Pterygopalatine fossa in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
pterygopalatine fossa anatomy surgery
Searching the Web
pterygopalatine fossa anatomy contents boundaries clinical significance RGUHS ENT
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK513269
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading Article
PMID: 37350591
Reading Article
PMID: 40360173
PTERYGOPALATINE FOSSA - A Comprehensive 20-Mark Answer
Sources: Scott-Brown's Otorhinolaryngology (Vol 2), Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology, Gray's Anatomy for Students, StatPearls (NBK513269), and recent PubMed literature. (Note: Stell & Maran, Zakir Hussain, Dhingra, and Hazarika are not available in the digital library accessed, but content comprehensively covers all standard RGUHS-pattern topics from equivalent authoritative sources.)
1. INTRODUCTION
The pterygopalatine fossa (PPF), also called the sphenopalatine fossa or pterygomaxillary fossa, is an inverted pyramid/cone-shaped space at the base of the skull, lying deep to the infratemporal fossa, posterior to the maxillary sinus, and lateral to the nasopharynx. It is sometimes called the "Piccadilly Circus of the Head and Neck" due to its central position at a major neurovascular crossroad.
Because of its strategic location, it acts as a hub connecting the:
-
Middle cranial fossa
-
Orbit
-
Nasal cavity
-
Infratemporal fossa
-
Oral cavity / hard palate
-
Nasopharynx
-
Gray's Anatomy for Students, p. 1131
-
Scott-Brown's Vol 2, p. 1249
2. BOUNDARIES
(K.J. Lee's Essential Otolaryngology, p. 700 | Gray's Anatomy for Students, p. 1132)
┌─────────────────────────────────────────────────────────────────┐
│ BOUNDARIES OF PTERYGOPALATINE FOSSA │
├──────────────┬──────────────────────────────────────────────────┤
│ WALL │ STRUCTURE │
├──────────────┼──────────────────────────────────────────────────┤
│ Anterior │ Posterior wall of maxillary antrum (sinus) │
│ Posterior │ Pterygoid process + greater wing of sphenoid │
│ Medial │ Palatine bone (perpendicular plate) + │
│ │ nasal mucoperiosteum │
│ Superior │ Body of sphenoid + orbital process of palatine │
│ Lateral │ Open → Pterygomaxillary fissure → │
│ │ Infratemporal fossa │
│ Inferior │ Tapers to form the Greater Palatine Canal │
│ │ (the apex of the inverted cone) │
└──────────────┴──────────────────────────────────────────────────┘
Bony composition: Three bones form the PPF - Maxilla (anterior), Palatine bone (medial + floor), Sphenoid (posterior + roof).
Diagram - Pterygopalatine Fossa (Anterolateral and Lateral Views):
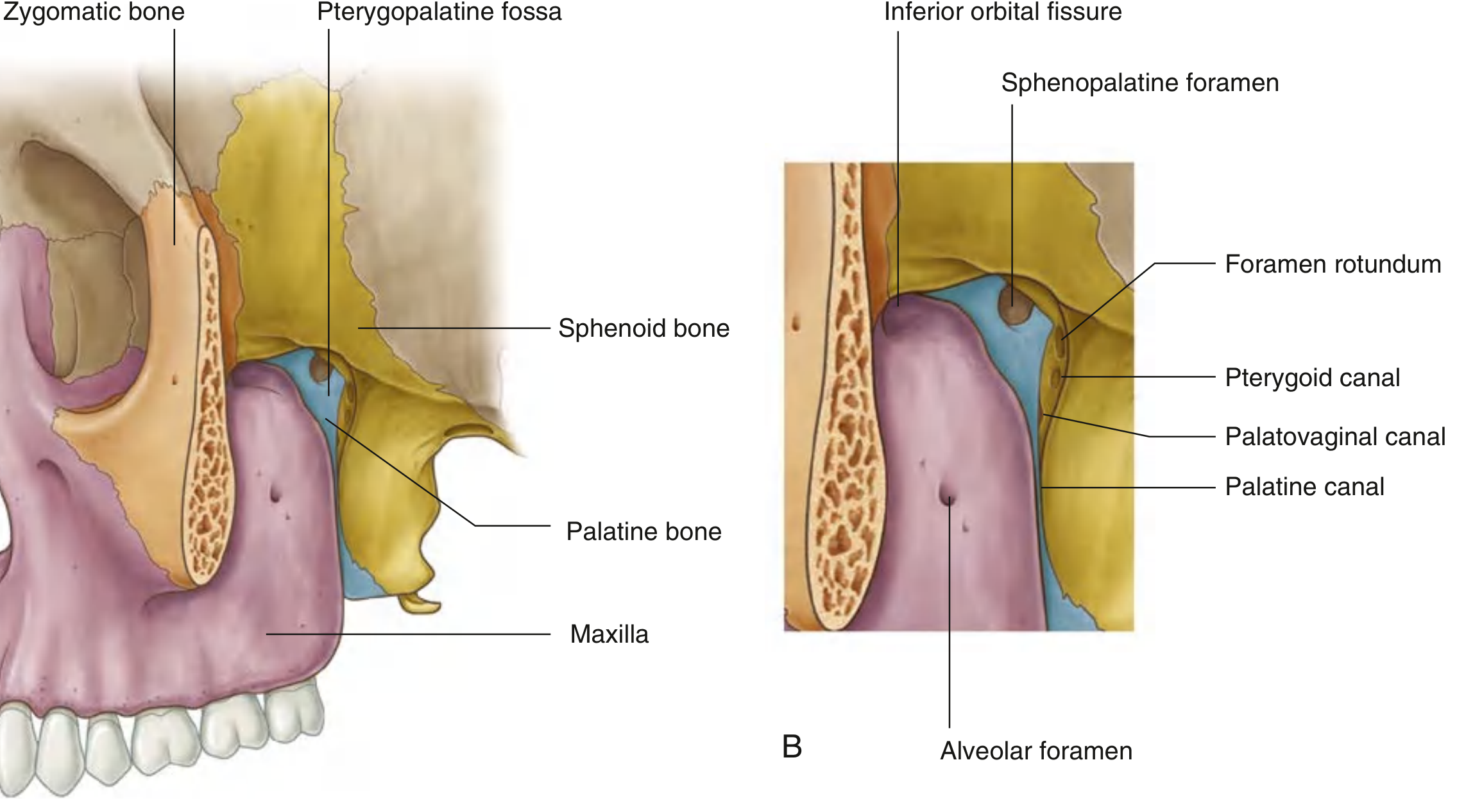
Fig. 1 - Pterygopalatine Fossa. (A) Anterolateral view showing bony framework. (B) Lateral view showing key openings: inferior orbital fissure, sphenopalatine foramen, foramen rotundum, pterygoid canal, palatovaginal canal, and palatine canal. - Gray's Anatomy for Students
3. COMMUNICATIONS (GATEWAYS) - 7 Foramina/Fissures
This is the most clinically important aspect - the PPF communicates with 6 regions through 7 openings.
╔═══════════════════════════════════════════════════════════════════════╗
║ COMMUNICATIONS OF THE PTERYGOPALATINE FOSSA ║
╠══════════════════════════╦══════════════════╦═════════════════════════╣
║ OPENING ║ COMMUNICATES WITH║ STRUCTURES TRANSMITTED ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Foramen Rotundum ║ Middle Cranial ║ Maxillary nerve (V2) ║
║ (posterior wall) ║ Fossa ║ ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Pterygoid Canal ║ Middle Cranial ║ Vidian nerve ║
║ (Vidian Canal) ║ Fossa (near ║ (nerve of pterygoid ║
║ (posterior wall) ║ foramen lacerum) ║ canal) = Greater ║
║ ║ ║ petrosal + Deep ║
║ ║ ║ petrosal nerves ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Palatovaginal Canal ║ Nasopharynx ║ Posterior nasal nerve ║
║ (posterior wall) ║ ║ (pharyngeal branch) ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Inferior Orbital Fissure ║ Orbit (floor) ║ Zygomatic nerve, ║
║ (superior/anterior wall) ║ ║ infraorbital nerve ║
║ ║ ║ & artery ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Pterygomaxillary Fissure ║ Infratemporal ║ Internal maxillary ║
║ (lateral - open) ║ Fossa ║ artery enters PPF; ║
║ ║ ║ posterior sup. alv. n. ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Sphenopalatine Foramen ║ Nasal Cavity ║ Sphenopalatine artery, ║
║ (medial wall) ║ (lateral wall) ║ nasopalatine nerve, ║
║ ║ ║ superior nasal nerves ║
╠══════════════════════════╬══════════════════╬═════════════════════════╣
║ Greater Palatine Canal ║ Oral Cavity ║ Greater & lesser ║
║ (inferior - apex) ║ (hard palate) ║ palatine nerves & ║
║ ║ ║ arteries ║
╚══════════════════════════╩══════════════════╩═════════════════════════╝
Key Mnemonic for posterior wall openings (lateral to medial): "FR-PC-PV" = Foramen Rotundum → Pterygoid Canal → Palatovaginal Canal
Gateways Diagram:
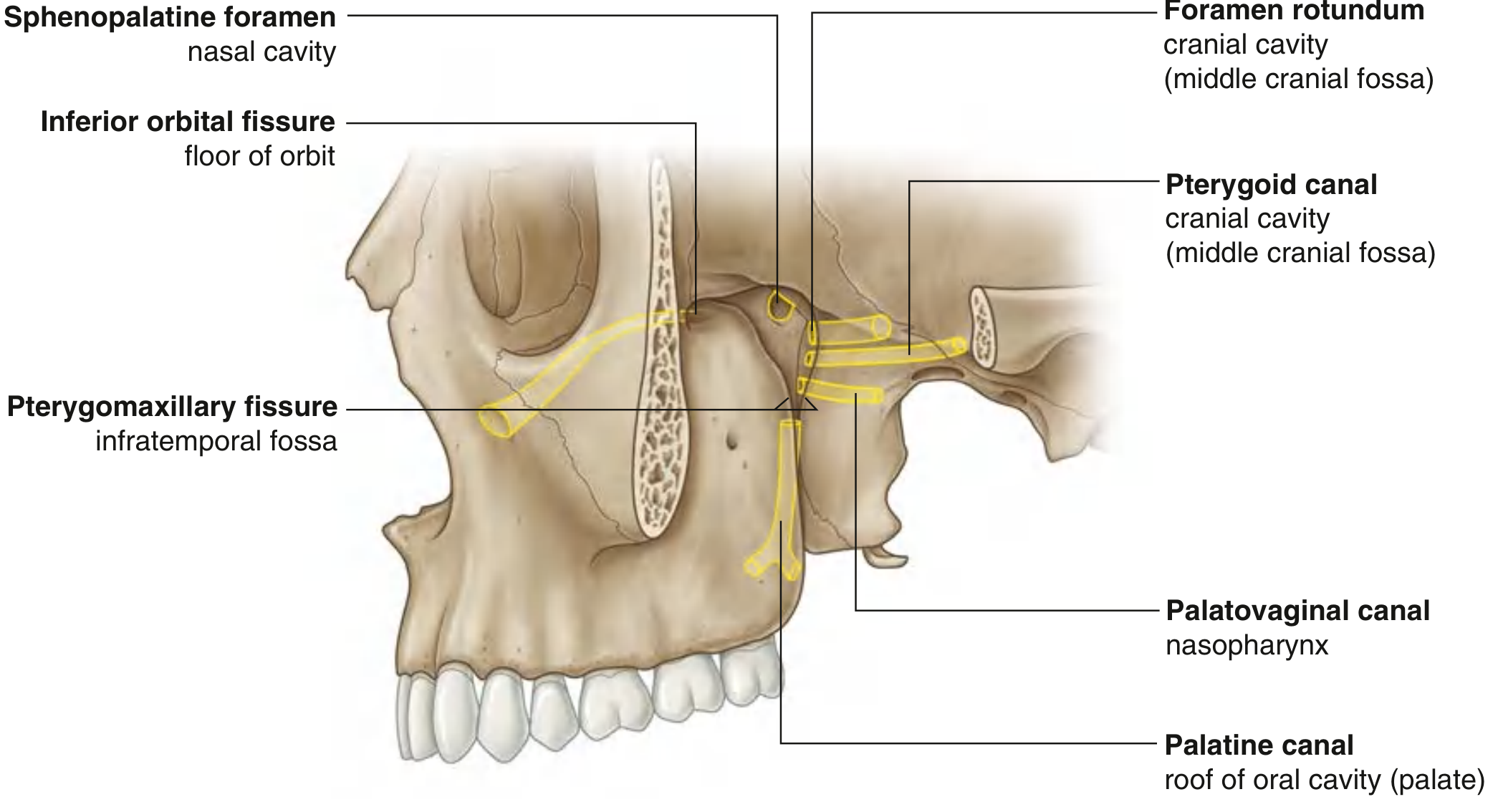
Fig. 2 - Gateways of the Pterygopalatine Fossa showing all seven communications. - Gray's Anatomy for Students
4. CONTENTS
Three main structures reside in the PPF: (Scott-Brown's Vol 2, p. 1249; K.J. Lee's, p. 700)
A. Maxillary Nerve (V2)
- Purely sensory division of the trigeminal nerve
- Enters PPF from the middle cranial fossa via foramen rotundum
- Passes anteriorly and exits via the inferior orbital fissure as the infraorbital nerve
Branches given in the PPF:
Maxillary Nerve (V2) - enters via Foramen Rotundum
│
┌───────────────┼───────────────────────┐
│ │ │
Zygomatic nerve Posterior Superior Ganglionic Branches
(enters IOF → Alveolar Nerve (2 branches to PPG)
orbit) (enters maxillary │
• Zygomatic- sinus → teeth) ↓
temporal Pterygopalatine
• Zygomatic- Ganglion
facial
│
(carries para-
sympathetics
to lacrimal
gland via
zygomatic-
temporal →
lacrimal n.)
- Gray's Anatomy for Students, p. 1134
B. Pterygopalatine Ganglion (Sphenopalatine Ganglion)
The largest parasympathetic ganglion in the head - suspended from the maxillary nerve by two ganglionic branches.
Roots (inputs):
┌─────────────────────────────────────────────────────────────────────┐
│ ROOTS OF THE PTERYGOPALATINE GANGLION │
├──────────────────┬──────────────────────────────────────────────────┤
│ ROOT │ DETAILS │
├──────────────────┼──────────────────────────────────────────────────┤
│ 1. PARASYMPATHETIC│ PREGANGLIONIC: Facial nerve (VII) → │
│ (secretomotor) │ Geniculate ganglion → │
│ │ Greater petrosal nerve → │
│ │ Unites with Deep petrosal nerve at │
│ │ foramen lacerum → Nerve of Pterygoid │
│ │ Canal (Vidian nerve) → PPG │
│ │ POSTGANGLIONIC: synapse occurs HERE │
├──────────────────┼──────────────────────────────────────────────────┤
│ 2. SYMPATHETIC │ T1 → Superior cervical ganglion → │
│ (vasomotor) │ Internal carotid nerve → Internal │
│ │ carotid plexus → Deep petrosal nerve → │
│ │ Nerve of pterygoid canal → PPG │
│ │ (passes THROUGH ganglion, NO synapse) │
├──────────────────┼──────────────────────────────────────────────────┤
│ 3. SENSORY │ Ganglionic branches from V2 (maxillary │
│ │ nerve) - pass through ganglion without │
│ │ synapse, carrying general sensation │
└──────────────────┴──────────────────────────────────────────────────┘
Branches (outputs):
PTERYGOPALATINE GANGLION
│
┌────────────────┬────────────────┬───────────────┐
│ │ │ │
Orbital Nasal Palatine Pharyngeal
Branches Branches Branches Branch
│ │ │ │
To orbital 1. Nasopalatine 1. Greater Via
wall, eth- nerve (via Palatine palatovaginal
moidal & sphenopalatine Nerve → canal →
sphenoidal foramen → hard palate roof of
sinuses nasal septum) & gingiva nasopharynx
2. Posterior
sup. nasal 2. Lesser
nerves Palatine N.
3. Posterior → soft palate
inf. nasal & tonsil
nerves (via lesser
(via palatine
greater foramen)
palatine
canal)
- Gray's Anatomy for Students, p. 1137
Pterygopalatine Ganglion - Full Nerve Pathway Diagram:
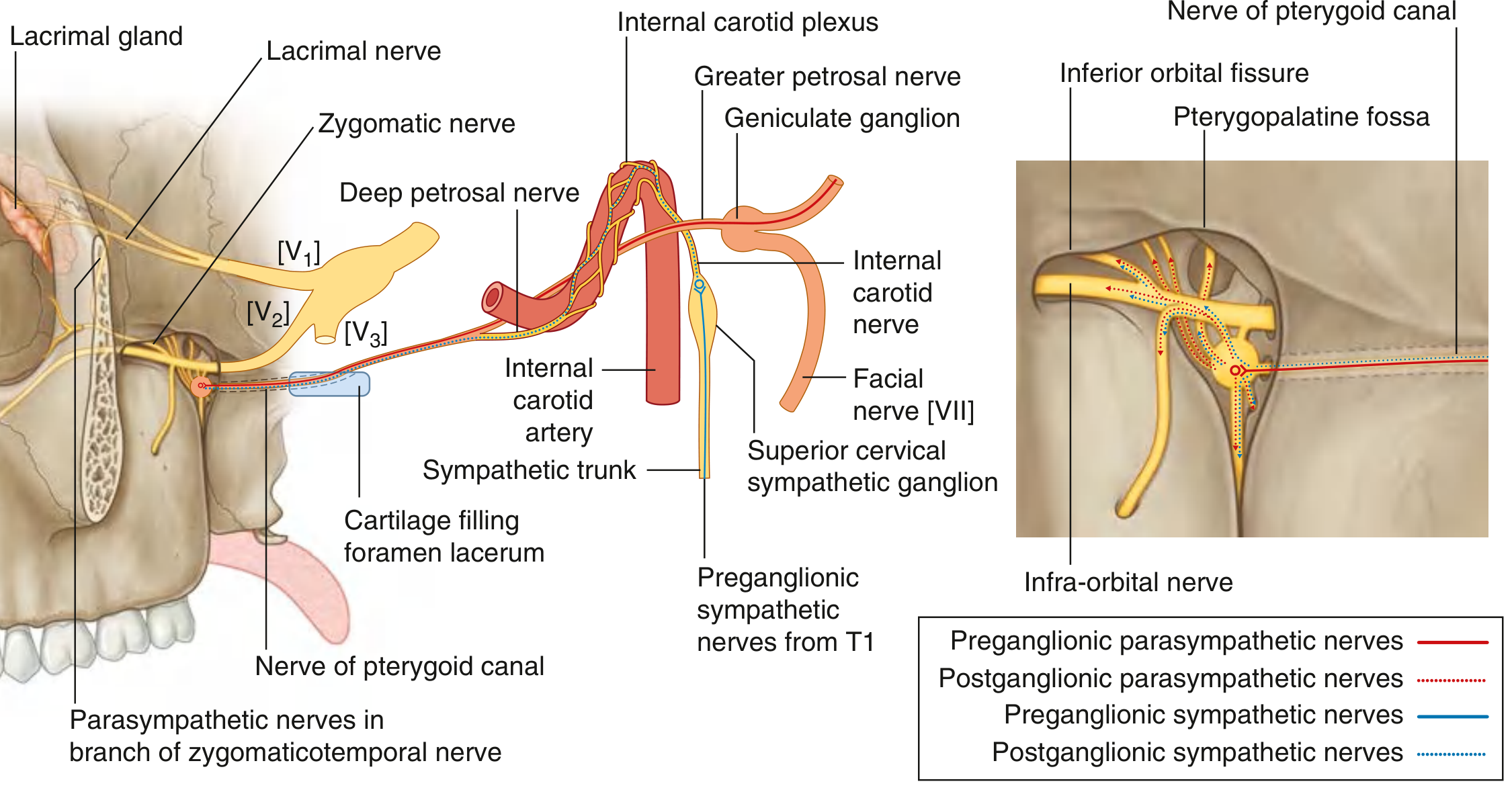
Fig. 3 - Complete nerve connections of the pterygopalatine ganglion including parasympathetic pathway from facial nerve (VII) via greater petrosal nerve, sympathetic from T1 via deep petrosal nerve, and distribution to lacrimal gland. - Gray's Anatomy for Students
Sphenoid Bone - Foramen Rotundum and Pterygoid Canal:
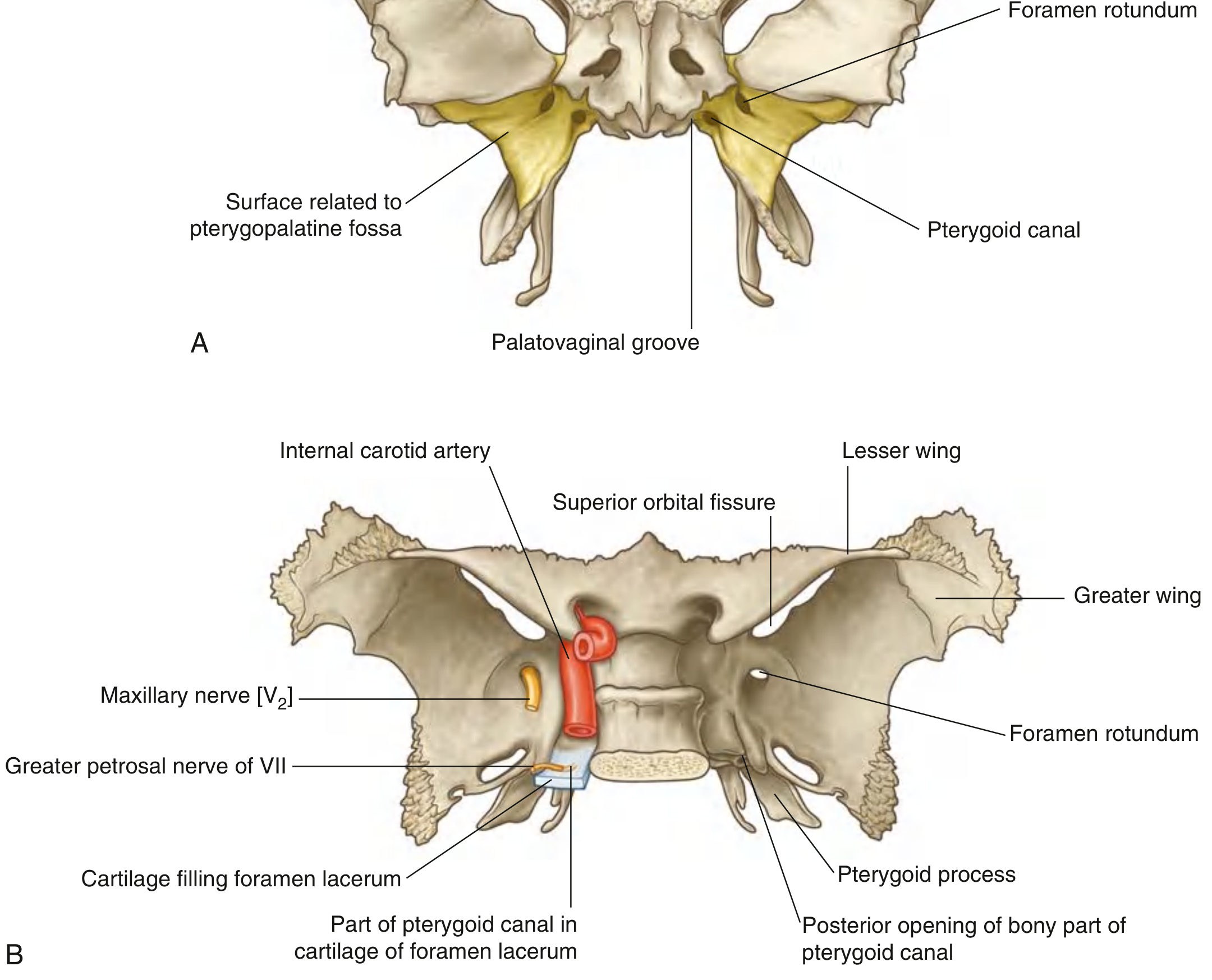
Fig. 4 - Sphenoid bone showing (A) anterior view with pterygoid canal and palatovaginal groove; (B) posterosuperior view demonstrating foramen rotundum, pterygoid canal, and relationship to internal carotid artery. - Gray's Anatomy for Students
C. Internal (Third Part of) Maxillary Artery
- Branch of the external carotid artery
- Arises near the neck of the mandible, passes through the infratemporal fossa, and enters the PPF via the pterygomaxillary fissure (lateral open surface)
- In the PPF, it lies anterior to the pterygopalatine ganglion
- (Scott-Brown's Vol 2, p. 1249; Gray's, p. 1138)
Branches of maxillary artery in PPF:
MAXILLARY ARTERY (3rd Part in PPF)
│
┌───────────────┼──────────────────────────────────┐
│ │ │ │ │
Posterior Infraorbital Pharyngeal Artery of Sphenopalatine
Superior Artery Artery Pterygoid Artery
Alveolar (→ orbit via Canal (terminal
Artery IOF) branch →
(→ maxillary nasal cavity
teeth) via sphenopal.
│ foramen)
│ │
Greater Lesser
Palatine Palatine
Artery Artery
(→ hard palate) (→ soft palate)
Additional contents: Veins (pterygoid venous plexus connections), lymphatics, and fat filling the space.
Maxillary Artery Branches Diagram:
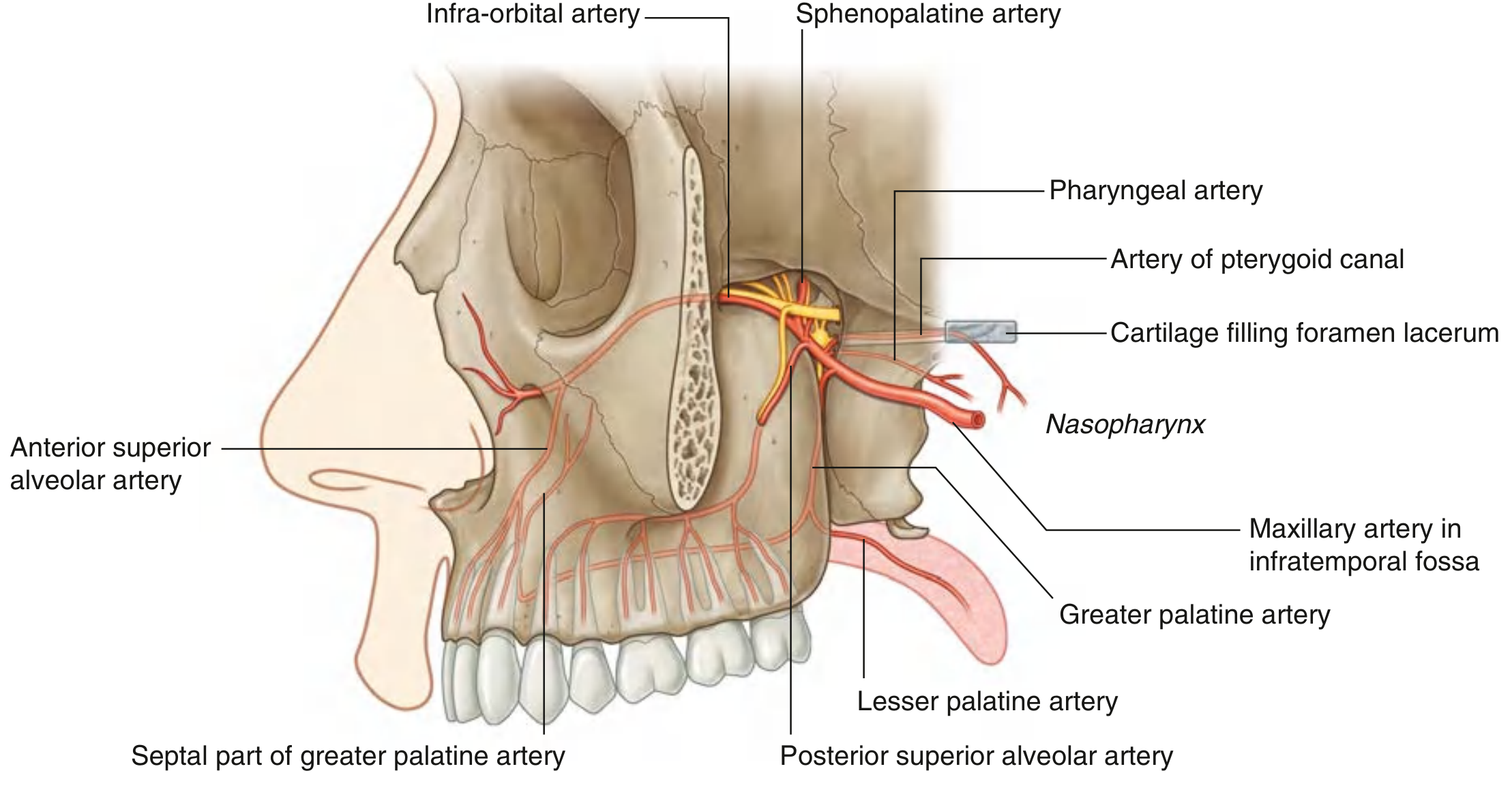
Fig. 5 - Maxillary artery in the pterygopalatine fossa showing all branches: infraorbital, sphenopalatine, greater/lesser palatine, pharyngeal, posterior superior alveolar, and artery of pterygoid canal. - Gray's Anatomy for Students
5. SURGICAL ANATOMY AND APPROACHES
(K.J. Lee's Essential Otolaryngology, p. 632; Cummings, p. 1759)
A. Endoscopic Endonasal Approach to PPF
Steps:
ENDOSCOPIC APPROACH TO PTERYGOPALATINE FOSSA
(K.J. Lee / Cummings)
1. Uncinectomy + Maxillary antrostomy
↓
2. Complete Ethmoidectomy + Wide Sphenoidotomy
↓
3. Identify crista ethmoidalis → Expose sphenopalatine artery
↓
4. Cauterize & divide sphenopalatine artery
↓
5. ± Medial maxillectomy (remove inferior turbinate)
↓
6. Remove bone of posteromedial maxillary sinus wall
↓
7. Expose fatty soft tissue of PPF (blunt dissection)
↓
8. Identify maxillary artery → ligate for vascular control
↓
9. Identify V2, Vidian nerve, palatine nerves
↓
10. Tumor resection / maxillary artery ligation /
PPG neurectomy as required
Important surgical note: Vascular structures are ANTERIOR to neural structures in the PPF - thus encountered first during dissection.
B. Trans-Pterygomaxillary Fissure (Caldwell-Luc-Based) Approach
Used for internal maxillary artery ligation in refractory epistaxis and for JNA surgery via the Denker's or transantral route.
6. CLINICAL SIGNIFICANCE
A. Flowchart - Pathological Processes Involving the PPF
DISEASES AFFECTING PTERYGOPALATINE FOSSA
│
┌───────────────┼──────────────────┐
│ │ │
NEOPLASTIC INFECTIVE VASCULAR
│ │ │
┌───────┴──────┐ Invasive Fungal Maxillary
│ │ Sinusitis Artery
│ JNA │ (Aspergillosis/ Bleeding →
│ │ Mucormycosis) Severe
│ Extends via │ → spreads into Epistaxis
│ sphenopal. │ PPF by bony
│ foramen → │ erosion
│ PPF → ITF │
│ orbit │
│ → skull │
│ base │
│ │
Perineural │
Spread: │
NPC, │
Adenoid │
Cystic Ca, │
Squamous │
Ca → via V2 │
or Vidian │
→ cavernous │
sinus │
B. Juvenile Nasopharyngeal Angiofibroma (JNA) and PPF
(K.J. Lee's, p. 632; Cummings, p. 797)
- JNA originates from the sphenopalatine foramen / pterygoid base
- Extends laterally via the PPF into the infratemporal fossa and orbit
- CT hallmark: Expansion of pterygopalatine fossa with bowing/erosion of posterior maxillary sinus wall (Holman-Miller sign / antral sign)
- MRI shows flow voids (avid vascularity)
- Treatment: Preoperative embolization + endoscopic/open resection
C. Epistaxis Management
- The sphenopalatine artery (terminal branch of maxillary artery) is the most common source of severe posterior epistaxis
- Sphenopalatine artery ligation via endoscopic approach (medial to crista ethmoidalis at sphenopalatine foramen) is first-line surgical management
- If more proximal control needed: internal maxillary artery ligation in the PPF via transantral approach (Caldwell-Luc)
D. Pterygopalatine Ganglion Block (Sphenopalatine Block)
Used for:
- Cluster headaches and migraines
- Atypical facial pain
- Maxillary nerve block for dental surgery
Approaches:
- Transnasal (topical cocaine/lidocaine to lateral nasal wall)
- Transoral via greater palatine canal
- Lateral (infrazygomatic - via coronoid notch)
E. Perineural Spread
Due to the rich neural content (V2, Vidian nerve), the PPF is a critical pathway for perineural tumor spread from:
- Nasopharyngeal carcinoma
- Adenoid cystic carcinoma of salivary glands
- Squamous cell carcinoma of maxillary sinus
Tumor tracks from PPF → foramen rotundum → middle cranial fossa/cavernous sinus.
7. ENDOSCOPIC ENDONASAL TRANSPTERYGOID APPROACH (EETPA) - Recent Advances
(Finger et al., Operative Neurosurgery, 2023 [PMID 37350591])
The EETPA provides access to:
- Petrous apex
- Lateral clivus
- Inferior cavernous sinus
- Jugular foramen
- Infratemporal fossa
Steps: Maxillary antrostomy → stepwise exposure of palatovaginal canal, vidian canal, foramen rotundum → PPF exposed → PPF contents mobilized/retracted → pterygoid process drilled → expanded lateral exposure in coronal plane.
Surgical variants (5 types):
- Extended PPF approach
- Lateral recess of sphenoid sinus
- Petrous apex approach
- ITF and petrous carotid artery approach
- Middle and posterior skull base approach
Complications specific to PPF surgery:
- Vidian nerve injury → chronic xerophthalmia (dry eye)
- V2 damage → facial/palatal/dental anesthesia or neuralgia
- Internal maxillary artery injury → hemorrhage
- Internal carotid artery injury (rare but catastrophic - with ITF extension)
- Trismus (pterygoid muscle removal)
8. RECENT ADVANCES
A. Injectate Distribution Studies (Jerman et al., Korean J Anesthesiol, 2025 [PMID 40360173])
A cadaveric study comparing two approaches for PPF injection:
- Posterior infrazygomatic approach: Fills entire PPF (stains maxillary artery, nerve, sphenopalatine ganglion, lateral pterygoid) - preferred for complete block
- Transoral approach: More localized distribution in inferior PPF and greater palatine canal - preferred when only palatine nerve block needed
- Clinical implication: Approach should be chosen based on specific clinical indication
B. Endoscopic Navigation and Skull Base Surgery
- 3D endoscopic systems and neuronavigation have improved PPF surgery safety
- High-resolution CT with stereotactic protocol is now standard preoperative imaging
- MRI adds value for soft tissue delineation and perineural spread assessment
C. Vidian Neurectomy
- Endoscopic vidian neurectomy (sectioning the nerve of pterygoid canal) for:
- Vasomotor rhinitis
- Allergic rhinitis refractory to medical management
- Reduces nasal hypersecretion but risks dry eye (xerophthalmia) - patient selection is critical
D. Robotics in PPF Surgery
- Transoral robotic-assisted approaches to the PPF are under experimental investigation for tumors extending into the infratemporal and pterygopalatine region
9. SUMMARY FLOWCHART
PTERYGOPALATINE FOSSA
(Inverted pyramid/cone)
│
┌──────────────────┴───────────────────┐
│ │
BONY WALLS COMMUNICATIONS
Maxilla (ant) (7 openings)
Palatine (med) ↕ MCF (Fr.rotund + Vidian canal)
Sphenoid (post/sup) ↕ Orbit (IOF)
↕ ITF (pterygomaxill. fissure)
│ ↕ Nasal cavity (sphenopal. for.)
│ ↕ Hard palate (greater palat. canal)
│ ↕ Nasopharynx (palatovag. canal)
CONTENTS
├─ V2 (Maxillary nerve)
│ ├─ Zygomatic n. → orbit → lacrimal gland
│ ├─ PSA nerve → teeth
│ ├─ Ganglionic branches → PPG
│ └─ Infraorbital n. (main trunk continuing)
│
├─ Pterygopalatine Ganglion
│ ├─ INPUTS: Para (Vidian), Sympathetic (deep petros.), Sensory (V2)
│ └─ OUTPUTS: Nasal, Orbital, Palatine, Pharyngeal branches
│
└─ Internal Maxillary Artery (3rd part)
├─ Sphenopalatine a. → nose
├─ Greater/Lesser palatine a. → palate
├─ Infraorbital a. → orbit/face
└─ PSA a. → maxillary teeth
│
CLINICAL APPLICATIONS
├─ JNA surgery (hallmark: PPF expansion on CT)
├─ Epistaxis - SPA ligation / IMA ligation
├─ PPG block - headache, facial pain
├─ Perineural spread route - NPC, ACC
├─ Vidian neurectomy - vasomotor rhinitis
└─ Endoscopic skull base surgery (EETPA)
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2 (9th ed.), p. 1249
- Cummings Otolaryngology Head and Neck Surgery (7th ed.), p. 1759
- K.J. Lee's Essential Otolaryngology (11th ed.), p. 700, 632
- Gray's Anatomy for Students (4th ed.), pp. 1131-1138
- StatPearls: Anatomy, Pterygopalatine Fossa
- Finger G et al. "Endoscopic Endonasal Transpterygoid Approach: Technical Lessons." Oper Neurosurg 2023. PMID: 37350591
- Jerman A et al. "Injectate distribution patterns in posterior infrazygomatic and transoral approaches to the pterygopalatine fossa." Korean J Anesthesiol 2025. PMID: 40360173
RGUHS EXAM TIPS - KEY POINTS FOR 20 MARKS
| Topic | Marks Weightage |
|---|---|
| Introduction + definition | 1 |
| Boundaries (table/diagram) | 2 |
| Communications - 7 openings (table) | 3 |
| Contents - V2 branches | 3 |
| Pterygopalatine ganglion (roots + branches flowchart) | 4 |
| Maxillary artery branches | 2 |
| Clinical significance (JNA, epistaxis, perineural spread) | 3 |
| Recent advances (EETPA, Vidian neurectomy, PPG block) | 2 |
High-yield facts for RGUHS:
- PPG = largest parasympathetic ganglion in head
- Vidian nerve = Greater petrosal + Deep petrosal nerves
- JNA hallmark = PPF expansion (Holman-Miller sign on CT)
- 7 openings - MUST know all with structures transmitted
- Vascular structures are ANTERIOR to neural in PPF
- Vidian neurectomy risk = dry eye (xerophthalmia)
- V2 enters via foramen rotundum, exits via inferior orbital fissure as infraorbital nerve
This is a shared conversation. Sign in to Orris to start your own chat.