Hey orris what is modified johnsons criteria And what are he grading for adhesions
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Searching the Web
grading of adhesions classification score surgery
Finding Sources
Searching the Web
Zuhlke adhesion classification grading Grade 1 2 3 4 surgery
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC8057995
Searching the Web
Zuhlke adhesion grading filmy vascular grade 1 2 3 4 classification table
Reading Web Page
https://www.sumroc.org.tw/upload/journal/1/20230620/10%20Adh…
Loading Image
I now have everything needed for a complete answer on both topics.
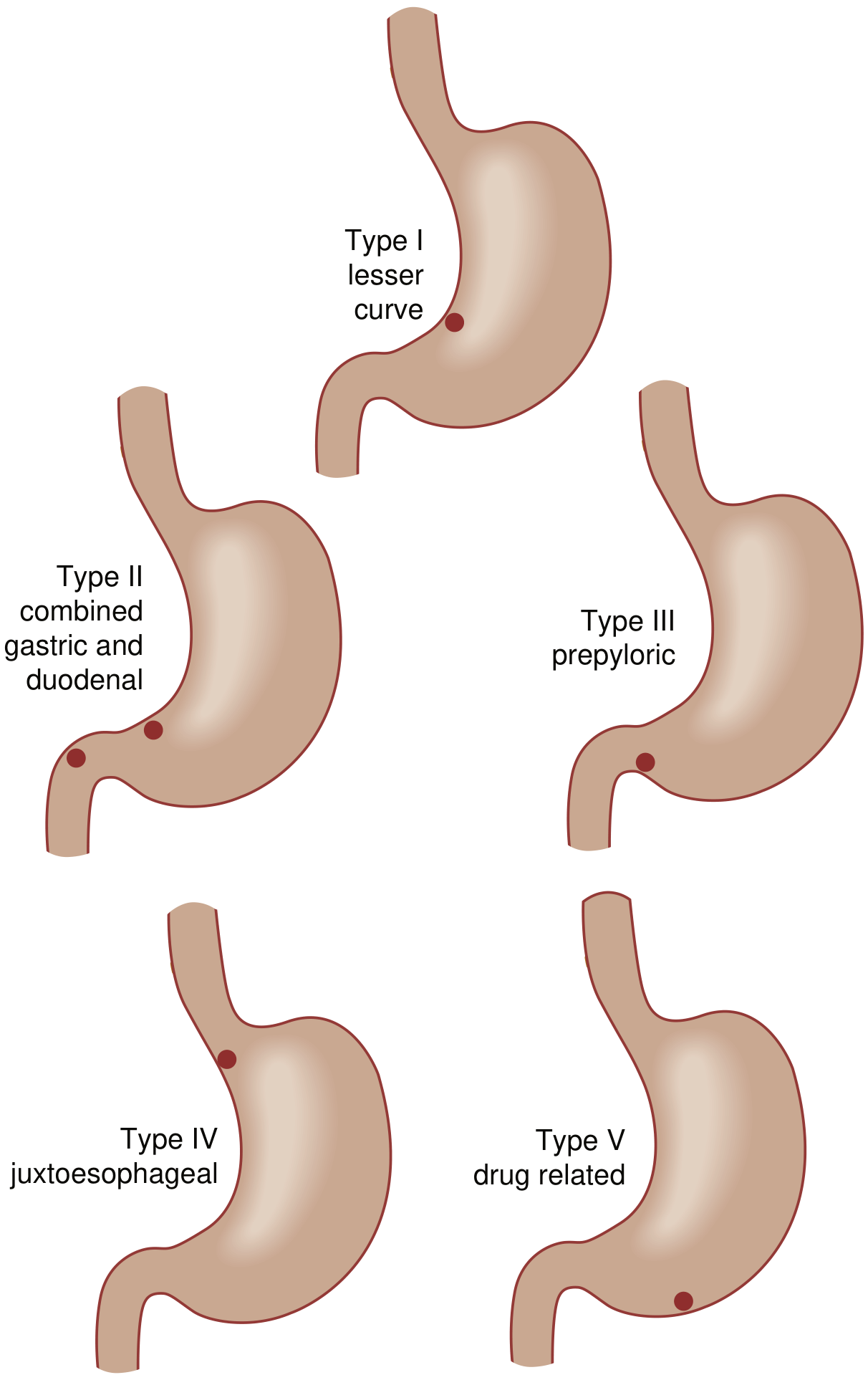
1. Modified Johnson Classification (Gastric Ulcers)
The original Johnson classification (1965) described 3 types of gastric ulcer based on anatomical location and acid secretion status. Two additional types were later added, creating the Modified Johnson Classification (5 types total):
| Type | Location | Acid Hypersecretion | Notes |
|---|---|---|---|
| I | Lesser curvature at/near angularis incisura | No | Most common benign gastric ulcer; NOT associated with H. pylori acid excess |
| II | Body of stomach/incisura + concomitant duodenal ulcer (active or healed) | Yes | Resembles duodenal ulcer pathophysiology |
| III | Prepyloric region | Yes | Also resembles duodenal ulcer; vagotomy included in surgical management |
| IV | High on lesser curvature, near the gastroesophageal junction | No | May require Csendes (Roux-en-Y) reconstruction; excision can encroach on esophagus |
| V | Anywhere in the stomach (medication/NSAID-induced) | No | Drug-related; amenable to simple wedge resection |
Key surgical implications:
-
Types I, IV, V - vagotomy NOT needed (no acid hypersecretion)
-
Types II and III - truncal vagotomy included in surgical treatment (acid-driven)
-
Type IV - Csendes or Pauchet procedure if excision encroaches on the cardia
-
Type V - simple wedge resection or patch/oversew with biopsy in unstable patients
-
Current Surgical Therapy, 14th ed., Table 1; Sabiston Textbook of Surgery, Table 86.3
2. Grading of Adhesions
The most widely used classification in general surgery is the Zuhlke (Zühlke) Classification (1990), which grades adhesions by their morphological characteristics at the time of surgery:
| Grade | Description | Ease of Separation |
|---|---|---|
| Grade 1 (Class I) | Filmy adhesions; no vascularization | Easy - blunt dissection, minimal/no bleeding |
| Grade 2 (Class II) | Stronger adhesions; some vascularization | Possible with blunt dissection but requires effort |
| Grade 3 (Class III) | Dense, vascular adhesions | Requires sharp dissection; risk of damage to underlying organ |
| Grade 4 (Class IV / severe) | Very dense, vascular, organ-to-organ adhesions; organs adherent to abdominal wall | Dissection highly difficult; high risk of inadvertent enterotomy |
Clinical significance: Enterotomy rates increase steeply with grade - 0% at grade 1, ~0.7% at grade 2, ~9% at grade 3, and up to 36% at grade 4. This is why adhesion grading is recorded peroperatively.
Other Adhesion Scoring Systems
Beyond Zuhlke, several context-specific systems are used:
- AFS (American Fertility Society) Score - used in gynecologic/pelvic surgery; scores adhesions by location, extent (< 1/3, 1/3-2/3, >2/3), and type (filmy vs. dense) at multiple pelvic sites (ovary, tube, etc.)
- Nair Score / Davey Score - used to predict pelvic adhesions before repeat caesarean section, correlating striae gravidarum with intraoperative adhesion severity
- CLAS (Clinical Adhesion Score) - a newer system that measures the clinical morbidity of adhesions (bowel obstruction, pain, infertility, difficulty at reoperation) rather than morphological appearance alone
Note: Zuhlke's classification is the standard for general/GI surgery. AFS scoring is standard in gynecology. Neither has been fully validated against long-term patient outcomes, which is why the CLAS was developed.
What are the surgical treatment options for gastric ulcer by type?
Finding Sources
Reading File
Reading File
Reading File
I have everything needed for a thorough answer.
Surgical Treatment Options for Gastric Ulcer by Type
Operations for gastric ulcer fall into two fundamental categories: (1) those that excise the ulcer and (2) those that leave the ulcer in situ but biopsy it (to exclude cancer). In unstable patients, formal resection is avoided.
Quick Rule Before Operating
- Always assess whether the ulcer involves the pancreas, portal triad, or celiac artery before resection
- If the ulcer is NOT excised, biopsy is mandatory to rule out malignancy
- Add vagotomy for types II and III (acid-driven); it is unnecessary for types I, IV, and V
Treatment by Ulcer Type
| Type | Option 1 - Resect Ulcer | Option 2 - Biopsy Ulcer (leave in situ) | Vagotomy? |
|---|---|---|---|
| I (lesser curve, incisura) | Distal gastrectomy (~50%) | Vagotomy + drainage ± wedge excision | No |
| II (body + duodenal ulcer) | Distal gastrectomy + vagotomy | Vagotomy + drainage | Yes |
| III (prepyloric) | Distal gastrectomy + vagotomy | Vagotomy + drainage | Yes |
| IV (near GEJ) | Csendes or Pauchet procedure | Kelling-Madlener procedure, or vagotomy + drainage | No |
| V (drug-induced, anywhere) | Wedge resection | Patch/oversew | No |
Unstable patients (any type): Simple patch or oversew with biopsy is the preferred option across all types.
Type-by-Type Detail
Type I (lesser curve at incisura)
- Distal gastrectomy (about 50%, to include the ulcer) without vagotomy is the standard
- Reconstruction: Billroth I (gastroduodenostomy) or Billroth II (gastrojejunostomy) to the greater curvature side of the remnant
- Wedge excision alone is technically difficult here and not preferred
Type II (body + duodenal ulcer)
- Distal gastrectomy + truncal vagotomy (pathophysiology resembles duodenal ulcer - acid hypersecretion)
- Billroth II reconstruction is often preferred given the concomitant duodenal disease
- Vagotomy + gastrojejunostomy with ulcer biopsy is an acceptable alternative in higher-risk patients
Type III (prepyloric)
- Distal gastrectomy + truncal vagotomy (same rationale as Type II)
- Vagotomy + drainage with biopsy is the alternative
Type IV (high lesser curvature, near GEJ)
- Csendes procedure (distal subtotal gastrectomy with in-continuity excision of the high lesser curvature ulcer + Roux-en-Y esophagogastrojejunostomy) - used when resection encroaches on the gastric cardia
- Pauchet procedure (distal gastric resection + lesser curvature extension + Billroth II or Roux reconstruction) - for type 4 ulcers that are more distally located or type 1 ulcers that are unusually proximal
- Kelling-Madlener procedure (distal gastrectomy without ulcer excision + ulcer biopsy) - for when the high ulcer cannot safely be resected
- No vagotomy needed
Type V (NSAID/drug-induced, any location)
- Simple wedge resection is ideal - these tend to be on the greater curvature and are amenable to it
- Patch/oversew with biopsy for unstable patients
- No vagotomy needed
- Remove the offending drug postoperatively
Reconstruction Options After Distal Gastrectomy
| Reconstruction | When Preferred |
|---|---|
| Billroth I (gastroduodenostomy) | Simpler; preferred when duodenum is healthy |
| Billroth II (gastrojejunostomy) | Preferred with concomitant duodenal disease (Type II); higher marginal ulcer risk - consider adding vagotomy |
| Roux-en-Y | Preferred with small gastric remnant or when anastomosis is close to the GEJ (Type IV); avoids biliopancreatic reflux |
Special Indications
Perforation (most common indication for surgery):
- Stable patients: distal gastrectomy ± vagotomy based on type
- Unstable patients: simple patch/oversew + biopsy, treat H. pylori postoperatively
Bleeding:
- Stable: definitive resection ± vagotomy by type
- Unstable: ulcer oversew or wedge ± vagotomy + drainage
Obstruction:
- Classic operation: vagotomy + distal gastrectomy
- Alternative: vagotomy + gastrojejunostomy (lower operative mortality, preferred in high-risk patients)
Nonhealing (intractability):
-
Distal gastrectomy (classic) ± vagotomy for types II and III
-
In thin/frail patients: wedge resection + highly selective vagotomy (HSV) is an option
-
Current Surgical Therapy, 14th ed., Table 2; Schwartz's Principles of Surgery, 11th ed.; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.