heart blood supply
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive information with excellent diagrams. Let me compile the full answer.
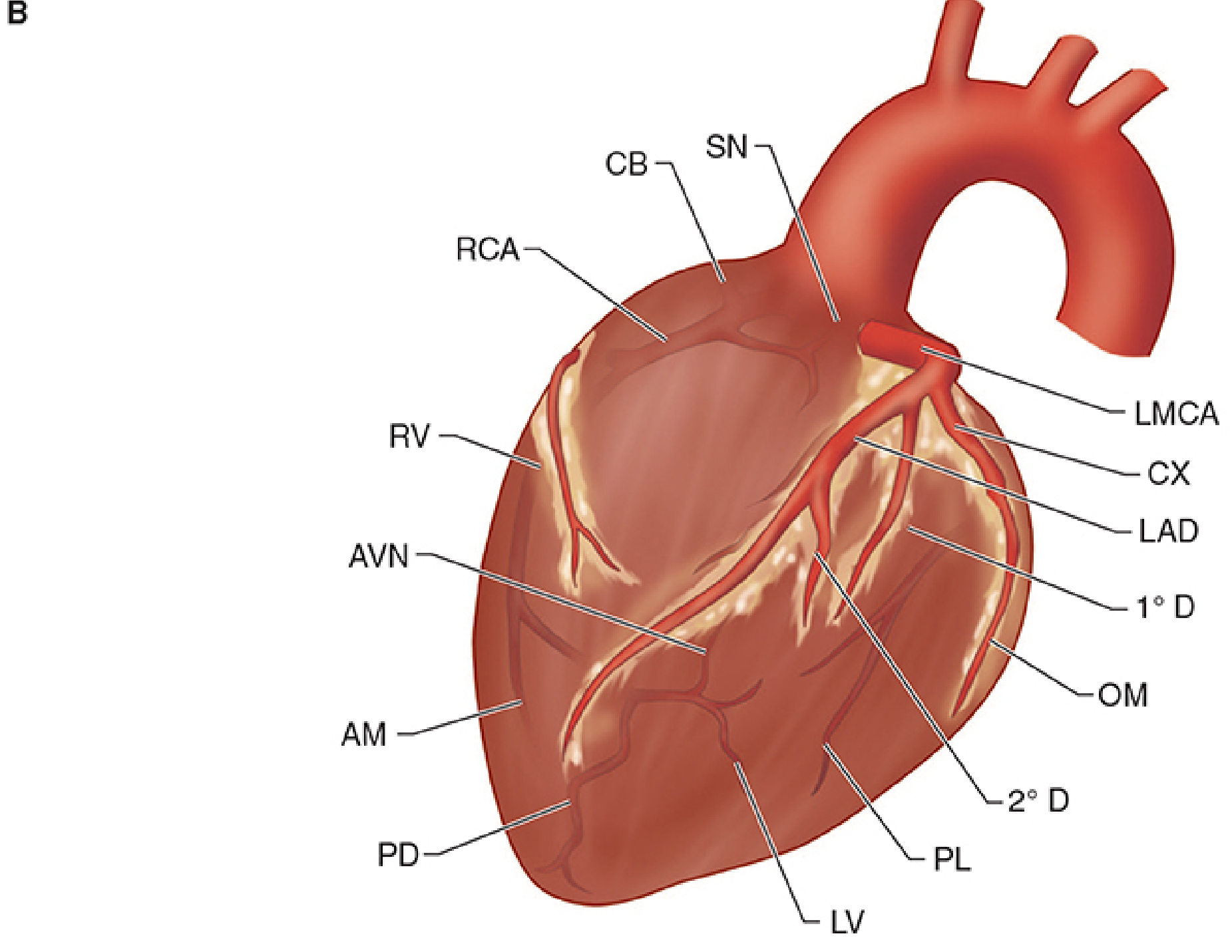
Blood Supply of the Heart (Coronary Circulation)
The heart receives its entire arterial supply from two coronary arteries - the right coronary artery (RCA) and the left coronary artery (LCA) - which arise from the right and left aortic sinuses, respectively. Blood flows from epicardial to endocardial vessels during diastole.
Arterial Supply
Origins
The coronary ostia open into the right and left aortic sinuses. As blood recoils after ventricular contraction and fills the aortic sinuses, it is automatically forced into the coronary arteries. The posterior (non-coronary) aortic sinus does not give off a coronary artery.
- Gray's Anatomy for Students
Right Coronary Artery (RCA)
The RCA arises from the right aortic sinus, passes behind the pulmonary trunk, and follows the right atrioventricular (A-V) sulcus.
Branches and territories:
- SA nodal artery - supplies the sinoatrial node in 60% of individuals
- Conus branch - supplies the right ventricular outflow tract
- Atrial branches - right atrium
- Right ventricular branches - anterior surface of right ventricle
- Acute (right) marginal branch - right border of heart; supplies remaining anterior surface of right ventricle and posterior third of the interventricular septum
- AV nodal artery - supplies the AV node in 85-90% of individuals
- Posterior descending artery (PDA) - runs down the posterior interventricular groove; supplies the superior-posterior interventricular septum and inferior wall of the left ventricle
In 85% of people, the RCA gives rise to the PDA - this is called right dominant circulation. In the remaining 15%, the PDA comes from the left coronary system (left dominant circulation).
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- P.C. Dikshit Textbook of Forensic Medicine
Left Coronary Artery (LCA)
The LCA (left main coronary artery, LMCA) arises from the left aortic sinus. After a short course of ~1 cm, it bifurcates into two major branches:
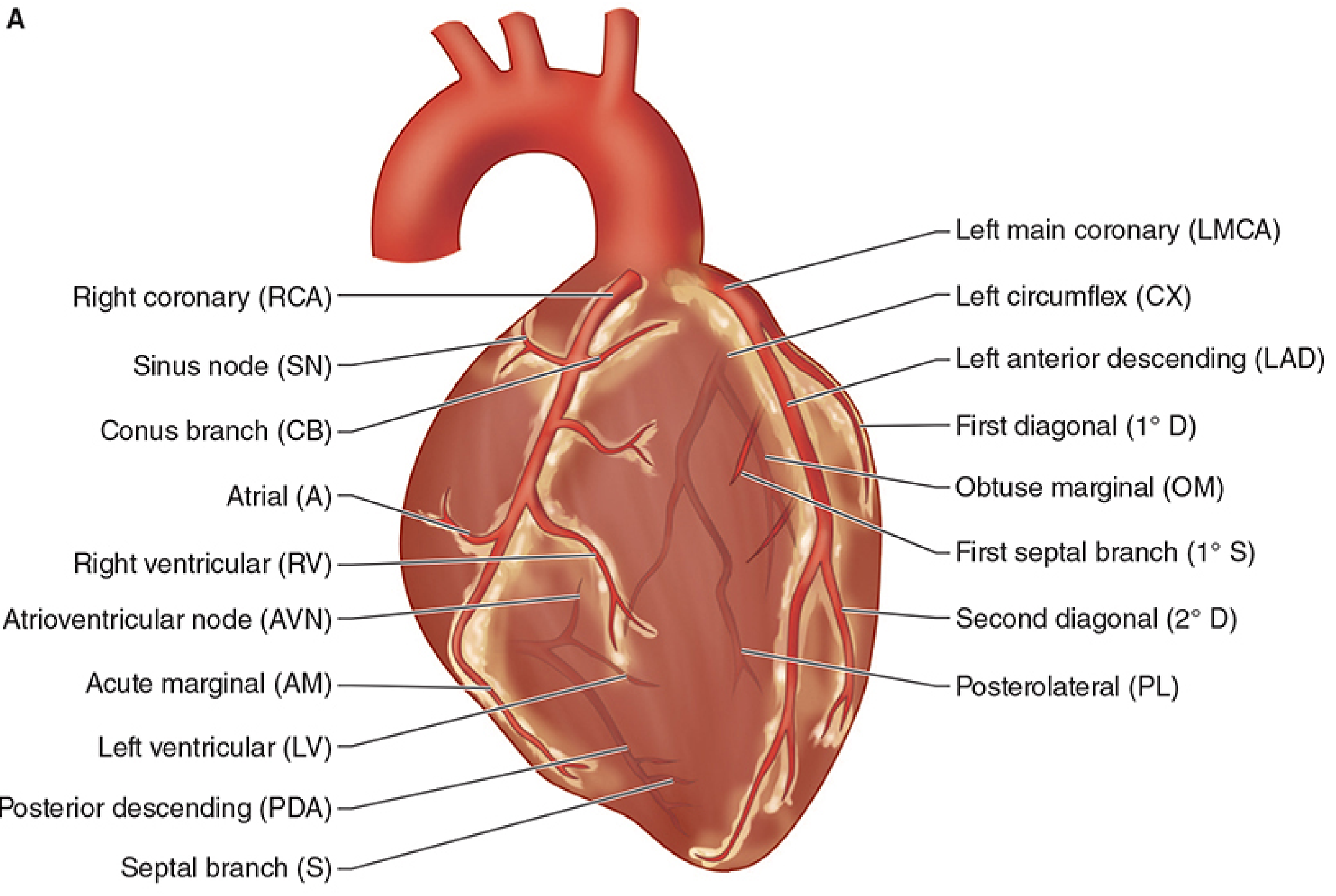
1. Left Anterior Descending Artery (LAD)
- Courses down the anterior interventricular sulcus to reach the apex
- Supplies:
- Anterior aspects of both right and left ventricles
- Anterior 2/3rds of the interventricular septum
- Apex of the heart
- Key branches: septal perforators, diagonal branches (supply anterolateral LV wall)
- Also called the "widow maker" due to the extensive territory it supplies
2. Left Circumflex Artery (CX)
-
Follows the left atrioventricular sulcus to the back of the heart
-
Supplies: left atrium, lateral wall of left ventricle
-
Key branch: obtuse marginal (OM) branch
-
In a left dominant circulation, the CX wraps around the AV groove and continues as the PDA, supplying most of the posterior septum and inferior wall
-
Morgan and Mikhail's Clinical Anesthesiology, 7e
-
P.C. Dikshit Textbook of Forensic Medicine
Summary Table: Coronary Territories
| Region | Primary Supply |
|---|---|
| Right atrium | RCA |
| Right ventricle (most) | RCA |
| Left atrium | LCA (CX) |
| Left ventricle - anterior wall | LAD |
| Left ventricle - lateral wall | CX |
| Left ventricle - inferior wall | RCA (PDA) in right dominant |
| Interventricular septum (anterior 2/3) | LAD |
| Interventricular septum (posterior 1/3) | PDA (usually RCA) |
| SA node | RCA (60%), LAD (40%) |
| AV node | RCA (85-90%), CX (10-15%) |
| Bundle of His | Dual - PDA + LAD |
| Anterior papillary muscle (mitral) | Dual - LAD diagonal + CX marginal |
| Posterior papillary muscle (mitral) | PDA only (vulnerable to ischemia) |
Venous Drainage
Blood returns to the right atrium via three routes:
- Coronary sinus (main route) - receives the great, middle, small, and posterior cardiac veins; drains into the right atrium
- Anterior cardiac veins - arise on the anterior surface of the right ventricle; cross the coronary sulcus and drain directly into the right atrium
- Thebesian veins - small veins that drain directly into the heart chambers
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Gray's Anatomy for Students
Coronary Perfusion Physiology
Key principle: Coronary perfusion is intermittent, not continuous.
- Left ventricle is perfused almost entirely during diastole - during systole, intramyocardial pressures approach systemic arterial pressure and nearly occlude the intramyocardial coronary vessels
- Right ventricle is perfused during both systole and diastole
Left coronary perfusion pressure = Arterial diastolic pressure - LVEDP
Normal coronary blood flow at rest: ~250 mL/min in an adult male.
The myocardium autoregulates blood flow between perfusion pressures of ~50-120 mmHg. The primary regulator is metabolic demand (adenosine is the key vasodilatory metabolite). Increased heart rate decreases perfusion because it disproportionately shortens diastolic time.
The endocardium is most vulnerable to ischemia because it is subjected to the greatest intramural pressures during systole.
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Coronary Artery Disease: Common Sites of Stenosis
From forensic/pathology data, fatal coronary stenosis most commonly affects:
- Anterior interventricular (LAD) - 45-64% of cases
- Right main coronary - 24-46%
- Left circumflex - 3-10%
- Left main coronary - 0-10%
- Right marginal and posterior interventricular branches - relatively immune
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
This is a shared conversation. Sign in to Orris to start your own chat.