach washout in cases of poisoning and overdose.
Images
Image A & B - Classic Lavacuator tube (double-lumen design):
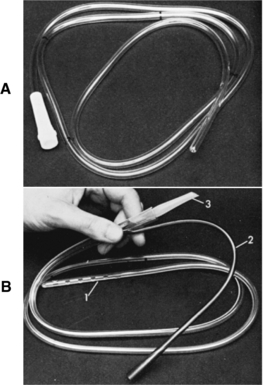
(A) The assembled tube. (B) Components labeled: 1 = gastric hose with multiple distal holes, 2 = drainage tubing, 3 = Y-connector adapter for closed-system lavage.
Modern lavacuator / large-bore gastric lavage tube (green-striped variant):

Key Features
| Feature | Detail |
|---|---|
| Bore size (adults) | 36-40 Fr (external diameter ~12-13.3 mm) |
| Bore size (children) | 24-28 Fr (diameter ~7.8-9.3 mm) |
| Route | Orogastric (NOT nasogastric - too large for the nose) |
| Distal end | Multiple holes cut near the tip to enhance aspiration of particulate matter |
| Y-connector | Closed system with two arms - one for fluid infusion, one for drainage |
| Material | Clear, flexible plastic (allows visual inspection of aspirate) |
How It Works
The Y-connector closed system allows sequential lavage cycles:
- Clamp the drainage arm, infuse aliquots of fluid (tap water in adults; warmed normal saline in children) into the stomach
- Clamp the infusion arm, open the drainage arm - gravity drainage of stomach contents
- Intermittent suction can be applied to enhance emptying
Clinical Notes
- Larger diameter tubes are more likely to retrieve particulate matter, but whole pills still rarely pass through
- The tube is large enough that it must be passed orally only
- Position patient in left lateral decubitus, Trendelenburg (~20-degree tilt) to reduce aspiration risk and slow passage of gastric contents into the duodenum
- Confirm placement radiographically before starting lavage
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Ch. 42; P.C. Dikshit Textbook of Forensic Medicine and Toxicology
Absolute vs relative
Reading File
Finding Sources
Finding Sources
The Roberts & Hedges textbook doesn't split into "absolute vs relative" by name, but the content clearly separates them. Here is the organized breakdown:
Absolute vs Relative Contraindications to Gastric Lavage
The textbooks group contraindications into hard stops (absolute) and situations requiring caution (relative):
Absolute Contraindications
| # | Contraindication | Reason |
|---|---|---|
| 1 | Unprotected airway (no gag reflex, obtunded patient without ETT) | High risk of aspiration of lavage fluid and gastric contents |
| 2 | Corrosive ingestion (strong acids or alkalis) | Passing the tube risks further esophageal/gastric perforation |
| 3 | Hydrocarbon ingestion (unless containing highly toxic pesticides or heavy metals) | Risk of aspiration pneumonitis; the toxin absorption risk is less than the lavage risk |
| 4 | Known esophageal stricture | Tube passage risks rupture |
| 5 | History of gastric bypass surgery | Altered anatomy - tube placement is dangerous and unreliable |
Relative Contraindications (Use With Caution)
| # | Contraindication | Reason |
|---|---|---|
| 1 | Combative / uncooperative patient | Risk of injury to patient and staff; tube displacement |
| 2 | Bleeding diathesis (coagulopathy, thrombocytopenia) | Mucosal trauma during tube passage can cause significant bleeding |
| 3 | Ingestion >1-2 hours prior | Most benefit is within 1 hour; risk-benefit tilts against lavage with increasing time |
Important Note on "Protected Airway"
A patient who is intubated moves the airway contraindication from absolute to relative - many clinicians will proceed with lavage in a seriously ill intubated patient because the airway is already protected. However, intubation + paralysis solely to perform gastric lavage is generally not recommended.
Key principle: The distinction between absolute and relative is essentially - absolute contraindications mean lavage should never be done regardless of circumstance; relative means the risk must be weighed against the potential benefit of toxin removal, with additional precautions taken.
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Ch. 42 - Gastric Lavage
Why hypothermia contraindicated in hypothermia
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have a clear and complete picture. Here is the answer:
Why is Cold Gastric Lavage Contraindicated in Hypothermia?
The question is: cold gastric lavage (used as a cooling technique) is contraindicated in patients who are already hypothermic (low body temperature). This seems paradoxical because cold lavage is used to cool patients -- so why not in hypothermia?
The Logic
Cold gastric lavage is a core cooling technique designed for hyperthermia (heatstroke) -- it works by instilling iced water into the stomach, which sits adjacent to the liver, great vessels, kidneys, and heart, rapidly drawing heat away from core organs.
If a patient is already hypothermic (core temp already low), instilling iced water would:
- Worsen the hypothermia - further drop core temperature, potentially into life-threatening ranges (severe hypothermia <28°C causes ventricular fibrillation)
- Remove what little heat remains - the body in hypothermia is already struggling to maintain core temperature; cold lavage actively strips more heat from central organs
- Trigger cardiac arrhythmias - the heart in hypothermia is highly irritable; cold fluid near the pericardium/great vessels can precipitate VF
What It Is Used For (and When It Is Appropriate)
| Indication | Contraindication |
|---|---|
| Severe hyperthermia / heatstroke | Pre-existing hypothermia |
| Cooling rate: ~0.15°C/min | Would deepen dangerous core cooling |
| Best when external cooling is insufficient | Any condition with low core temp |
Key Teaching Point
Cold gastric lavage takes heat away from the core. In hyperthermia you want this. In hypothermia you absolutely do not -- it would be adding insult to injury by cooling an already dangerously cold patient further.
The same principle applies to other cold lavage methods (bladder, peritoneal, rectal) -- all are contraindicated in hypothermia for identical reasons.
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Ch. 65 - Cold Gastric Lavage / Contraindications to Rapid Cooling
Create a quick reference guide on heatstroke vs hypothermia management
Activated charcoal use in gastric lavage
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here are both answers:
1. Quick Reference Guide: Heatstroke vs Hypothermia Management
Definition & Classification
| Feature | Heatstroke | Hypothermia |
|---|---|---|
| Core temp | >40°C (>104°F) | <35°C (<95°F) |
| Mild | 37-40°C | 32-35°C |
| Moderate | -- | 28-32°C |
| Severe | >40°C with organ failure | <28°C |
| Key danger | Multi-organ failure, cerebral edema | VF, cardiac arrest |
Heatstroke Management
Goal: Reduce rectal temp to ≤40°C within 30 minutes
Step 1 - ABCs + Monitoring
- IV access, cardiac monitor, pulse oximetry
- Consider intubation if GCS impaired (also needed before gastric lavage)
Step 2 - Cooling Techniques (in order of preference)
| Technique | Method | Cooling Rate | Notes |
|---|---|---|---|
| Evaporative (1st choice) | Tepid water mist (15°C) + large warm fans, expose all body surfaces | ~0.10-0.31°C/min | Simplest, fastest external method; non-invasive |
| Ice water immersion | Full body submersion in ice water | ~0.15-0.20°C/min | Effective but cumbersome; monitoring difficult; shivering |
| Strategic ice packs | Axilla, groin, neck | ~0.03-0.11°C/min | Adjunct; patient tolerates poorly |
| Cold gastric lavage | 10 mL/kg iced water, 30-60s dwell, suction - repeat | ~0.15°C/min | Requires ETT; invasive; limited human data |
| Cold peritoneal lavage | Peritoneal catheter, cold fluid | ~0.11-0.56°C/min | Rapid; invasive; only if not responding |
| Hemodialysis/ECMO | Cold dialysate 30-35°C | Variable | Last resort for refractory cases |
Step 3 - Pharmacologic Adjuncts
| Drug | Indication | Notes |
|---|---|---|
| Dantrolene | Muscle rigidity OR suspected malignant hyperthermia (MH) | NOT routinely used in heatstroke (no benefit in RCT) |
| Bromocriptine / Amantadine | Neuroleptic malignant syndrome (NMS) | Dopamine agonist |
| IV Ketorolac 30mg | Adjunct to cooling | One RCT: temp 2x lower at 90 min vs placebo |
| Benzodiazepines | Shivering / agitation | Reduces metabolic heat production |
Cooling Contraindication
- Rapid cooling is never contraindicated in heatstroke
- Cold gastric lavage: contraindicated without protected airway (ETT)
Hypothermia Management
Goal: Increase core temp at 0.5-2.0°C/hour; avoid aggressive rewarming in mild/stable cases
Rewarming Methods by Severity
| Severity | Temp | Method |
|---|---|---|
| Mild | 32-35°C | Passive External Rewarming (PER): remove wet clothing, insulate, blankets, warm oral fluids (only if fully alert), warm IV fluids |
| Moderate | 28-32°C | Active External Rewarming (AER): heating pads/blankets to trunk only, forced warm air; + less invasive active core |
| Severe | <28°C | Active Core Rewarming (ACR): warmed humidified oxygen, warm IV fluids 40-42°C, bladder/gastric/pleural warm lavage, ECMO/bypass |
Active Core Rewarming Options
| Technique | Route | Notes |
|---|---|---|
| Warmed IV fluids (40-42°C) | IV | Counteracts cold diuresis; first step |
| Warmed humidified O₂ | Airway | 40-45°C |
| Warm bladder lavage | Foley | Minimally invasive |
| Warm gastric lavage | NG/OG tube | Warm fluid (opposite of heatstroke!) |
| Warm pleural lavage | Chest tubes | Bilateral |
| Peritoneal lavage | Peritoneal catheter | Relative CI if prior abdominal surgery |
| ECMO / Cardiac bypass | Vascular | Most effective; for cardiac arrest + hypothermia |
Pitfalls in Hypothermia
| ⚠️ Danger | Reason |
|---|---|
| Aggressive rewarming in mild cases | Can cause rebound hypotension, paradoxical core temp drop, arrhythmias |
| Cold IV fluids | Worsen hypothermia |
| Cold gastric lavage | Absolutely contraindicated - worsens core cooling, precipitates VF |
| Ignoring underlying cause | Hypoglycemia, sepsis, adrenal crisis, hypothyroidism, drug OD must be treated simultaneously |
Side-by-Side Summary
| Heatstroke | Hypothermia | |
|---|---|---|
| Core temp direction | ↑ Must LOWER | ↓ Must RAISE |
| Gastric lavage fluid | Ice cold | Warm (40-45°C) |
| Fan/airflow | Yes - maximize evaporation | No - increases heat loss |
| Dantrolene | Only if rigidity / MH | Not indicated |
| ECMO | Last resort for refractory | Cardiac arrest + severe hypothermia |
| Endpoint | Rectal temp ≤40°C in 30 min | Core temp rising 0.5-2°C/hr |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Ch. 65; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
2. Activated Charcoal in Gastric Lavage
What Is It?
Activated charcoal (AC) is a fine black powder of carbon treated to have an enormous surface area. It adsorbs (binds) most organic toxins in the gut, reducing systemic absorption. It is given after gastric lavage is completed, through the same lavage tube before removal.
Timing in the Procedure
After gastric aspiration and lavage are completed → administer AC slurry through the gastric tube → then clamp the tube before removal (to avoid dribbling into airway)
Dosing
| Age | Single Dose |
|---|---|
| <1 year | 1 g/kg body weight |
| 1-12 years | 25-50 g |
| >12 years / adult | 25-100 g |
Target ratio: 10:1 (charcoal : toxin by weight) if amount ingested is known. Plain aqueous charcoal (without sorbitol) is preferred.
Indications
- Most organic drug/toxin overdoses where a clinically significant fraction remains in the GI tract
- Most effective within 60 minutes of ingestion (extended for bezoar-forming drugs like aspirin)
- AC is generally considered superior to gastric lavage alone for gut decontamination
- MDAC (multiple-dose AC) is used to:
- Prevent ongoing absorption (extended-release/enteric-coated preparations)
- Enhance elimination of already-absorbed drugs by interrupting enterobiliary recirculation (e.g., phenobarbital, theophylline, carbamazepine, digoxin, dapsone, quinine)
Contraindications
| Contraindication | Reason |
|---|---|
| Unprotected airway (no ETT) | Aspiration risk - can cause pneumonitis, ARDS, bronchiolitis obliterans |
| Corrosive ingestion (acids/alkalis) | No benefit; triggers vomiting; can enter mediastinum/peritoneum if perforation |
| Aliphatic hydrocarbons | Not adsorbed by AC; increases aspiration risk |
| Iron ingestion | Iron NOT adsorbed by charcoal |
| Lithium ingestion | Lithium NOT adsorbed by charcoal |
| Ethanol ingestion | Not adsorbed |
| Bowel obstruction/perforation | Inspissated charcoal worsens obstruction |
| Gastric bypass history | Anatomical risk |
Complications
| Complication | Notes |
|---|---|
| Pulmonary aspiration | Most feared; 4-39% in intubated patients; can cause pneumonitis, ARDS |
| Vomiting | In both awake and obtunded patients |
| Constipation | Common |
| Bowel obstruction | From inspissated charcoal (especially MDAC) |
| Bowel perforation | Rare; reported in diverticular disease |
| Electrolyte imbalance | With MDAC + cathartic combinations |
Lavage + AC vs AC Alone
- Within 1 hour of ingestion: lavage + AC provides a small but statistically significant advantage over AC alone
- After 1 hour: no difference in outcome between lavage + AC vs AC alone
- Current trend: AC used in <1% of overdose cases in the US (2014 data); lavage also declining
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, Ch. 42; Goldman-Cecil Medicine, Ch. 96
Urinary alkalization vs urinary acidification
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent textbook content retrieved. Here is the complete answer:
Urinary Alkalinization vs Urinary Acidification
Both are enhanced elimination techniques that exploit the principle of ion trapping - manipulating urinary pH to keep a drug ionized in the tubular lumen so it cannot be reabsorbed and must be excreted.
The Core Principle: Ion Trapping
| Drug type | Behavior in urine | Trick |
|---|---|---|
| Weak ACID (e.g. salicylate, phenobarbital) | Unionized in acidic urine → reabsorbed | Alkalinize urine → drug becomes ionized → trapped → excreted |
| Weak BASE (e.g. amphetamine, PCP) | Unionized in alkaline urine → reabsorbed | Acidify urine → drug becomes ionized → trapped → excreted (but NOT recommended - see below) |
1. Urinary Alkalinization ✅ (Recommended)
Mechanism
Raising urine pH causes weak acid drugs to become ionized (negatively charged) → cannot cross tubular cell membranes → stay in urine → excreted. Also alkalinizes serum, which keeps drugs like salicylate out of the CNS (added benefit).
Drugs Treated
| Drug | Notes |
|---|---|
| Salicylates (aspirin) | Primary indication; serum level >30 mg/dL = start; alkalinization also prevents CNS penetration |
| Phenobarbital | Weak acid; enhanced elimination |
| Chlorpropamide | Weak acid |
| Methotrexate | Weak acid |
| 2,4-Dichlorophenoxyacetic acid (herbicide) | Weak acid |
| Formic acid | Methanol metabolite |
| Chlorpropamide | Oral hypoglycemic |
Mnemonic - CAMPS: Chlorpropamide, Aspirin/salicylates, Methotrexate, Phenobarbital, (2,4-D/herbicides)
Protocol
- IV bolus: Sodium bicarbonate 1-2 mEq/kg body weight
- Infusion: 3 ampules (150 mEq) of 8.4% NaHCO₃ in 1 L D5W + 20-40 mEq KCl → infuse at 2-3x maintenance rate (up to 250 mL/hr)
- Target urine pH: 7.5-8.0 (check hourly)
- Target serum pH: 7.45-7.55 (do NOT exceed 7.55)
Critical: Correct Hypokalemia First
Alkalinization causes intracellular shift of K⁺ → hypokalemia → distal tubule compensates by excreting H⁺ in exchange for K⁺ → acidifies urine → defeats the purpose entirely. Always co-administer potassium.
Contraindications
- Volume overload
- Cerebral or pulmonary edema
- Severe alkalemia (pH >7.55)
2. Urinary Acidification ❌ (NOT Recommended)
Mechanism
Lowering urine pH causes weak base drugs (amphetamines, PCP) to become ionized (positively charged) → cannot be reabsorbed → excreted faster.
Why It Is NOT Done
| Reason | Explanation |
|---|---|
| Rhabdomyolysis risk | Amphetamines and PCP commonly cause rhabdomyolysis. Acidifying urine causes myoglobin to precipitate in renal tubules → acute tubular necrosis / acute renal failure |
| Modest benefit | The increase in elimination doesn't outweigh the renal danger |
| MAOI overdose | Acidification is ineffective AND predisposes to acute renal failure |
"Acidification may increase the urine concentration of drugs such as phencyclidine and amphetamines but is not advised because it may worsen renal complications from rhabdomyolysis, which often accompanies the intoxication." - Katzung
Side-by-Side Comparison
| Feature | Urinary Alkalinization | Urinary Acidification |
|---|---|---|
| Target drug type | Weak ACIDS | Weak BASES |
| Mechanism | Ion trapping of anions | Ion trapping of cations |
| Agent used | IV sodium bicarbonate | Ammonium chloride / ascorbic acid (historical) |
| Target urine pH | 7.5-8.0 | <5.5 |
| Key drugs | Salicylates, phenobarbital, methotrexate | Amphetamines, PCP (theoretical only) |
| Currently recommended? | Yes (for salicylates especially) | No (abandoned - rhabdomyolysis risk) |
| Major hazard | Hypokalemia (blocks alkalinization), systemic alkalemia | Acute renal failure from myoglobin precipitation |
| Extra benefit | Prevents CNS penetration of salicylate | None |
Key Exam Points
- Urinary alkalinization = NaHCO₃ + KCl (always correct hypokalemia)
- It is 1st-line for moderate salicylate poisoning not meeting hemodialysis criteria
- Urinary acidification is historically taught but clinically abandoned
- Forced diuresis alone (without pH change) is also not recommended - causes volume overload without meaningful benefit (except possibly in lithium poisoning)
Sources: Goldman-Cecil Medicine; Goodman & Gilman's Pharmacology; Katzung Basic & Clinical Pharmacology; Rosen's Emergency Medicine; Washington Manual of Medical Therapeutics
Give any tricks to remember poision and antidote
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Perfect - comprehensive antidote table retrieved. Now here's the full memory trick guide:
Poison & Antidote - Memory Tricks
Group 1: The "OPIOID Reversal" Pair - Easy One First
| Poison | Antidote | Trick |
|---|---|---|
| Opioids (morphine, heroin, fentanyl) | Naloxone | NALoxone = NALls the opioid down. "NALl it shut" |
| Benzodiazepines (diazepam) | Flumazenil | FLUmazenil FLUshes out the benzo. Flu clears the sedation |
Group 2: The Famous Trio - Organophosphates (OP)
"ATROPINE PRALIDOXIME for OPs - ATP for energy, ATPase for nerve"
| Poison | Antidote | Trick |
|---|---|---|
| Organophosphates / carbamates / nerve agents | Atropine (1st) + Pralidoxime / 2-PAM (2nd) | Atropine for All symptoms (dries secretions), Pralidoxime to Prevent aging of AChE |
- Atropine blocks muscarinic effects (SLUDGE)
- Pralidoxime reactivates AChE if given early (before "aging")
- Mnemonic: "AP for OP" = Atropine + Pralidoxime for OrganoPosphate
Group 3: Heavy Metals - The Chelators
"BAD metals need BAL or DMSA"
| Poison | Antidote | Trick |
|---|---|---|
| Lead | Dimercaprol (BAL) + CaNa₂EDTA or Succimer (DMSA) | Lead = Lots of chelators. "EDTA grabs Lead" |
| Mercury | Dimercaprol (BAL) / Succimer | Mercury → Mercaprol (both start with Mer-) |
| Arsenic | Dimercaprol (BAL) / Succimer | Arsenic → BAL (British Anti-Lewisite - used in WWI arsenic warfare) |
| Iron | Deferoxamine | Deferoxamine Drags out iron = De-iron-amine |
| Thallium/Cesium | Prussian Blue | Thallium → "Thallium turns Prussian Blue" (used in nuclear accidents) |
BAL trick: BAL = Bad Arsenic Lead (+ mercury) - covers all 3
Group 4: Carbon & Cyanide - The "Gas Killers"
| Poison | Antidote | Trick |
|---|---|---|
| Carbon Monoxide | 100% O₂ (± hyperbaric) | CO kicks O₂ off Hb → flood with O₂ to kick CO back off |
| Cyanide | Hydroxycobalamin (1st line) OR Sodium nitrite + Sodium thiosulfate | "Cyanide → Cyanocobalamin cousin = Hydroxycobalamin" |
Cyanide antidote logic:
- Nitrite creates methaemoglobin → CN prefers metHb over cytochrome (diverts it)
- Thiosulfate donates sulfur → rhodanese converts CN → thiocyanate (harmless, excreted)
- Mnemonic: "NiNa NiNa" = Nitrite + Na thiosulfate (like a siren - emergency!)
Group 5: Paracetamol / Acetaminophen
| Poison | Antidote | Trick |
|---|---|---|
| Paracetamol (APAP) | N-Acetylcysteine (NAC) | "Paracetamol → NACk it with NAC"**. NAC replenishes glutathione to neutralize NAPQI |
NAPQI is the toxic metabolite. NAC = glutathione substitute. Give within 8-10 hours.
Group 6: Anticoagulants - Reverse the Clot Stoppers
| Poison / Drug | Antidote | Trick |
|---|---|---|
| Warfarin / Coumarins | Vitamin K₁ (Phytonadione) | War-far-in is far from clotting → K brings it back |
| Heparin | Protamine sulfate | Heparin → Protamine (Pro is the opposite/antidote) |
| Dabigatran (direct thrombin inhibitor) | Idarucizumab | Idarucizumab Ida-reverses Dabigatran (Ida ~ reversal of Da) |
| Rivaroxaban / Apixaban (Xa inhibitors) | Andexanet alfa | Andexanet for Xa (factor Xa inhibitors) |
Group 7: Receptor Blockers & Overdoses
| Poison | Antidote | Trick |
|---|---|---|
| Beta-blockers | Glucagon + High-dose insulin | Glucagon for β-Gone heart rate. Glucagon bypasses the blocked β-receptor |
| Calcium channel blockers | Calcium + Glucagon + High-dose insulin | CCB → give Calcium to compete |
| Digoxin/Digitalis | Digoxin-immune Fab | Fabulous Fab fragments Fabulate the digoxin away |
| Anticholinergic (atropine OD, antihistamines) | Physostigmine | Anticholinergic → Physostigmine (cholinesterase inhibitor = restores ACh) |
| Methemoglobinemia (nitrites, dapsone) | Methylene Blue | Met-Hb is blue → Methylene Blue fixes blue blood |
Group 8: Metabolic Poisons
| Poison | Antidote | Trick |
|---|---|---|
| Methanol / Ethylene glycol | Fomepizole (4-MP) | Fomepizole Freezes alcohol dehydrogenase - stops toxic metabolite formation |
| Isoniazid (INH) / Gyromitra mushroom | Pyridoxine (Vit B₆) | INH depletes B₆ → "INH eats B₆, give it back" |
| Methotrexate | Leucovorin (folinic acid) + Glucarpidase | MTX blocks folate → Leucovorin = Rescue folate |
| Sulfonylurea hypoglycemia | Octreotide | Octreotide Octopus grabs and stops insulin release |
| Local anesthetics (bupivacaine toxicity) | Intralipid (IV fat emulsion) | Fat soaks up fat-soluble drug - "lipid sink" |
Master Memory Table - "ABCDEFGH" Framework
| Letter | Poison | Antidote |
|---|---|---|
| A | Acetaminophen | Acetylcysteine (NAC) |
| B | Benzodiazepines | Flumazenil (Benzo → Flush) |
| C | Cyanide | Hydroxycobalamin / NaNO₂ + Na-thiosulfate |
| D | Digoxin | Digoxin-immune Fab |
| E | Ethylene glycol / mEthanol | Fomepizole |
| F | Fluoride / Ca-channel blocker | Calcium gluconate |
| G | β-blockers (Gone HR) | Glucagon |
| H | Heparin | Protamine |
| I | Iron | Deferoxamine |
Quick-Fire Mnemonics Summary
| Mnemonic | Covers |
|---|---|
| "NAL nails opioids" | Naloxone → opioids |
| "FLU flushes benzos" | Flumazenil → benzodiazepines |
| "AP for OP" | Atropine + Pralidoxime → Organophosphates |
| "BAL for BAd metals" | BAL/Dimercaprol → Lead, Arsenic, Mercury |
| "De-iron-amine" | Deferoxamine → Iron |
| "NiNa NiNa" | Nitrite + Na-thiosulfate → Cyanide |
| "NAC-k Paracetamol" | N-Acetylcysteine → Paracetamol |
| "Fab-ulous for Digoxin" | Digoxin-immune Fab → Digoxin |
| "Fomepizole Freezes ADH" | Fomepizole → Methanol / Ethylene glycol |
| "INH eats B₆" | Pyridoxine → INH / Gyromitra mushroom |
| "Methylene blue for blue blood" | Methylene blue → MetHb |
| "Fat sink for fat drugs" | Intralipid → local anesthetic toxicity |
| "War-farin → War needs K to stop" | Vitamin K → Warfarin |
| "Prussian Blue for Thallium" | Prussian Blue → Thallium/Cesium |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 9-14; Lippincott Illustrated Reviews Pharmacology; Park's Textbook of Preventive and Social Medicine
Acid corrosives vs alkali corrosives
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Complete picture. Here's the full comparison:
Acid Corrosives vs Alkali Corrosives
1. Basic Definitions & Examples
| Feature | Acid Corrosives | Alkali Corrosives |
|---|---|---|
| pH | <7 | >7 |
| Common agents | Sulfuric acid (H₂SO₄), Hydrochloric acid (HCl), Nitric acid (HNO₃), Formic acid, Acetic acid | Sodium hydroxide/lye (NaOH), Potassium hydroxide (KOH), Ammonia (NH₃), Sodium hypochlorite (bleach) |
| Found in | Toilet bowl cleaners, pool cleaners, rust removers, battery acid | Drain cleaners (Drano), oven cleaners, hair relaxers, dish detergents, industrial bleach |
| Other name | Corrosives | Caustics |
2. Mechanism of Injury - THE KEY DIFFERENCE
| Acid | Alkali | |
|---|---|---|
| Type of necrosis | Coagulation necrosis | Liquefaction necrosis |
| Mechanism | H⁺ ions denature proteins → form a coagulum (gel-like eschar) on mucosa | OH⁻ ions cause protein denaturation + lipid saponification → deep tissue destruction + microvascular thrombosis |
| Depth of injury | Coagulum limits penetration - relatively self-limiting | No limiting barrier - penetrates deeply into all tissue layers |
| Severity | Generally less severe | More severe - progressive, worsening with time |
Memory trick: Acid = Armour (coagulum forms a protective shell). Alkali = Attacks everywhere (no barrier, melts through)
3. Anatomical Distribution of Injury
| Site | Acid | Alkali |
|---|---|---|
| Oropharynx | Less affected (bitter taste + gag reflex limits ingestion) | More affected (especially solid/powder forms - lye crystals) |
| Esophagus | Relatively spared (coagulum protects) though recent endoscopy data shows equal esophageal injury rates | Primary site of injury (full-thickness burns, circumferential strictures) |
| Stomach | Main target - acid settles in stomach, increased pH → deeper penetration → pyloric stenosis, gastric outlet obstruction, perforation | Can be affected with large intentional ingestions |
| Beyond GI | Systemic absorption → metabolic acidosis, hemolysis, renal failure | Deep penetration → mediastinitis, pancreatitis, peritonitis |
Trick: Acid hits the Abdomen (stomach). Alkali hits the Airway and Airpipe (esophagus, pharynx)
4. Esophageal Burn Grading (Zargar Classification)
| Grade | Endoscopic Finding | Risk |
|---|---|---|
| 0 | Normal | None |
| 1 | Mucosal edema + hyperemia | No stricture |
| IIa | Superficial, non-circumferential ulcers, whitish membranes | Low stricture risk |
| IIb | Deep, circumferential lesions | High stricture risk |
| IIIa | Small scattered areas of necrosis | Very high |
| IIIb | Extensive necrosis | Surgical |
| IV | Perforation | Emergency surgery |
Critical period: Days 2-14 after injury = maximum tissue friability + perforation risk (both spontaneous and iatrogenic)
5. Clinical Features (Both)
| Symptom | Mechanism |
|---|---|
| Vomiting (most common) | Direct mucosal irritation |
| Dysphagia / odynophagia | Esophageal burn |
| Drooling | Cannot swallow saliva |
| Oral/chest/abdominal pain | Mucosal/transmural injury |
| Hoarseness, stridor | Laryngeal/epiglottic injury - "chemical epiglottitis" |
| Dribble burns on face/chest | Streaks from spillage - acid ingestion classic sign |
| Fever + chest pain | Mediastinitis / perforation |
| Hypotension | Shock (hemorrhage, perforation, third-spacing) |
6. Management - What NOT to Do
| ❌ Contraindicated | Reason |
|---|---|
| Activated charcoal | Doesn't bind caustics; obscures endoscopy |
| Emetics / Ipecac | Re-exposes mucosa + airway to caustic on the way back up; can cause perforation |
| Neutralization (giving acid for alkali and vice versa) | Exothermic reaction → more heat damage + distension + vomiting |
| Dilution | No proven benefit; causes distension, vomiting |
| Blind NGT insertion | Risks perforation of injured esophagus |
| Gastric lavage | Absolute contraindication (perforation risk) |
| Blind nasotracheal intubation | Can worsen airway injury |
7. Management - What TO Do
Step 1 - Airway (FIRST priority)
- Approach as difficult airway - oedema worsens with time
- Early oral intubation under direct vision
- Fiberoptic evaluation before intubation if possible
- Cricothyrotomy if intubation impossible
Step 2 - Decontamination
- Remove contaminated clothing
- Copious water irrigation of skin/eyes
- DO NOT neutralize
Step 3 - Investigations
- ABG, electrolytes, LFTs, FBC, lactate, blood type & screen
- Chest X-ray - look for mediastinal/peritoneal free air
- CT thoracoabdomen (IV contrast) - better than endoscopy at predicting stricture depth and need for surgery
- Endoscopy - gold standard for grading; do within 12-24 hours; mandatory for all intentional ingestions
Step 4 - Supportive
- Large-bore IV + crystalloid resuscitation
- Nil by mouth
- Analgesia
- PPI / H2 blockers
Step 5 - Steroids?
- Controversial - one trial showed benefit for grade IIb lesions
- Meta-analysis: no clear benefit + may increase infection/perforation risk
- Currently not routinely recommended
Side-by-Side Summary
| Feature | Acid | Alkali |
|---|---|---|
| Necrosis type | Coagulation | Liquefaction |
| Depth | Superficial (self-limiting eschar) | Deep (progressive, no barrier) |
| Primary site | Stomach (pyloric stenosis, GOO) | Esophagus (strictures) |
| Severity | Less severe | More severe |
| Systemic toxicity | Metabolic acidosis, hemolysis, renal failure | Mediastinitis, pancreatitis, peritonitis |
| Stricture risk | Lower | Higher (especially Grade IIb+) |
| Both contraindicated | Lavage, charcoal, emetics, neutralization | Same |
Sources: Tintinalli's Emergency Medicine Ch. 200; Cummings Otolaryngology Ch. 211; Rosen's Emergency Medicine; Tintinalli's EM - Alkali Injuries
Give information for undergraduate level with full clarification
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - full forensic textbook data retrieved. Now delivering the complete undergraduate-level guide:
Acid Corrosives vs Alkali Corrosives
Complete Undergraduate Guide
PART 1: INTRODUCTION & DEFINITIONS
A corrosive poison is a chemical agent that destroys living tissue immediately upon contact by direct chemical action, before any systemic absorption is needed. This distinguishes it from a systemic poison (like cyanide) which must be absorbed first to cause harm.
- Corrosive = derived from Latin corrodere = "to gnaw through flesh"
- Caustic = strictly refers to alkalis/bases, but clinically used interchangeably with "corrosive"
- Some agents are BOTH corrosive AND poison (e.g., phenol = local corrosive + systemic CNS depressant)
Two major groups:
- Acid corrosives - pH <7
- Alkali (caustic) corrosives - pH >7
PART 2: ACID CORROSIVES
2A. SULFURIC ACID (H₂SO₄) - "Oil of Vitriol" - The Most Important
Physical Characters:
- Pure form: heavy, odorless, colorless, non-fuming, oily hygroscopic liquid
- Commercial form: brown or dark colored (due to impurities)
- Causes superficial burns in 1 second; full-thickness burns in 30 seconds
- Strongly hygroscopic - absorbs water from tissues causing dehydration injury
Mechanism:
Coagulation necrosis - H⁺ ions denature surface proteins → form a hard, leathery coagulum (eschar) → this eschar limits further penetration (self-limiting at mucosa level, BUT not in stomach where acid pools)
Signs & Symptoms (Ingestion):
| System | Feature |
|---|---|
| Lips/mouth | Swollen, excoriated; brown/black streaks from angles of mouth to chin ("dribble burns") |
| Teeth | Chalky-white |
| Tongue | Swollen, sodden, black |
| Throat/esophagus | Burning pain, stridor, odynophagia, dysphagia |
| Stomach | Epigastric pain spreading all over abdomen; vomiting - vomit is brown/black, mucoid, strongly acid, may contain charred stomach wall shreds |
| Thirst | Intense, but any attempt to drink causes more vomiting |
| Bowels | Severe constipation + tenesmus |
| Voice | Hoarse and husky |
| Eyes | Sunken; pupils dilated |
| Sensorium | Mind remains clear till death (classic exam point) |
Fatal Dose: 10-15 mL
Fatal Period: 12-24 hours
Cause of Death:
- Circulatory collapse (shock)
- Spasm or edema of glottis → asphyxia
- Perforation of stomach → peritonitis
- Toxemia
- Delayed: hypostatic pneumonia, secondary infection, renal failure, starvation from esophageal stricture
Complications:
| Acute | Chronic |
|---|---|
| Upper airway obstruction | Esophageal stricture/obstruction |
| GI hemorrhage | Pyloric stenosis |
| Esophageal/gastric perforation | Vocal cord paralysis |
| Sepsis | Permanent skin/oropharyngeal scars |
| Tracheobronchial necrosis, atelectasis |
Postmortem Appearances:
External:
- Corrosion of lips, mouth, throat, skin at chin angles and hands
- Necrotic areas: initially greyish-white → become brown or black and leathery
- Examine clothing for burns and stains
Internal:
- Upper digestive tract inflamed and edematous even when corrosion is absent
- Acid hematin forms in stomach → contents brown or black, gelatinous
- Stomach wall soft, friable; gastric mucosa may be detached in patches
- Esophageal mucosa shows longitudinal erosions and corrosion
- Intestines usually spared; upper duodenum may be affected
- Kidneys: swollen, congested; tubules may contain hemoglobin casts
- Thickening of wall due to intense inflammatory reaction
Chemical Test:
- Barium nitrate or chloride solution → white precipitate of barium sulphate (confirms sulfate)
- Strong acid chars organic matter
Circumstances of Poisoning:
- Accidental - mistaken for glycerin or castor oil; inhalation in chemical factories
- Suicidal - most common
- Homicidal - rare (bitter taste, immediate local action, obvious physical changes make detection easy)
- Used as abortifacient by vaginal injection
- VITRIOLAGE - throwing acid on another person (see below)
2B. VITRIOLAGE (Acid Attack)
"Throwing of sulfuric acid on another individual is known as vitriolage"
- Burns are initially painless (due to nerve ending damage)
- Penetrating burns - acid devitalizes tissue and predisposes to infection
- Repair is slow; scar tissue causes contracture
- Blindness if eyes involved
- Death from shock or toxemia if extensive area involved
- Other agents also used: nitric acid, carbolic acid, corrosive alkali, juice of marking nut (Semecarpus anacardium), calotropis
Medicolegal aspect (BNS Section 124):
Causing permanent/partial damage by throwing or administering acid = imprisonment not less than 10 years (up to life) + fine. The fine is paid to the victim.
2C. NITRIC ACID (HNO₃) - "Aqua Fortis" / "Red Spirit of Niter"
Physical Characters:
- Clear, colorless, fuming, heavy liquid with peculiar choking odor
Hallmark Feature:
YELLOW discoloration of tissues - due to xanthoproteic reaction (reaction with proteins produces picric acid)
- Yellow stains on clothing, yellow discoloration of skin, crowns of teeth, urine (brown)
Signs & Symptoms: Same as sulfuric acid PLUS:
- More eructation and greater abdominal distension (due to gas formation)
- Lachrymation, photophobia on inhalation of fumes → sneezing, coughing, dyspnoea, asphyxia
Fatal Dose: 10-15 mL | Fatal Period: 12-24 hours
Postmortem: Similar to H₂SO₄ but with characteristic YELLOW staining of tissues. May appear brown-black due to acid hematin. Stomach wall soft, friable, ulcerated.
Test: Brown ring test - add ferrous sulphate solution + sulphuric acid to a solution containing nitric acid → brown ring forms at the junction of two fluids
2D. HYDROCHLORIC ACID (HCl) - "Muriatic Acid"
Physical Characters:
- Pungent, colorless, fuming liquid
- Natural constituent of gastric juice
Key Distinction:
- Less corrosive than H₂SO₄
- Does not usually corrode skin seriously, but readily destroys mucous membrane
- Mucous membrane initially grey or grey-white → later dark
Fatal Dose: 15-20 mL | Fatal Period: 12-24 hours
2E. OXALIC ACID - "Special Organic Acid"
Unique mechanism: Unlike mineral acids, oxalic acid exerts BOTH local corrosive AND systemic toxic effects
Three Phases of Poisoning:
- Local/Corrosive phase: Whitened, "bleached" mucosa of esophagus; corrugated with longitudinal erosions; gastric mucosa reddened/black; gelatinous brown stomach contents (acid hematin)
- Systemic/Convulsive phase: Hypocalcemia (oxalate binds Ca²⁺) → muscle irritability, tetany, convulsions, numbness/tingling of fingertips and legs, cardiovascular collapse
- Delayed phase: Uremia - scanty/suppressed urine with blood, albumin, calcium oxalate crystals; metabolic acidosis; ventricular fibrillation
Postmortem: Kidneys swollen, congested; tubules filled with oxalate crystals; proximal convoluted tubules necrosed
Antidote: Calcium (any form - lime water, calcium lactate, calcium gluconate) - converts oxalate to insoluble calcium oxalate + IV Calcium gluconate 10% 10mL
Test: Barium nitrate → white precipitate of barium oxalate (soluble in HCl/HNO₃)
2F. CARBOLIC ACID (Phenol; C₆H₄OH) - "Carbolism"
Unique features:
- BOTH a corrosive AND a systemic poison
- Rapidly absorbed through ALL routes (skin, GI, rectum, vagina, serous cavities, wounds, lungs)
- Characteristic carbolic/phenolic smell
Fatal Dose: 10-15 g | Fatal Period: 3-4 hours (much faster than mineral acids)
Local Effects:
- Skin: burning + numbness (damages nerve endings); hard, cracked, whitish surfaces; deep burns are black; white opaque painless eschar that falls off leaving brown stain
- GI: burning pain mouth to stomach; white/grey corrugated mucosa
Systemic Effects (CNS Depressant):
- Excitement → narcosis → unconsciousness → death
- Respiratory failure (CNS depression)
- Dark/smoky brown urine (phenol metabolites - hydroquinone, pyrocatechol)
Test: Add 10% ferric chloride to urine → bluish colour (also positive with salicylates)
Key exam point: Phenol is about 8 times more toxic than Lysol (Lysol = 50% cresol in saponified vegetable oil)
PART 3: ALKALI CORROSIVES (CAUSTIC ALKALIS)
Chief Alkali Poisons:
Sodium hydroxide (NaOH/lye/caustic soda), Potassium hydroxide (KOH), Calcium hydroxide (lime), Ammonia (NH₃/NH₄OH), Ammonium carbonate, Potassium carbonate, Sodium carbonate
Mechanism of Action (The Core Difference from Acids)
The hydroxyl (OH⁻) ion:
- Saponification of fats (dissolves cell membranes)
- Soluble alkaline proteinases destroy proteins
- Cellular dehydration
- Exothermic reaction (generates heat - additional damage)
- Liquefaction necrosis: OH⁻ passes from molecule to molecule, denaturing each in turn, burrowing deeply → soft, gelatinous, friable eschars
- No limiting barrier forms - unlike acid's coagulum, there is no protective layer → injury is PROGRESSIVE and worsens with time
LYE (NaOH) can produce transmural necrosis of esophagus after just 1 second of contact
Primary Site: Esophagus
"Ingestion of an alkali produces severe effects mainly on lining of esophagus, while gastric involvement is less common. Therefore, stricture formation is much more common with alkalis than with acids."
Signs & Symptoms
| Feature | Detail |
|---|---|
| Taste | Acrid, caustic ("soapy") |
| Vomiting | Vomited matter is alkaline, does not effervesce on contact with ground; thick and slimy at first, later dark altered blood + shreds of mucosa |
| Bowels | Purging (frequent) with severe pain, straining; motions of mucus and blood |
| Skin contact | Greyish, soapy, necrotic area |
| Lips/skin near mouth | Abrasions, blisters, brownish discoloration |
| GI mucosa | Swollen, soft, grey slough readily detached |
| Long-term | Esophageal stricture |
Fatal Dose:
- NaOH/KOH: 5 g
- K₂CO₃: 18 g
- Na₂CO₃: 30 g
- Ammonia: 15-20 mL
Fatal Period: Usually 24 hours
Postmortem Appearances
- Marks around mouth: dark, parchment-like
- Lips, mouth, throat: evident corrosion
- Pronounced inflammatory edema
- Esophageal and gastric tissues: corrosion + sliminess (contrast with acid's leathery, dry eschar)
- Stomach: similar soft, slimy necrosis
Ammonia Vapor Inhalation
- Congestion and watering of eyes
- Violent sneezing, coughing, choking
- Sudden collapse from suffocation due to inflammation and swelling of glottis
- Later: pneumonia
Miniature (Button) Batteries
Contain potassium hydroxide - when swallowed can cause liquefaction necrosis following leakage from battery. Symptoms mostly GI tract.
PART 4: STAGES OF ESOPHAGEAL INJURY (Both Acid & Alkali)
| Stage | Timing | Pathology |
|---|---|---|
| Acute inflammatory | 0-4 days | Edema, hemorrhage, eosinophilic necrosis, bacterial invasion |
| Ulceration/necrosis | 4-7 days | Bacterial invasion, saponification, full-thickness necrosis |
| Perforation risk | 7-21 days | Tissue at its WEAKEST - highest risk of spontaneous or iatrogenic perforation |
| Cicatrization (scarring) | From ~3rd week, persists years | Excessive scar tissue → stricture formation |
⚠️ Do NOT perform endoscopy or pass NG tubes during days 7-21 without extreme caution - this is the highest perforation risk window.
Zargar Endoscopic Grading
| Grade | Findings | Risk |
|---|---|---|
| 0 | Normal | None |
| 1 | Mucosal edema + hyperemia | No stricture |
| IIa | Superficial, non-circumferential ulcers, whitish exudates | Low stricture risk |
| IIb | Deep, circumferential lesions | High stricture risk |
| IIIa | Small scattered necrosis | Very high |
| IIIb | Extensive necrosis | Surgical |
| IV | Perforation | Emergency |
PART 5: COMPARATIVE TABLE - ACID vs ALKALI
| Feature | Acid Corrosives | Alkali Corrosives |
|---|---|---|
| pH | <7 | >7 |
| Necrosis type | Coagulation (protein denaturation → hard eschar) | Liquefaction (saponification of fat + protein denaturing → soft, gelatinous eschar) |
| Depth of injury | Superficial (coagulum limits penetration) | Deep and progressive (no limiting barrier) |
| Primary injury site | Stomach (acid pools here) | Esophagus (contact during swallowing) |
| Stricture formation | Less common | Much more common |
| Vomit character | Brown/black, acid reaction | Alkaline, thick, slimy, does not effervesce |
| Eschar character | Hard, dry, leathery, brown/black | Soft, gelatinous, slimy, grey |
| Severity | Less severe overall | More severe (progressive destruction) |
| Oropharyngeal injury | Bitter taste limits ingestion; less | More severe (especially solid forms) |
| Systemic toxicity | Metabolic acidosis, hemolysis, renal failure (especially HCl, H₂SO₄) | Mediastinitis, pancreatitis, multi-organ injury (severe intentional ingestions) |
| Fatal period | 12-24 hours | ~24 hours |
PART 6: GENERAL MANAGEMENT
Do NOT Do (Both Acids and Alkalis)
| ❌ | Reason |
|---|---|
| Gastric lavage | Risk of perforation through injured tissue |
| Emetics/Ipecac | Reexposes mucosa + airway to corrosive |
| Activated charcoal | Doesn't bind corrosives; blocks endoscopy view |
| Neutralization (acid for alkali or vice versa) | Exothermic reaction + CO₂ gas production → distension + vomiting + rupture |
| Alkaline carbonates/bicarbonates for acid (internally) | Liberate CO₂ → gastric distension → rupture |
| Blind NG tube insertion | Perforation |
| Blind nasotracheal intubation | Worsens airway injury |
What TO Do
Airway first - approach as difficult airway; early fiberoptic assessment; early intubation before oedema worsens; tracheostomy if needed
Skin/Eye Burns:
- Wash with plenty of water + soap
- Acid burns: apply thick paste of magnesium oxide/carbonate (for skin) or sodium bicarbonate solution (for eyes)
- Alkali burns: same copious water irrigation
Oral ingestion (if within 5-30 minutes and patient conscious):
- Give water or milk (dilution/demulcent) - 250 mL
- Demulcents: egg whites, olive oil, milk, starch water, mineral oil, melted butter
IV access + crystalloid resuscitation
NPO + parenteral nutrition for ~1 week, then gradual reintroduction
Endoscopy: within 12-24 hours of ingestion to grade injury (gold standard)
CT scan (IV contrast): Better than endoscopy for predicting stricture and depth; recommended by World Society of Emergency Surgery
Steroids (prednisolone 60 mg/day): Controversial; may prevent stricture formation in Grade IIb - not routinely recommended due to increased perforation/infection risk
Dilation (bougienage): 4 cm mercury-filled bougie daily if stricture develops
Surgery (exploratory laparotomy): If circumferential 2nd/3rd degree burns or gastric necrosis; esophagogastrostomy may be needed
PART 7: MEDICOLEGAL ASPECTS
| Aspect | Acid | Alkali |
|---|---|---|
| Accidental | Common - mistaken for other liquids, industrial inhalation | Less common |
| Suicidal | Most cases | Less common than acid |
| Homicidal | Rare (taste + immediate pain make detection easy) | Rare |
| Abortifacient | Vaginal injection - acid | Less used |
| Special crime | VITRIOLAGE (acid throwing) - legally a serious crime | Used less for vitriolage |
| BNS Section 124 | Acid attack = min 10 years imprisonment + fine to victim | Applicable |
PART 8: MEMORY TRICKS
| Trick | Content |
|---|---|
| "Acid = Armour" | Coagulation forms a protective eschar - self-limiting |
| "Alkali = Attacks ALL layers" | Liquefaction, no barrier, progressive |
| "Acid hits the Abdomen, Alkali hits the Airway/Alimentary tube" | Stomach vs Esophagus predominance |
| "Alkali Strictures > Acid Strictures" | Because no self-limiting barrier |
| "Vomit = Acid? Brown/black + acid reaction. Alkali? Slimy, alkaline, no effervesce" | Distinguishing vomit character |
| "Nitric acid = Yellow" | Xanthoproteic reaction → yellow staining of tissues, teeth, clothing |
| "Phenol = fast death (3-4h) + brown urine + blue FeCl₃ test" | Unique features of carbolic acid |
| "Oxalic acid = Convulsions + Crystals" | Hypocalcemia → tetany; oxalate crystals in kidney |
| "7-21 days = Most dangerous perforation window" | For esophageal tissue post-caustic injury |
| "No neutralization EVER" | Exothermic + gas → more damage |
Sources: The Essentials of Forensic Medicine and Toxicology 36th Ed (2026); Tintinalli's Emergency Medicine; Cummings Otolaryngology; Rosen's Emergency Medicine
Sulpharic acid poisoning
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is the complete, dedicated undergraduate account of sulfuric acid poisoning:
Sulfuric Acid (H₂SO₄) Poisoning
Synonyms
- Oil of Vitriol (historical name)
- "Vitriol" in forensic/legal context
Physical Characteristics
| Property | Detail |
|---|---|
| Appearance | Pure: heavy, colorless, odorless, non-fuming, oily liquid |
| Commercial form | Brown or dark colored (due to impurities) |
| Nature | Hygroscopic (absorbs water greedily from tissues) |
| Special property | Strong tendency to carbonize (char) organic substances |
| Speed of injury | Superficial burns in 1 second; full-thickness burns in 30 seconds |
Mechanism of Injury
Coagulation necrosis:
- H⁺ ions denature surface proteins → form a hard, dry, leathery coagulum (eschar)
- The coagulum acts as a partial barrier - limits further acid penetration into the esophagus
- However, acid flows down to the stomach (lesser curvature → pylorus), where initial pyloric spasm traps acid → deepest injury at the stomach and pylorus
- Hygroscopic nature - absorbs water from cells → additional dehydration injury
- Exothermic reaction with water in tissues generates heat → thermal injury on top of chemical injury
Signs and Symptoms
Mouth and Face
- Lips: swollen and excoriated
- Brown or black streaks extending from angles of mouth → sides of chin → front of neck (due to flow of acid = "dribble burns")
- Teeth: chalky-white (acid dissolves enamel)
- Tongue: swollen, sodden, and black
Throat and Esophagus
- Pharyngeal pain - most common presenting symptom
- Immediate burning pain, stridor
- Drooling, odynophagia, dysphagia
- Voice becomes hoarse and husky
Gastrointestinal
- Epigastric pain spreading all over the abdomen and thorax
- Eructation, nausea, vomiting
- Vomit character: brown or black, mucoid, strongly acid, may contain shreds of the charred stomach wall
- Intense thirst - but any attempt to drink causes more vomiting
- Abdomen becomes distended and very tender
- Severe constipation + tenesmus
Systemic
- Eyes: sunken; pupils usually dilated
- Circulatory collapse (shock) - may cause immediate death
- Asphyxia from edema of glottis
- Mind remains clear till death (⚠️ classic exam point - sensorium preserved unlike many other poisons)
If the Patient Survives
- Late esophageal, gastric and pyloric strictures and stenoses
- Permanent scars on skin and oropharynx
Fatal Dose and Period
| Fatal Dose | 10-15 mL |
| Fatal Period | 12-24 hours |
Cause of Death
| Immediate | Delayed |
|---|---|
| 1. Circulatory collapse | Hypostatic pneumonia |
| 2. Spasm/edema of glottis → asphyxia | Secondary infection |
| 3. Perforation of stomach → peritonitis | Renal failure |
| 4. Toxemia | Starvation from esophageal stricture |
Complications
Acute
- Upper airway obstruction and injury
- GI hemorrhage
- Esophageal and gastric perforation
- Sepsis
- Tracheobronchial necrosis, atelectasis, obstructive lung injury
Chronic
- Esophageal obstruction (stricture)
- Pyloric stenosis
- Vocal cord paralysis with airway obstruction
Time Course of Esophageal/Gastric Injury
| Stage | Timing | What Happens |
|---|---|---|
| Acute inflammatory | 0-4 days | Edema, hemorrhage, granulation begins |
| Granulation | 4-7 days | Tissue forming, still necrotic |
| Perforation risk | 7-21 days | Tissue at its weakest - maximum perforation risk |
| Cicatrization (scarring) | From ~3rd week | Stricture formation; may persist for years |
Treatment
What NOT to Do
| ❌ | Reason |
|---|---|
| Gastric lavage | Perforates damaged stomach wall |
| Emetics | Re-exposes mucosa to acid |
| Alkaline carbonates or bicarbonates orally | Liberate CO₂ → gastric distension → rupture |
What TO Do
Step 1 - Dilute and neutralize in-situ (within 30 minutes of ingestion):
Give 250 mL (one-fourth liter) of any of the following:
- Water or milk (first choice)
- Milk of magnesia
- Lime water
- Soap suds
- Aluminium hydroxide gel
⚠️ Do NOT use alkaline carbonates/bicarbonates (NaHCO₃) - they release CO₂ gas, cause gastric distension and may rupture the stomach
Step 2 - Demulcents (soothing, coating agents):
Olive oil, milk, egg whites, starch water, mineral oil, melted butter
Step 3 - Airway:
- Tracheostomy if edema of glottis develops
Step 4 - Nothing by mouth:
- IV nutrition for ~1 week
- Then: liquids → soft food → regular diet gradually
Step 5 - Endoscopy:
- Flexible fiberoptic endoscopy within 24-48 hours to assess extent of damage to esophagus and stomach
- If circumferential 2nd/3rd degree burns → exploratory laparotomy
- If gastric necrosis → esophagogastrostomy
Step 6 - Steroids:
- Prednisolone 60 mg/day in divided doses to prevent esophageal stricture
- Generally NOT recommended due to increased perforation risk
Step 7 - Stricture management:
- 4 cm diameter mercury-filled bougie passed daily if stricture develops
Step 8 - Skin burns:
- Wash with large amounts of water
- Apply paste of magnesium oxide or sodium bicarbonate
Step 9 - Eye burns:
- Irrigate with water or sodium bicarbonate solution for 10-15 minutes
- Ideal: suspended IV bag providing low-pressure continuous irrigation
- Instill a few drops of olive oil or castor oil after irrigation
Step 10 - Symptomatic - analgesia, antibiotics, IV fluids
Postmortem Appearances
External
- Corrosion of lips, mouth, throat, skin at chin angles and hands
- Necrotic areas: initially greyish-white → become brown or black and leathery
- Examine clothing for acid burns and stains
- If acid taken from a spoon - lips and mouth may escape injury
Gross pathology image - Stomach in Sulfuric Acid Poisoning:
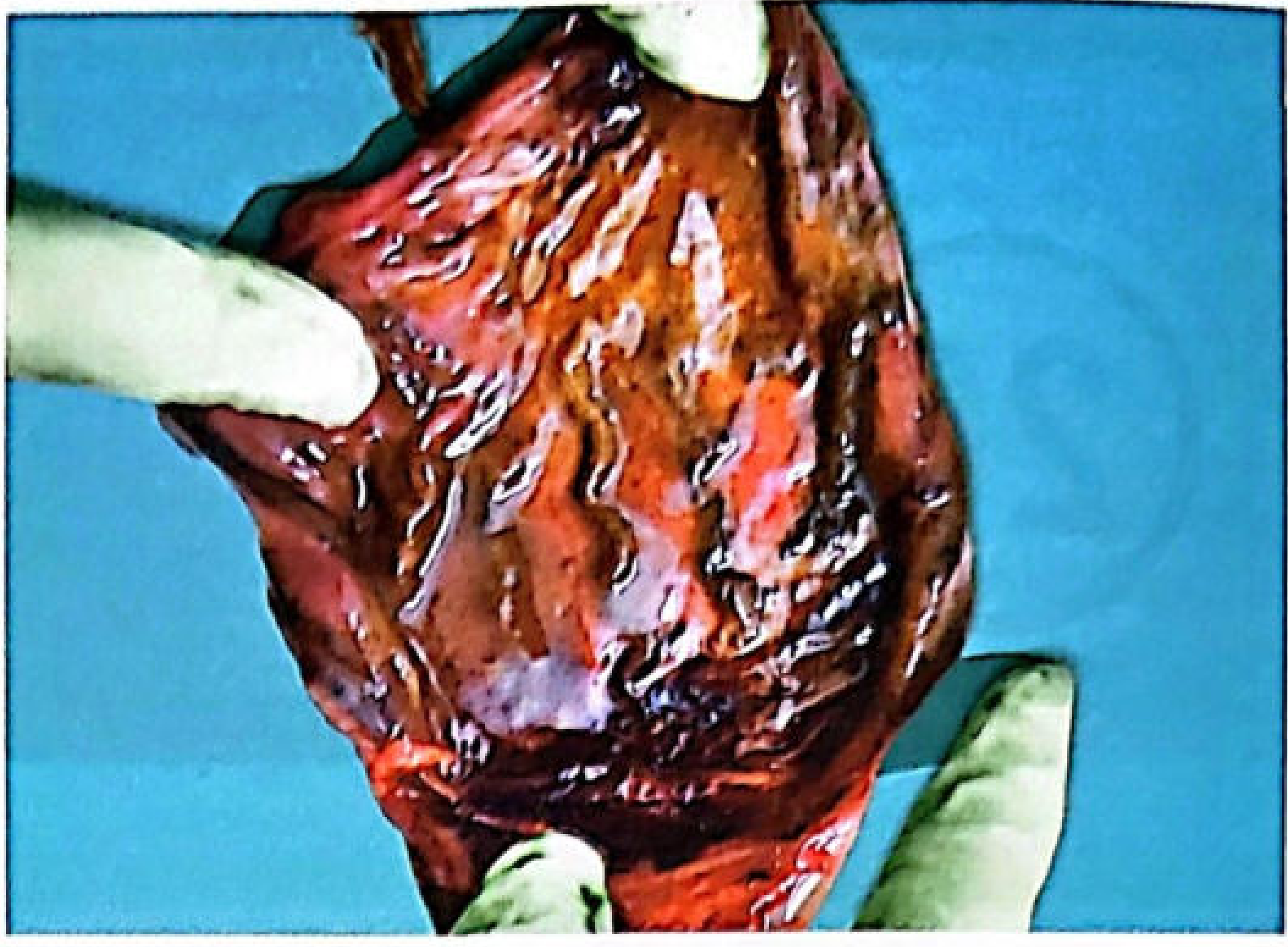
The stomach shows extensive brown-black coagulation necrosis. The mucosal ridges are more damaged than the intervening furrows. The wall may disintegrate when touched.
Internal
| Site | Findings |
|---|---|
| Esophagus | Squamous epithelium relatively resistant; superficial mucosal reaction; corrosion present but perforation is rare |
| Stomach | Main target organ - columnar epithelium affected; superficial erosion + coagulation + eschar; greater part may become a soft, spongy, black mass that disintegrates on touch; acid follows lesser curvature to pylorus → pyloric region most severely affected |
| Stomach contents | Dark brown/black from acid hematin; altered blood; gelatinous; calcium oxalate crystals may be present |
| Peritoneum | Chemical peritonitis + corrosion of organs if perforation occurs |
| Duodenum | Similar but less intense changes |
| Small intestine | Signs of irritation |
| Larynx/Trachea | Corrosion or severe inflammation if acid inhaled |
| Liver/Kidneys | Secondary toxic swelling if patient survives longer; renal tubular necrosis (proximal convoluted tubules primarily) |
| Diaphragm | May show perforation in severe cases |
⚠️ Important: In many cases, little or no free acid is found in viscera at autopsy - because the acid is converted to substances normally present in the body, especially if victim survived 2+ days
Chemical / Forensic Tests
The only suitable material for analysis is the stomach contents
| Test | Result |
|---|---|
| Strong acid + organic matter | Chars organic material |
| Barium nitrate or barium chloride solution added to stomach contents | White precipitate of barium sulphate confirms sulfate/sulfuric acid |
Circumstances of Poisoning
| Mode | Details |
|---|---|
| Suicidal | Most common |
| Accidental | Mistaken for glycerin or castor oil; inhalation in chemical factories |
| Homicidal | Rare - acid taste, immediate action, and obvious physical changes make detection easy |
| Abortifacient | Injected into vagina; also used out of vengeance |
| VITRIOLAGE | Throwing acid on another person (see below) |
Vitriolage (Acid Throwing)
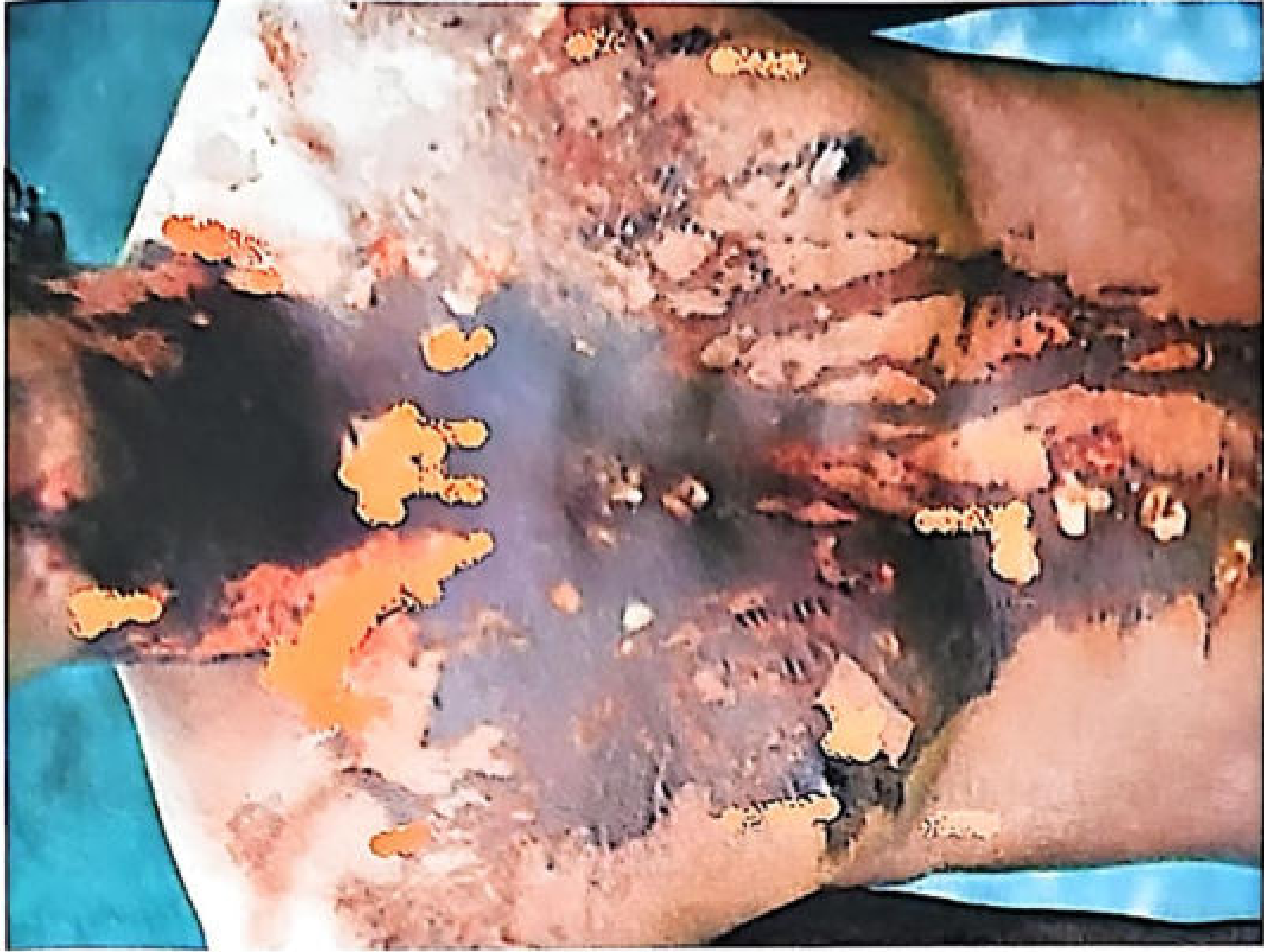
Severe disfiguring acid burns from vitriolage - black necrotic patches with surrounding areas of destruction
- Burns are initially painless (acid destroys nerve endings)
- Penetrating burns - devitalizes tissues, predisposes to infection
- Slow repair; scar tissue causes contracture and disfigurement
- Blindness if eyes involved
- Death from shock or toxemia if extensive body area involved
- Other agents also used: HNO₃, carbolic acid, caustic alkali, juice of marking nut, calotropis
Medicolegal Aspect
- BNS (Bharatiya Nyaya Sanhita) Section 124: Acid attack causing permanent/partial damage = imprisonment of not less than 10 years (may extend to life) + fine payable directly to the victim
Quick Revision - Bullet Points for Exams
- Sulfuric acid = Oil of Vitriol
- Superficial burns in 1 second; full-thickness in 30 seconds
- Mechanism = Coagulation necrosis + hygroscopic dehydration
- Most common presenting symptom = pharyngeal pain
- Teeth = chalky-white; Tongue = swollen, black
- Vomit = brown/black, strongly acid
- Mind remains clear till death
- Fatal dose = 10-15 mL; Fatal period = 12-24 hours
- Stomach most affected (not esophagus) - acid pools at pylorus
- No carbonates/bicarbonates internally - gas + rupture
- No gastric lavage, no emetics
- Postmortem = brown/black leathery eschar; stomach like soft spongy black mass
- Test = Barium sulphate white precipitate with barium nitrate/chloride
- Most cases = suicidal; Vitriolage = throwing acid on others
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026)
Oxalic acid poisoning
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Complete data from three forensic textbooks. Here is the full undergraduate-level account:
Oxalic Acid Poisoning
Basic Information
| Property | Detail |
|---|---|
| Chemical name | Oxalic acid (C₂H₂O₄) |
| Synonyms | Acid of sugar, Salt of sorrel |
| Type | Organic corrosive acid |
| Appearance | Colorless, transparent, prismatic crystals |
| Confusion | Closely resembles magnesium sulphate and zinc sulphate in appearance - common cause of accidental poisoning |
| Natural source | Natural constituent of many plants - spinach, rhubarb, cabbage, sorrel; ~20 mg excreted in urine daily |
Differentiation from Magnesium Sulphate (Important Exam Table)
| Feature | Oxalic Acid | Magnesium Sulphate | Zinc Sulphate |
|---|---|---|---|
| Taste | Sour and acidic | Bitter and nauseating | Bitter and metallic |
| Reaction (pH) | Strongly acidic (<7) | Neutral (7) | Slightly acid |
| On heating | Sublimes (evaporates directly) | Fixed (does not sublime) | Fixed |
| With sodium carbonate | Effervesces but no precipitate | No effervesce; white precipitate | No effervesce; white precipitate |
| Ink/iron stains | Bleaches them | No action | No action |
Memory trick: OA - Oxalic Acid = Sour + Sublimes + Stain-bleacher (3 S's)
Uses (Why It Is Available)
Commercial uses:
- Calico printing
- Cleaning brass, copper articles, wooden surfaces, leather
- Manufacture of straw hats
- Photography
- Bookbinding
Domestic use:
- Common household remedy for removing ink stains and iron marks from clothing
Illegal use:
- Used to erase writing and signatures from paper (document forgery)
Mode of Action - The Three-System Attack
Oxalic acid is unique among corrosive acids - it has BOTH local AND systemic (remote) actions.
1. Local Action (Corrosive)
- Crystals and solutions >10% concentration → corrosive to mucous membranes of GI tract
- Rarely damages skin
- Less than 10% solution → irritant (still causes serious systemic effects after absorption)
- Does NOT lose poisonous properties when diluted (unlike some other poisons)
2. Systemic Action - Hypocalcaemia (KEY FEATURE)
Oxalic acid + Ca²⁺ in blood/tissues → insoluble calcium oxalate
This reaction:
- Removes ionised calcium from circulation → hypocalcaemia
- Calcium oxalate crystals deposit in kidney tubules → tubular necrosis
- Low serum calcium → tetany, convulsions, cardiac arrhythmias
3. Systemic Action - Shock
Large doses cause rapid death from circulatory shock (narcotic effect on cardiovascular system)
Fatal Dose and Period
| Fatal Dose | 15-30 g (smallest recorded: 5 g) |
| Fatal Period | 1-2 hours (longest recorded: 5 days) |
Signs and Symptoms - Three Phases
Phase 1: Fulminating Poisoning (Large dose ≥15 g - death within minutes)
| Symptom | Detail |
|---|---|
| Taste | Burning, sour, bitter taste in mouth |
| Throat | Sense of constriction around throat |
| Pain | Burning pain mouth → stomach; starts epigastric → radiates all over abdomen; tenderness |
| Vomiting | Nausea, eructations → persistent vomiting; vomit = "coffee-ground" (altered blood + mucus) |
| Thirst | May be present |
| Bowels | Usually unaffected (death too fast); if life prolonged → diarrhoea |
| Death | Before bowels are affected - within minutes |
Phase 2: Acute Poisoning (Large dose - patient survives hours)
Dominated by hypocalcaemia symptoms:
| Symptom | Mechanism |
|---|---|
| Muscle irritability and tenderness | Low Ca²⁺ increases neuromuscular excitability |
| Tetany → Convulsions | Severe hypocalcaemia → seizures |
| Numbness and tingling of fingertips and legs | Peripheral nerve irritability |
| Cardiovascular collapse | Low Ca²⁺ → cardiac dysfunction |
| Stupor and coma | In some cases |
Phase 3: Delayed Poisoning (Death in 2-14 days from renal failure)
Symptoms of uraemia:
- Scanty or suppressed urine (oliguria/anuria)
- Urine contains: blood, albumin, calcium oxalate crystals
- Oxaluria = calcium oxalate crystals in urine (envelope-shaped under microscope)
- Metabolic acidosis
- Ventricular fibrillation
Treatment
Step 1 - Gastric Lavage
- Since corrosion is less severe than mineral acids, a soft stomach tube can be passed with care
- Lavage performed using calcium lactate or gluconate (2 teaspoonfuls in each lavage aliquot)
- Do NOT use warm water - warm water dissolves more acid and increases absorption
Step 2 - Antidote: CALCIUM (any preparation)
Calcium + oxalate → insoluble calcium oxalate → harmless, cannot be absorbed
Options:
- Chalk (calcium carbonate) suspension - 30 g chalk in water or milk neutralizes ~20 g oxalic acid (most readily available)
- Lime water
- Calcium lactate
- Calcium gluconate (oral)
- Calcium gluconate 10%, 10 mL IV at regular intervals (for systemic hypocalcaemia)
⚠️ Do NOT give alkalis (soda/potash/ammonia) - their oxalates are soluble and increase absorption
Step 3 - Severe Hypocalcaemia
- Parathyroid extract 100 units IM in severe cases
Step 4 - Renal Monitoring
- Check urinary output to detect renal damage
- Control fluid intake accordingly
Step 5 - Other Measures
- Demulcent drinks
- Bowels may be evacuated by enema or castor oil
- Dialysis or exchange transfusion for renal failure
- Symptomatic treatment
Postmortem Appearances
External
- Skin is rarely burned (unlike mineral acids)
- No staining of lips/chin (important difference from sulfuric/nitric acid)
Internal - Mouth and Oesophagus
- Mucous membrane of tongue, mouth, throat, oesophagus: white, as if bleached (sometimes reddened by irritation)
- Oesophagus shows corrugated surface with longitudinal erosion
Internal - Stomach
- Outer coat: inflamed and reddened; patchy softening
- Stomach contents: brownish, gelatinous (due to acid haematin formation)
- Mucous membrane: corroded and detached in degrees depending on concentration
- Blood vessels in submucous layer visible as dark lines (due to acid haematin)
- Perforation is rare
- If death is immediate: stomach may be pale and not corroded
- If whole stomach affected: corroded and perforated in severe cases
Internal - Kidneys (Pathognomonic Feature)
Kidneys: swollen, congested; renal tubules filled with calcium oxalate crystals Tubular necrosis primarily in proximal convoluted tubules
- Calcium oxalate crystals: envelope-shaped under microscope
Internal - If Only Narcotic Effect (No Local Damage)
- Congestion of lungs, liver, kidneys, brain - without any local GI changes
If Death Delayed
- Inflammation of upper small intestine
- Kidney changes (oxaluria, tubular necrosis)
Chemical Test
| Test | Result |
|---|---|
| Add barium nitrate solution to suspected material | White precipitate of barium oxalate (soluble in HCl or HNO₃ - distinguishes from barium sulphate which is insoluble) |
| Urine with 10% ferric chloride | Not applicable (ferric chloride is for phenol) |
| Strong acid chars organic matter | Not applicable to oxalic acid (sublimes) |
Material for analysis: Stomach contents
Medicolegal Aspects
| Mode | Details |
|---|---|
| Accidental | Most common - frequently mistaken for magnesium sulphate or sodium bicarbonate (similar crystal appearance). Also: rhubarb leaves used as vegetables |
| Suicidal | Occasionally - sour taste limits willingness |
| Homicidal | Very rare - sour/bitter taste is detectable; rapid action makes it obvious |
| Abortifacient | Rarely used |
| Forgery | Used to erase writing and signatures from paper |
| Special note | Oxalic acid solutions poured on head cause falling off of hair |
Summary Comparison - Oxalic Acid vs Other Acids
| Feature | Sulfuric Acid | Oxalic Acid |
|---|---|---|
| Type | Inorganic/mineral | Organic |
| Necrosis | Coagulation (hard, leathery) | Coagulation (softer, bleached) |
| Skin burns | Yes - prominent | Rare |
| Lip/chin staining | Yes - brown/black | No staining |
| Main systemic toxicity | Shock, renal failure | Hypocalcaemia → tetany/convulsions + renal failure |
| Gastric lavage | Contraindicated | Allowed with care (soft tube + calcium solution) |
| Antidote | None specific (demulcents) | Calcium (precipitates oxalate) |
| Crystal deposits | None | Calcium oxalate crystals in kidney (envelope-shaped) |
| Fatal period | 12-24 hours | 1-2 hours (faster) |
| Postmortem stomach | Black, leathery, soft spongy mass | Brownish gelatinous; white bleached mucosa |
| Confusion with | - | Magnesium sulphate (appearance) |
Memory Tricks
| Trick | Content |
|---|---|
| "OA = Oxalate grabs cAlcium" | Oxalic Acid → Hypocalcaemia |
| "Tetany, Twitching, Tingling = Think Oxalic" | 3 T's of hypocalcaemia |
| "Coffee-ground vomit + Convulsions" | Unique combination pointing to oxalic acid |
| "Antidote = Chalk/Calcium - makes insoluble crystals" | Calcium precipitates oxalate |
| "No soda/alkali - their oxalates are SOLUBLE" | Avoid NaOH/NaHCO₃ as antidote |
| "Envelope crystals in kidney" | Calcium oxalate on microscopy |
| "Sublimes on heating - not magnesium sulphate" | Distinguishing test |
| "No lip staining" | Unlike H₂SO₄ and HNO₃ |
Sources: The Essentials of Forensic Medicine and Toxicology 36th Ed (2026); Parikh's Textbook of Medical Jurisprudence; P.C. Dikshit Textbook of Forensic Medicine and Toxicology
This is a shared conversation. Sign in to Orris to start your own chat.