Ckd
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"chronic kidney disease"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to deliver a thorough CKD clinical review. Let me compile it all.
Chronic Kidney Disease (CKD) - Full Clinical Review
Definition
CKD is defined as kidney damage or decreased kidney function lasting 3 months or more, regardless of cause. The key markers are:
-
GFR < 60 mL/min/1.73 m² (stages G3-G5), OR
-
Markers of kidney damage (proteinuria, hematuria, imaging abnormalities, pathologic lesions) present for ≥3 months even with normal GFR (stages G1-G2)
-
Harrison's Principles of Internal Medicine 22E (2025)
Staging - CGA Classification (KDIGO)
CKD is classified by Cause (C), GFR category (G), and Albuminuria (A) - the "CGA" system.
GFR Categories (G Staging)
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high (+ kidney damage marker) | ≥90 |
| G2 | Mildly decreased (+ kidney damage marker) | 60-89 |
| G3a | Mildly to moderately decreased | 45-59 |
| G3b | Moderately to severely decreased | 30-44 |
| G4 | Severely decreased | 15-29 |
| G5 | Kidney failure (ESKD) | <15 |
Albuminuria Categories (A Staging) - Urine Albumin:Creatinine Ratio
| Category | Label | ACR |
|---|---|---|
| A1 | Normal to mildly increased | <30 mg/g |
| A2 | Moderately increased | 30-300 mg/g |
| A3 | Severely increased | >300 mg/g |
Prognosis is determined by combining G and A staging - higher stages in both confer much greater risk of all-cause mortality, cardiovascular mortality, and CKD progression.
- Washington Manual of Medical Therapeutics; Brenner and Rector's The Kidney
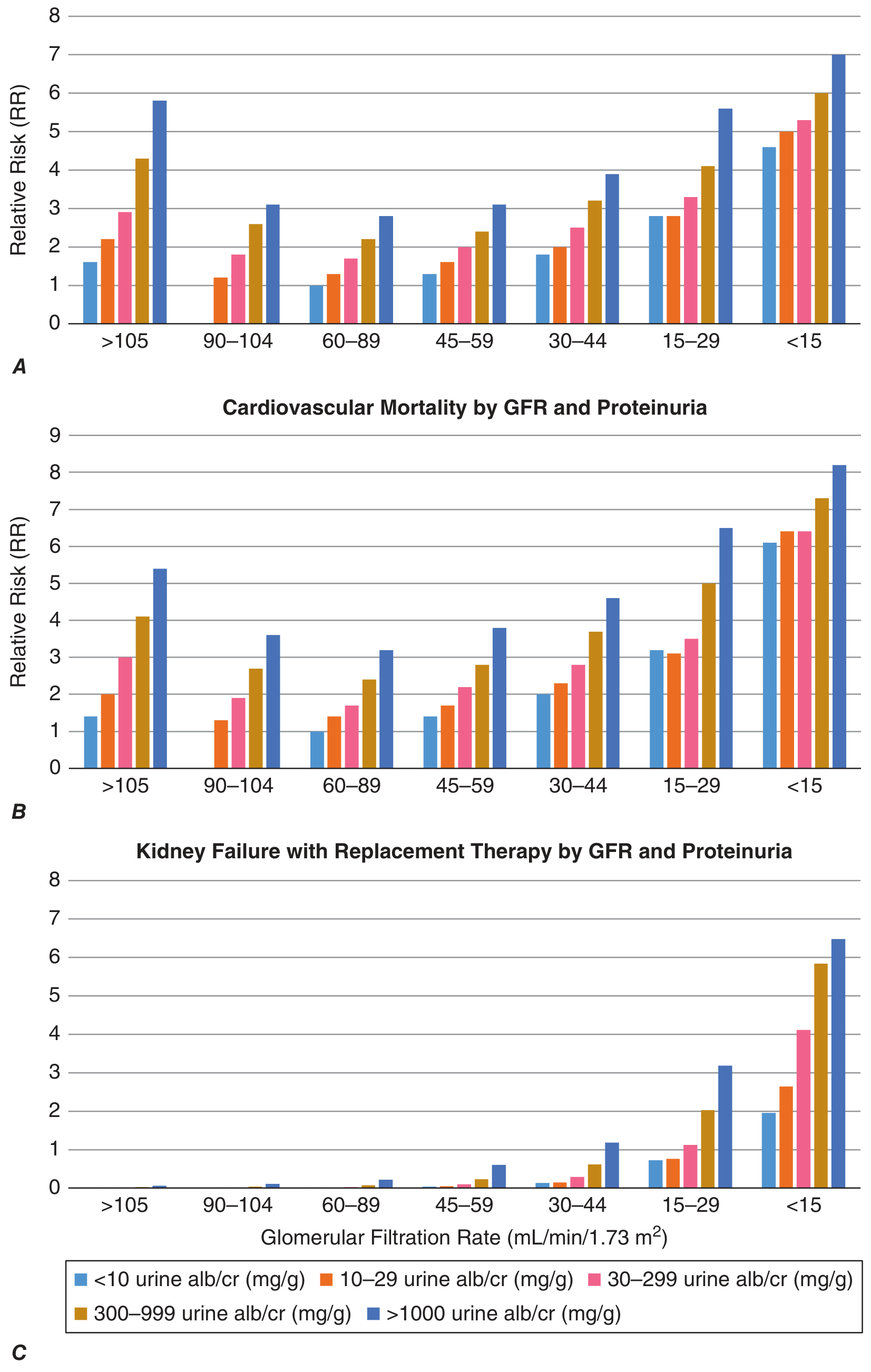
KDIGO Risk Chart - Relative Risk by GFR and Albuminuria
The chart below (from Harrison's 22e) shows how declining GFR combined with increasing albuminuria multiplicatively raises relative risk for cardiovascular death, all-cause mortality, and kidney failure requiring replacement therapy:
Pathophysiology
Two broad mechanisms drive CKD:
-
Initiating injury-specific mechanisms - immune complex deposition, inflammation, genetic defects, metabolic injury, microvascular disease, or toxin exposure affecting glomerular, vascular, or tubulointerstitial compartments.
-
Common final pathway - hyperfiltration/hypertrophy: After nephron mass is reduced (from any cause), surviving nephrons undergo compensatory hyperfiltration driven by vasoactive hormones, cytokines, and growth factors. Initially this preserves GFR, but increased intraglomerular pressure and flow distorts glomerular architecture, impairs podocyte function, and disrupts the filtration barrier - leading to progressive glomerulosclerosis and nephron dropout. Intrarenal RAS activation and reduced tubuloglomerular feedback both contribute to this maladaptive hypertrophy and sclerosis.
This explains why a reduction in nephron number from an initial insult can cause progressive GFR decline over many years, irrespective of whether the original disease is still active.
- Harrison's Principles of Internal Medicine 22E (2025)
Causes / Etiology
| Category | Examples |
|---|---|
| Diabetic nephropathy | Most common cause of CKD and ESKD globally |
| Hypertensive nephrosclerosis | Second most common |
| Glomerular diseases | IgA nephropathy, focal segmental glomerulosclerosis, membranous nephropathy |
| Polycystic kidney disease | ADPKD (most common monogenic kidney disease) |
| Tubulointerstitial disease | Reflux nephropathy, analgesic nephropathy, myeloma kidney |
| Renovascular disease | Renal artery stenosis, atheroembolism |
| Hereditary/genetic | APOL1 variants (sub-Saharan African ancestry; G1/G1, G2/G2, G1/G2 confer 7.5% lifetime risk of ESKD), Alport syndrome |
| Congenital | Multicystic kidney, cystic renal dysplasia, juvenile nephronophthisis |
| Recurrent AKI | Incomplete recovery leads to new-onset or progressive CKD |
Genetic risk factors may account for up to 20% of adult-onset CKD. Modifiable risk factors include diabetes, hypertension, obesity, smoking, NSAIDs, and prior AKI.
- Harrison's 22E; Campbell-Walsh-Wein Urology; Washington Manual
Symptoms and Clinical Presentation
Patients are typically asymptomatic until late G4-G5. Complications begin appearing at G3:
- Early (G1-G2): Usually none; detected incidentally on labs or screening
- G3: Hypertension, mild anemia, early mineral-bone disorder, fatigue
- G4-G5 (uremic syndrome):
- Nausea, vomiting, anorexia, metallic taste
- Pruritus (uremic pruritus)
- Encephalopathy, asterixis, seizures (severe uremia)
- Pericarditis (uremic)
- Volume overload, edema, dyspnea
- Bleeding tendency (platelet dysfunction)
Complications
1. Hypertension
- Almost universal in CKD; caused by sodium and water retention, RAS activation, sympathetic overactivation
- Leads to further nephron damage (hyperfiltration) and is a major cardiovascular risk factor
2. Anemia
- Normochromic normocytic anemia due to reduced erythropoietin (EPO) production by diseased kidneys
- Worsened by iron deficiency, chronic inflammation, shortened RBC survival
- Management: correct iron deficiency first, then erythropoiesis-stimulating agents (ESAs) if needed
3. Metabolic Acidosis
- Common in CKD; usually mild and compensated by chronic hyperventilation
- Due to impaired NH₄⁺ excretion and reduced HCO₃⁻ regeneration
- Accelerates muscle catabolism, bone disease, and CKD progression
4. Hyperkalemia
- Most serious electrolyte disturbance in CKD
- Mechanisms: reduced renal K⁺ excretion, metabolic acidosis (shifts K⁺ extracellularly), ACE inhibitor/ARB use
- Risk greatest in G4-G5 and with RAAS blockade
5. CKD-Mineral Bone Disorder (CKD-MBD) / Renal Osteodystrophy
- Begins at G3; includes secondary hyperparathyroidism, hyperphosphatemia, hypocalcemia, vitamin D deficiency, elevated FGF-23
- Bone diseases include high-turnover (osteitis fibrosa from 2° hyperparathyroidism) and low-turnover (adynamic bone disease, osteomalacia)
- Increased vascular calcification contributes to cardiovascular mortality
6. Cardiovascular Disease
- Leading cause of death in CKD patients
- Risk increases multiplicatively with lower GFR and higher albuminuria (see chart above)
- Mechanisms: hypertension, dyslipidemia, anemia, inflammation, volume overload, uremic toxins
7. Hyperuricemia
- Common in CKD; associated with CKD progression and cardiovascular risk
- Xanthine oxidase inhibitors (allopurinol, febuxostat) may help in some patients
8. Dyslipidemia
- Elevated triglycerides, reduced HDL; increased cardiovascular risk
9. Malnutrition / Protein-Energy Wasting (PEW)
-
Progressive in advanced CKD due to anorexia, metabolic acidosis, inflammation
-
Miller's Anesthesia 10e; Washington Manual; National Kidney Foundation Primer 8e
Diagnosis and Monitoring
- eGFR using CKD-EPI equation (preferred over MDRD in most guidelines); Cockcroft-Gault for drug dosing
- Urine ACR (albumin:creatinine ratio) on spot urine - defines albuminuria category
- Serum creatinine, BUN, electrolytes, bicarbonate, phosphate, calcium, PTH
- CBC for anemia assessment
- Urinalysis + microscopy - RBC casts (glomerulonephritis), granular casts (ATN), lipid casts (nephrotic)
- Renal ultrasound - assess size (small bilateral = chronic), echogenicity, obstruction, cysts
- 24-hour urine for proteinuria quantification if needed
- Kidney biopsy when cause is unclear and diagnosis will change management
Management
General Approach
Treatment focuses on: (1) slowing CKD progression, (2) managing complications, (3) cardiovascular risk reduction, (4) preparation for renal replacement therapy (RRT)
1. Blood Pressure Control
- Target: <130/80 mmHg (SPRINT data supports this in non-diabetic CKD patients at high CV risk)
- First-line: ACE inhibitors or ARBs - reduce systemic and intraglomerular pressure, decrease albuminuria; proven to slow CKD progression, especially with proteinuria
- Do NOT combine ACE inhibitor + ARB (dual RAAS blockade - increases hyperkalemia and AKI risk)
- Usually requires 2-4 antihypertensive agents including a diuretic
- Monitor for hyperkalemia and acute eGFR drop (acceptable up to 30% with RAAS initiation)
2. SGLT2 Inhibitors (Major Recent Advance)
- Originally developed for diabetes, now proven to slow CKD progression in both diabetic and non-diabetic CKD
- Mechanisms: reduce intraglomerular hyperfiltration (tubuloglomerular feedback restoration), lower albuminuria, blood pressure, and body weight; possible direct anti-fibrotic and anti-inflammatory effects
- CREDENCE trial (canagliflozin): 30% reduction in composite of ESKD, doubling of serum creatinine, and renal/CV death; 32% reduction in ESKD (eGFR 30-89 with albuminuria despite max RAAS therapy)
- DAPA-CKD (dapagliflozin): benefit in both diabetic and non-diabetic CKD
- Currently indicated in diabetes + CKD (eGFR ≥30 for some agents); trials expanding to non-diabetic CKD
3. Finerenone (Nonsteroidal MRA)
- FIDELIO-DKD and FIGARO-DKD trials: 18% relative risk reduction in CKD endpoint, 13% relative risk reduction in major adverse cardiovascular events in diabetes + CKD
- Safer potassium profile than steroidal MRAs (spironolactone, eplerenone)
- Now a pillar of the "triple therapy" in diabetic CKD: ACEi/ARB + SGLT2 inhibitor + finerenone
4. Dietary Modification
- Sodium: restrict to <2 g/day (especially with hypertension or heart failure)
- Potassium: restrict to 60 mEq/day if hyperkalemic; avoid tomatoes, bananas, potatoes, citrus
- Phosphate: restrict in advanced CKD; use phosphate binders if needed
- Protein: moderate restriction (0.6-0.8 g/kg/day) in later stages, though strict restriction has not consistently slowed progression
- Fluid: no restriction unless dilutional hyponatremia; overrestriction causes volume depletion
5. Glycemic Control (Diabetic CKD)
- HbA1c target ~7% (individualize in advanced CKD to avoid hypoglycemia)
- GLP-1 receptor agonists (e.g., semaglutide) showing emerging CV and renal benefit
- Avoid metformin at GFR <30 (risk of lactic acidosis)
6. Dyslipidemia
- Statins reduce cardiovascular events in CKD; start/continue in most CKD patients
- Less clear benefit once on dialysis (dialysis patients were excluded from major statin trials)
7. Anemia Management
- Correct iron deficiency first (IV iron preferred in dialysis patients)
- ESAs (epoetin alfa, darbepoetin): target Hb 10-11.5 g/dL; avoid over-correction (>13 g/dL increases stroke/thrombosis risk)
8. CKD-MBD Management
- Dietary phosphate restriction + phosphate binders (calcium carbonate, sevelamer, lanthanum carbonate)
- Active vitamin D analogs (calcitriol, paricalcitol) for 2° hyperparathyroidism
- Cinacalcet (calcimimetic) for refractory secondary hyperparathyroidism
- Parathyroidectomy if refractory tertiary hyperparathyroidism
9. Metabolic Acidosis
- Oral sodium bicarbonate supplementation (target serum HCO₃⁻ ≥22 mEq/L)
- May slow CKD progression and reduce muscle catabolism
10. Avoid Nephrotoxins
- NSAIDs: block renal autoregulatory mechanisms, worsen GFR acutely
- Iodinated contrast: minimize; use pre-hydration; avoid nephrotoxic combinations
- Aminoglycosides: use with great caution; monitor levels
- Adjust drug doses based on eGFR
11. Preparation for RRT
- Refer to nephrology when eGFR approaches 20-30 mL/min/1.73 m²
- Discuss modalities early: hemodialysis (HD), peritoneal dialysis (PD), or preemptive transplantation
- Arrange arteriovenous fistula creation well in advance of anticipated need (6-12 months)
- Initiation of dialysis should be based on symptoms and metabolic/nutritional status, not on a GFR target alone - starting at a fixed eGFR has not shown mortality benefit
When to Refer / Urgent Indications for Dialysis
Indications for urgent dialysis (AEIOU mnemonic):
- Acidosis (severe, pH <7.1-7.2, refractory)
- Electrolyte disturbance (hyperkalemia refractory to medical management)
- Intoxication (dialyzable toxins: methanol, ethylene glycol, salicylates, lithium)
- Overload (volume/fluid overload refractory to diuretics)
- Uremia (uremic pericarditis, encephalopathy, bleeding)
Prognosis / Global Burden
-
CKD affects approximately 20 million persons in the US alone and is a leading global cause of morbidity and mortality
-
Without effective prevention and treatment, global years of life lost due to CKD are projected to rise from 26 million (2016) to 52.5 million by 2040, with CKD mortality expected to triple to 3.1 million deaths/year
-
CKD is forecast to rise in YLL rankings from 16th (2016) to 5th by 2040, driven by the global diabetes and hypertension epidemic
-
Harrison's Principles of Internal Medicine 22E (2025); National Kidney Foundation Primer 8e; Brenner and Rector's The Kidney
Key message: CKD management has been transformed by SGLT2 inhibitors (benefit even in non-diabetic CKD) and finerenone. Combined with RAAS blockade and tight BP control, these form the evidence-based backbone of nephroprotection, with the goal of delaying or preventing ESKD and reducing the excess cardiovascular mortality that CKD patients face.
This is a shared conversation. Sign in to Orris to start your own chat.