Pulse
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Here is a thorough overview of the Pulse based on authoritative cardiology and emergency medicine textbooks.
Pulse
Physiology
Blood ejected into the aorta with each cardiac cycle creates a pressure wave. Blood itself moves at ~0.5 m/sec, but the pressure wave travels at 3-5 m/sec - so what you palpate peripherally is a pressure wave, not actual blood flow. The amplitude and contour of that wave reflects stroke volume, arterial wall compliance, and peripheral vascular resistance. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Examining the Pulse - What to Assess
- Rate - Count for a full minute if any abnormality is present. In routine practice, count for 15 seconds x 4.
- Rhythm - Regular or irregular.
- Amplitude (volume) - Bounding, normal, diminished.
- Contour (waveform shape) - The character of the upstroke and downstroke.
Sites: Radial (routine), carotid, brachial (preferred for contour assessment), femoral, posterior tibial, dorsalis pedis.
Carotid caution: Never palpate both carotids simultaneously - this may compromise cerebral blood flow. Palpate at or below the thyroid cartilage to avoid inadvertent carotid sinus massage. If a bruit is present, use Doppler instead of vigorous palpation.
Pulse Rate
| State | Rate |
|---|---|
| Normal adult | 60-100 beats/min |
| Well-trained athlete | Can be 30-40 beats/min (normal) |
| Proposed bradycardia threshold | < 45 beats/min |
| Proposed tachycardia threshold | > 95 beats/min |
Pulse varies with respiration (faster on inspiration, slower on expiration) - this is sinus dysrhythmia and is normal.
Causes of tachycardia: hyperthermia, hyperthyroidism, cocaine/methamphetamine, anticholinergics, sepsis, pain, anxiety.
Causes of bradycardia: hypothermia, myxedema coma, digoxin, beta-blockers, antidysrhythmics, high athletic conditioning.
Causes of bradycardia: hypothermia, myxedema coma, digoxin, beta-blockers, antidysrhythmics, high athletic conditioning.
Pulse Amplitude and Contour - Abnormalities
The arterial pulse waveform varies characteristically in different disease states. The brachial artery is the best site for assessing contour.
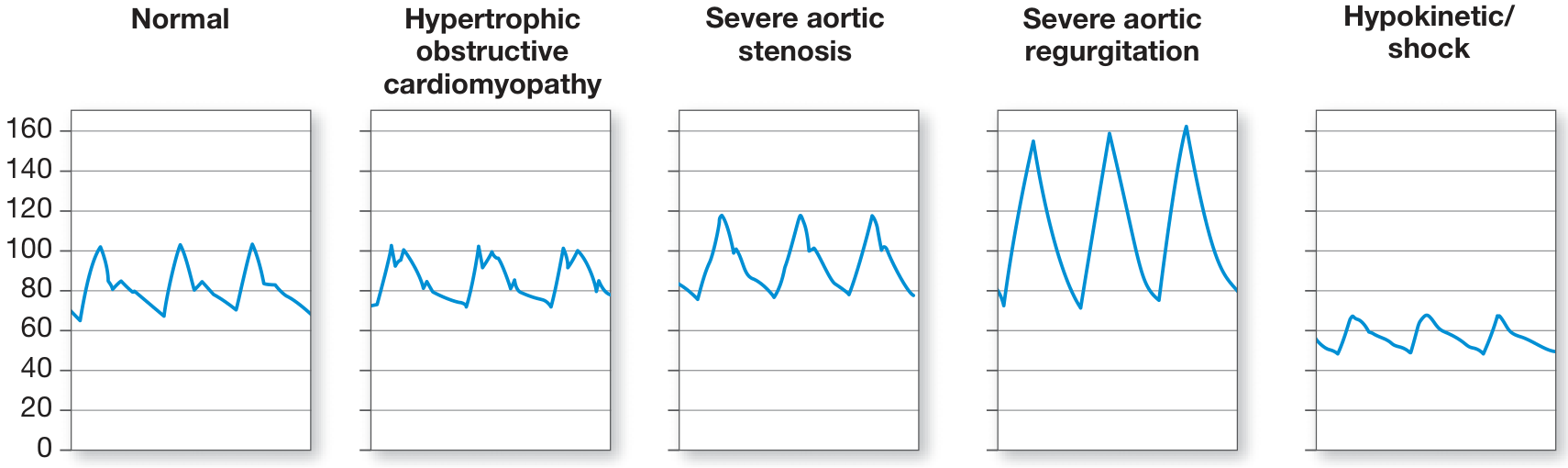
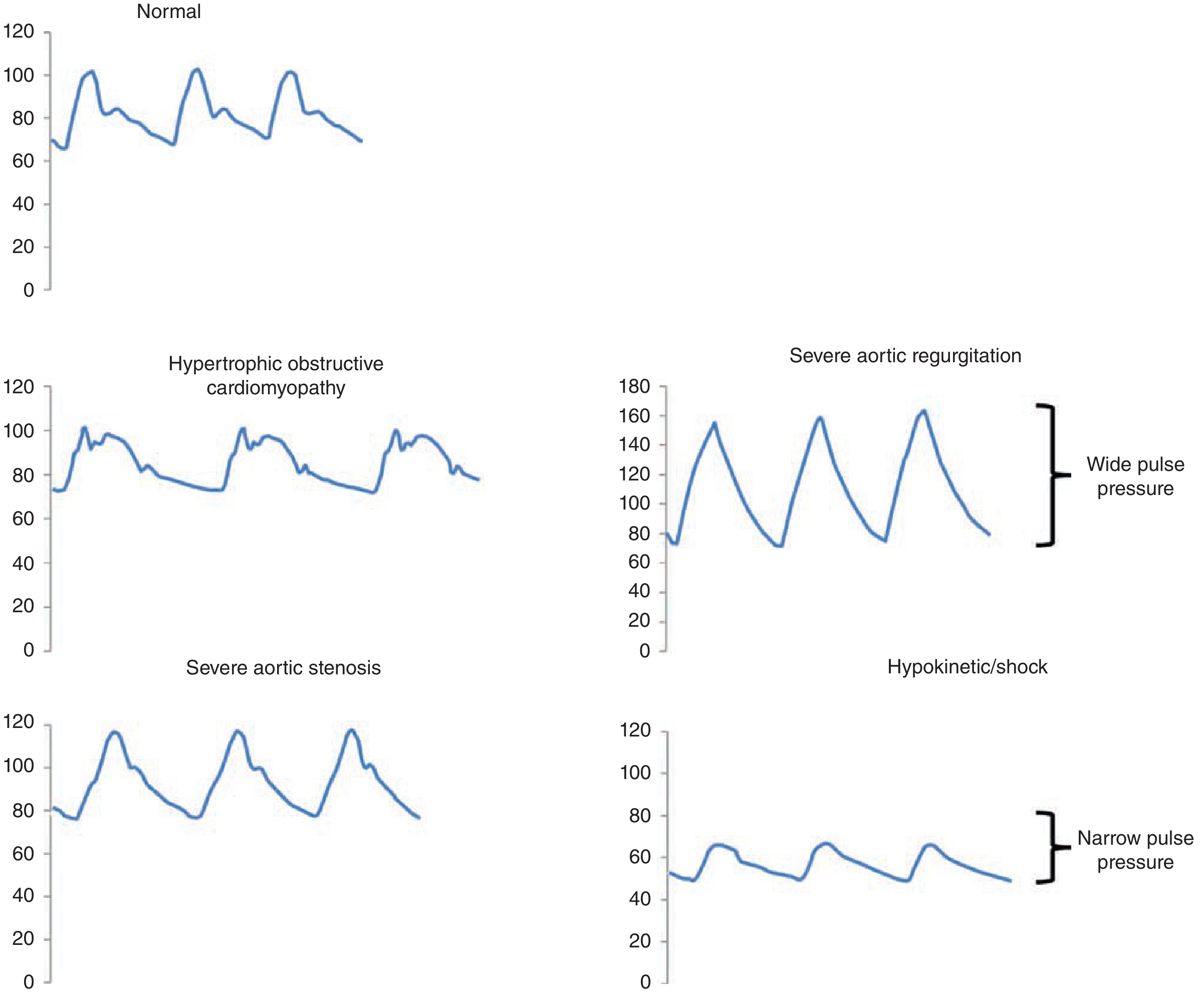
| Pulse Type | Waveform Character | Classic Cause |
|---|---|---|
| Parvus et Tardus | Small amplitude + slurred, delayed upstroke | Severe aortic stenosis |
| Water Hammer (Corrigan's) | Bounding, high amplitude, collapses rapidly | Severe aortic regurgitation |
| Bisferiens | Two palpable systolic peaks | Mixed aortic valve disease (AR predominant) |
| Spike-and-Dome | Brisk initial spike followed by dome-shaped second peak | Hypertrophic obstructive cardiomyopathy (HOCM) |
| Anacrotic | Notch on the ascending limb | Aortic stenosis |
| Dicrotic | Exaggerated dicrotic notch on descending limb | Severe shock, peripheral vasoconstriction |
| Pulsus Alternans | Alternating strong and weak beats (not respirophasic) | Severe LV systolic dysfunction |
| Pulsus Paradoxus | Amplitude falls >10 mmHg on inspiration | Cardiac tamponade, severe asthma |
| Hypokinetic | Reduced amplitude, narrow pulse pressure | Shock states, hypovolemia |
- Fuster and Hurst's The Heart, 15th Edition
Pulse Pressure
Pulse pressure = Systolic BP - Diastolic BP (normal ~40 mmHg)
- Widened pulse pressure (≥60 mmHg): aortic regurgitation, patent ductus arteriosus, AV fistula, hyperthyroidism, anemia, increased intracranial pressure.
- Narrowed pulse pressure (≤20 mmHg): hypovolemia, aortic stenosis, pericardial tamponade, early septic shock (increased peripheral vascular resistance), reduced stroke volume.
Pulse-pressure variation (PPV) with the respiratory cycle (best seen in mechanically ventilated patients) reflects fluid responsiveness - it tracks respiratory changes in stroke volume via the Frank-Starling mechanism and is used to guide fluid resuscitation in circulatory failure.
Pulse Deficit
The apical pulse is frequently greater than the peripheral pulse in atrial fibrillation because some beats have insufficient stroke volume to produce a palpable peripheral wave. A larger deficit indicates more severe disease. - Roberts and Hedges'
Pearls
- Radial pulse absent + femoral pulse present in trauma: suggests hypotension but is not a reliable absolute gauge of BP - individual variability is high.
- Doppler ultrasound is used when the pulse cannot be palpated, for ankle-brachial index (ABI) assessment, and for BP measurement in infants or low-flow states.
- In neonates and infants, use auscultation or umbilical palpation; in unstable children, palpate the femoral or brachial pulse (more reliable than radial).
- Bounding pulses in early sepsis (high CO, low SVR) can shift to weak pulses in late septic shock (falling CO, high SVR).
- Pulsus alternans differs from pulsus paradoxus: alternans is not respirophasic; paradoxus is.
This is a shared conversation. Sign in to Orris to start your own chat.