I just completed sarcoidosis from robbins
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have everything I need from Robbins to build a thorough revision note. Here it is:
Sarcoidosis - Robbins Revision Notes
Quick Recall Box
| Feature | Key Fact |
|---|---|
| Etiology | Unknown (multisystem granulomatous disease) |
| Histology | Non-caseating epithelioid granuloma |
| Key cells | CD4+ Th1 cells (driver); epithelioid macrophages |
| Most common presentation | Bilateral hilar lymphadenopathy on CXR |
| Lung involvement | 90% of patients |
| Unique epidemiology | Higher prevalence in nonsmokers (unique among lung diseases) |
Epidemiology
- Adults < 40 years predominantly affected
- Higher incidence in Danish/Swedish populations and African Americans (2-3x more than European descent)
- Unique feature: higher prevalence among nonsmokers - virtually unique to sarcoidosis among pulmonary diseases
Pathogenesis
Disordered immune regulation in genetically predisposed individuals exposed to undefined environmental agents.
Immunologic clues (all CD4+ Th1 driven):
- Intraalveolar and interstitial accumulation of CD4+ Th1 cells
- Oligoclonal expansion of CD4+ Th1 T cells within the lung
- Increased Th1 cytokines: IL-2 (T-cell proliferation) and IFN-γ (macrophage activation)
- Increased IL-8, TNF, MIP-1α → recruit more T cells and monocytes → granuloma formation
Paradox: Blood CD4+ T cells are often LOW → associated with anergy to common skin test antigens (Candida, PPD)
After lung transplantation, sarcoidosis recurs in the new lungs in at least one-third of patients.
Morphology (MORPHOLOGY box - HIGH YIELD)
Cardinal feature: Non-necrotizing (non-caseating) epithelioid granuloma
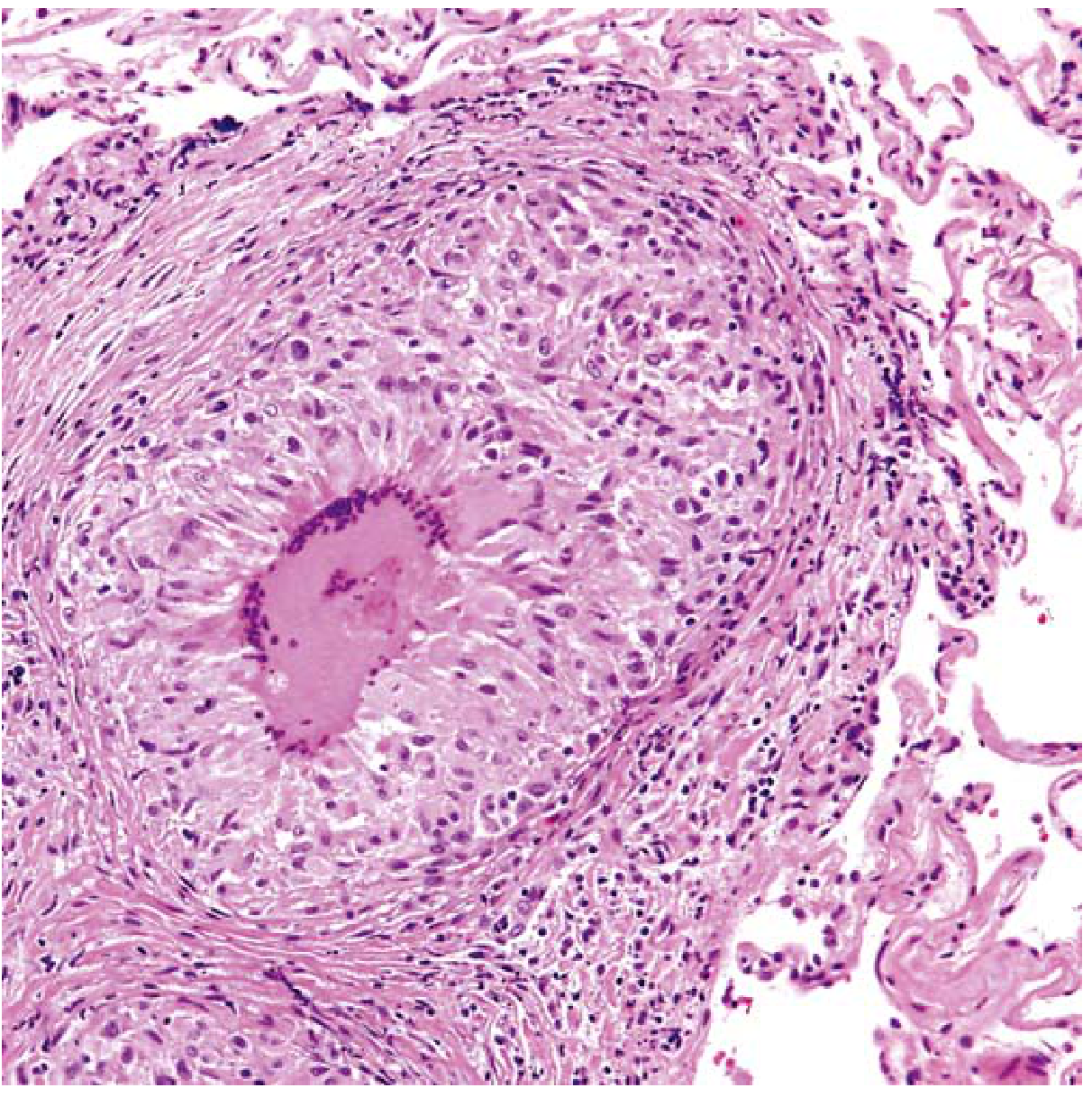
Characteristic noncaseating granuloma with a large central multinucleated giant cell
Structure of granuloma:
- Discrete compact collection of epithelioid macrophages
- Rimmed by an outer zone rich in CD4+ T cells
- Intermixed multinucleate giant cells (from fused macrophages)
- Thin layer of laminated fibroblasts peripherally → over time → hyalinized scar
Special bodies (not required for diagnosis, not specific):
- Schaumann bodies - laminated concretions of calcium and proteins
- Asteroid bodies - stellate inclusions within giant cells
Note: Rarely, foci of central necrosis may appear (nodular form) - but caseation is NOT a feature.
Organ Involvement
Lungs (90%)
- Granulomas in the interstitium (not air spaces)
- "Lymphangitic" distribution - around bronchioles, pulmonary venules, and pleura
- BAL: abundant CD4+ T cells
- 5-15% progress to diffuse interstitial fibrosis → honeycomb lung
Lymph Nodes (75-90%)
- Intrathoracic hilar and paratracheal enlargement
- 1/3 have peripheral lymphadenopathy
- Nodes are painless, firm, rubbery
- Key distinction from TB: "nonmatted" (non-adherent), no necrosis
Skin (~25%)
- Erythema nodosum - hallmark of acute sarcoidosis; bilateral raised, red, tender nodules on anterior legs; it's a panniculitis - classic sarcoid granulomas are actually uncommon in these lesions
- Discrete painless subcutaneous nodules - these DO contain typical noncaseating granulomas
Eyes (20-50%)
- Iritis or iridocyclitis (uveitis) - unilateral or bilateral
- Complications: corneal opacities, glaucoma, vision loss
- Posterior uveal tract: choroiditis, retinitis, optic nerve involvement
- Lacrimal gland involvement → sicca syndrome (dry eyes)
Parotid glands (<10%)
- Painful parotid enlargement, xerostomia (dry mouth)
- Mikulicz syndrome = combined uveoparotid involvement
Spleen
- Granulomas in ~75% microscopically
- Clinical splenomegaly in ~10%
Liver
- Granulomas (usually in portal triads) in ~75%
- Hepatomegaly or abnormal LFTs in ~1/3
Bone Marrow
- Granulomas in up to 40%; rarely causes severe manifestations
Diagnosis
No definitive test exists. Diagnosis requires:
- Clinical + radiologic findings consistent with sarcoidosis
- Exclusion of other disorders (especially TB must be excluded)
- Identification of noncaseating granulomas in involved tissues
Clinical Course & Prognosis
- Many cases: asymptomatic, discovered incidentally on CXR (bilateral hilar adenopathy) or at autopsy
- Course is unpredictable - chronic progressive OR remissions (spontaneous or steroid-induced)
- Prognosis:
- 65-70% recover with minimal/no residual manifestations
- 20% develop permanent lung dysfunction or visual impairment
- 10-15% succumb to progressive pulmonary fibrosis and cor pulmonale
High-Yield Exam Traps
| Trap | Correct Answer |
|---|---|
| Granuloma type in sarcoidosis | Non-caseating (caseation = TB) |
| Low blood CD4+ cells means immunodeficiency? | No - it's just skin test anergy; lung CD4+ cells are HIGH |
| Erythema nodosum granulomas | Classic sarcoidal granulomas are UNCOMMON in EN lesions |
| Sarcoid lymph nodes vs TB nodes | Sarcoid = non-matted, non-necrotic; TB = matted, caseating |
| Schaumann/asteroid bodies - specific to sarcoid? | NO - also seen in other granulomatous diseases |
| Smoking and sarcoidosis | Sarcoidosis is MORE common in nonsmokers |
| After lung transplant | Sarcoidosis recurs in ≥1/3 of patients |
Summary Mnemonic - SARCOID
- S - Schaumann/asteroid bodies (inclusions)
- A - Anergy to PPD/Candida skin tests (blood CD4 low)
- R - Restrictive lung disease (interstitial fibrosis)
- C - CD4+ Th1 cells drive it; Cor pulmonale (end-stage)
- O - Ocular (iritis/iridocyclitis), unknown etiology
- I - IL-2, IFN-γ (Th1 cytokines); Incidence in African Americans
- D - Diagnosis of exclusion; Diffuse hilar adenopathy on CXR
Source: Robbins & Kumar Basic Pathology, pp. 461-463; Robbins, Cotran & Kumar Pathologic Basis of Disease
Everything about thyroid neoplasms
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from both Robbins books. Let me compile the full revision notes.
Thyroid Neoplasms - Complete Robbins Revision Notes
Overview
Thyroid tumors range from benign follicular adenomas to highly aggressive anaplastic carcinomas.
Clinical clues suggesting malignancy in a thyroid nodule:
- Solitary nodule (vs. multiple)
- Age < 30 years or male gender
- History of radiation exposure
- Cold nodule on radionuclide scan (does not take up radioactive iodine)
- Majority of solitary nodules are benign; carcinomas account for < 1% of solitary thyroid nodules
Important: Ultrasound + fine-needle aspiration (FNA) biopsy are essential for preoperative evaluation.
1. Thyroid Adenoma (Follicular Adenoma)
Key Features
- Typically solitary, spherical lesion derived from follicular epithelium
- Most are nonfunctional; small proportion are toxic adenomas (produce thyroid hormone → thyrotoxicosis)
- Follicular adenomas are generally NOT forerunners of carcinoma, though shared genetics (RAS, PTEN) raise the possibility that some follicular carcinomas arise in preexisting adenomas
Genetics
| Adenoma Type | Mutation |
|---|---|
| Toxic adenoma (functional) | Gain-of-function TSHR mutation (most common); less commonly GNAS (Gsα subunit) |
| Nonfunctional adenoma | RAS mutations (<20%), PTEN mutations |
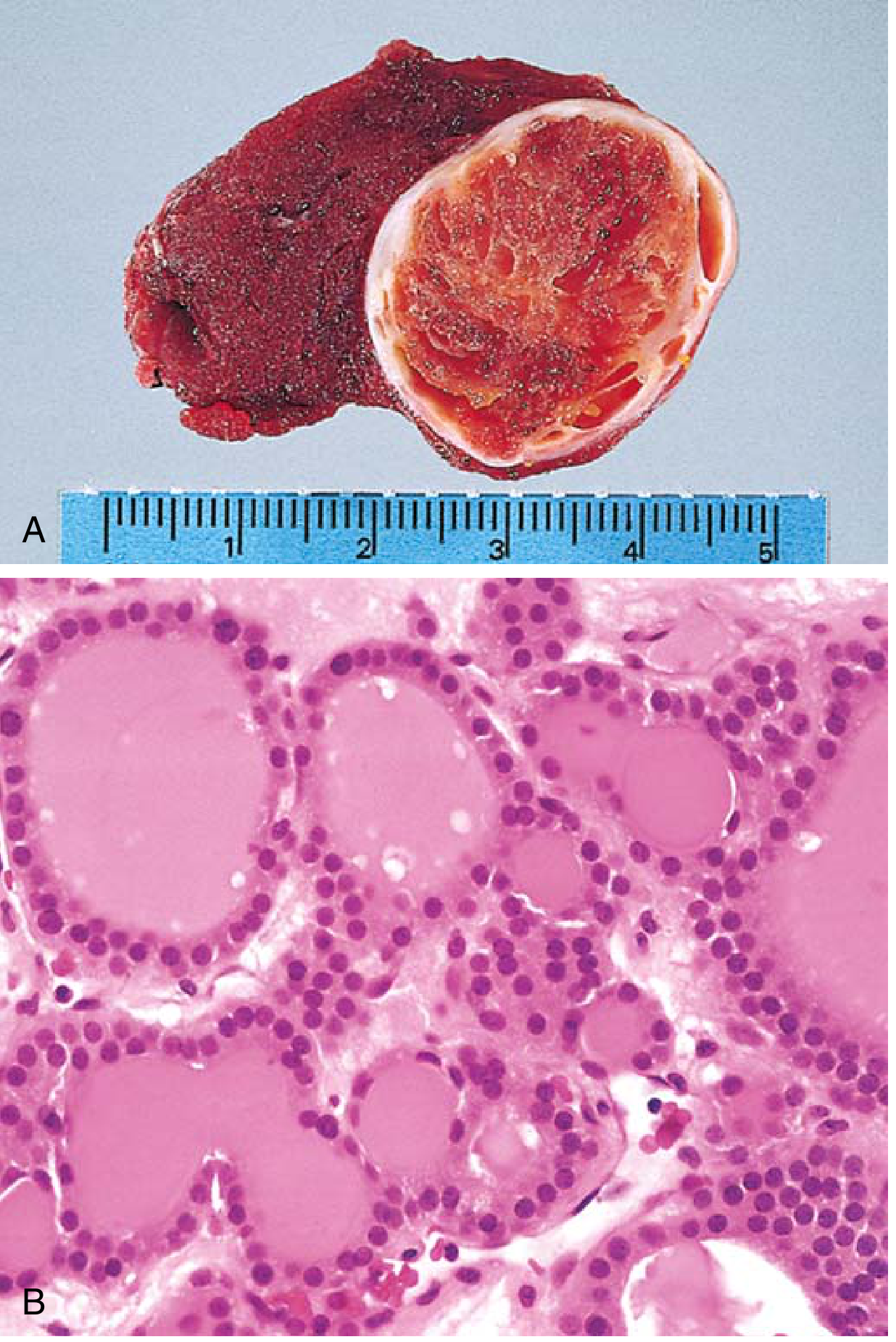
Morphology
- Gross: Solitary, spherical, compresses adjacent thyroid
- Micro: Uniform follicles with colloid; cells uniform in size, shape, nuclear morphology; mitotic figures rare
- Key hallmark: Intact capsule encircling the ENTIRE tumor - this is what distinguishes adenoma from follicular carcinoma
- Occasional oxyphil (Hürthle cell) change - brightly eosinophilic granular cytoplasm
Radionuclide Scan
- Nonfunctional (cold nodule): Takes up less iodine than normal thyroid - up to 10% of cold nodules prove malignant
- Toxic adenoma (hot/warm nodule): Malignancy is uncommon in hot nodules
Prognosis
Excellent - do not recur after surgical removal.
2. Thyroid Carcinomas - Overview
| Type | Frequency | Origin | Key Feature |
|---|---|---|---|
| Papillary thyroid carcinoma (PTC) | ~85% | Follicular epithelium | Orphan Annie nuclei, psammoma bodies |
| Follicular thyroid carcinoma (FTC) | 5-15% | Follicular epithelium | Vascular/capsular invasion (NO lymph spread) |
| Medullary thyroid carcinoma (MTC) | 5% | Parafollicular C cells | Calcitonin, amyloid, RET mutation |
| Anaplastic (undifferentiated) | <5% | Follicular epithelium | Most aggressive, worst prognosis |
3. Papillary Thyroid Carcinoma (PTC)
Epidemiology
- Most common thyroid malignancy (~85% of cases in the US)
- Most often between 25-50 years of age
- Most thyroid carcinomas associated with prior ionizing radiation are papillary
Genetics (HIGH YIELD)
- BRAF V600E mutation - most common; associated with more aggressive behavior
- RET/PTC rearrangements - especially in radiation-induced PTC
- RAS mutations - seen in follicular variant of PTC
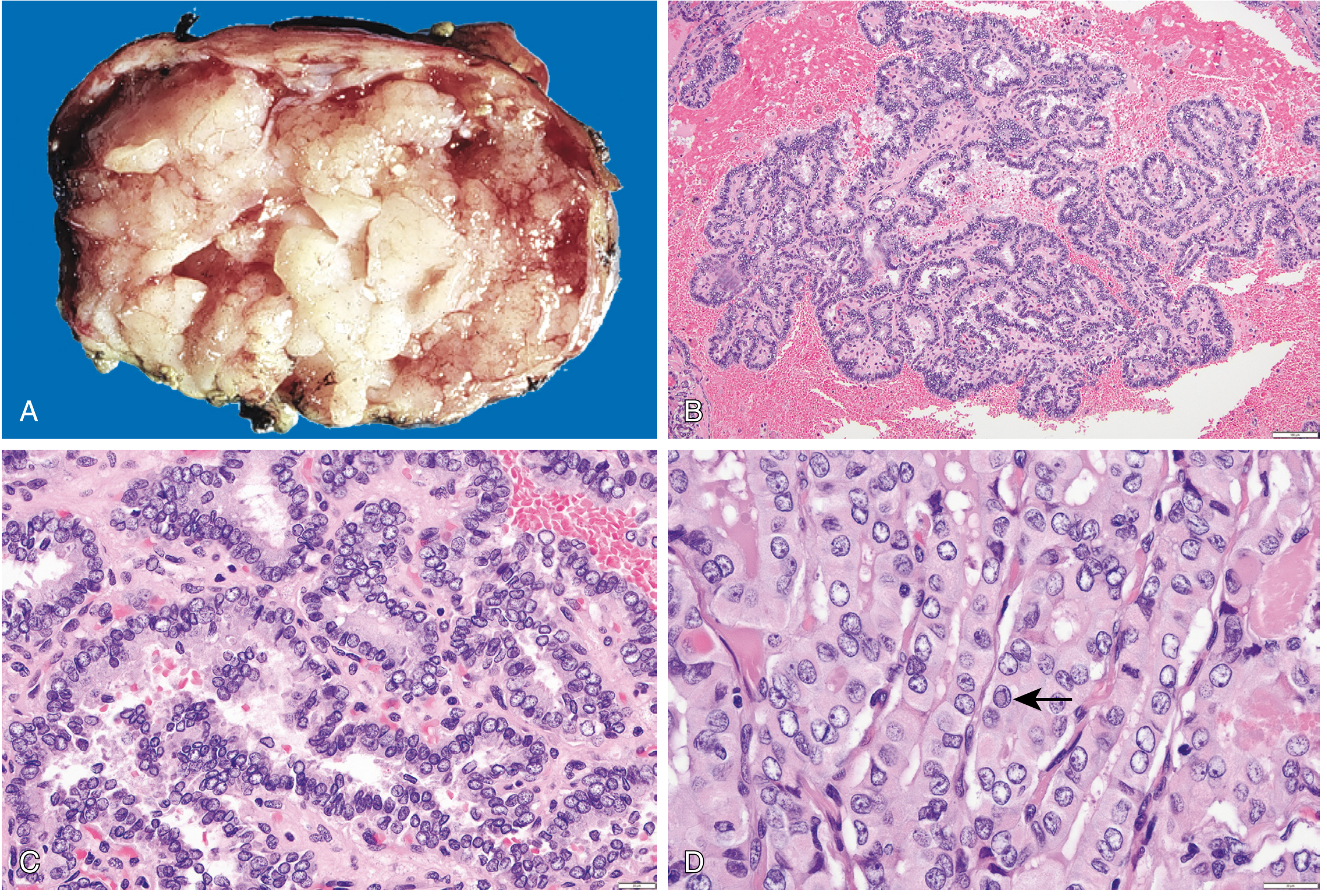
Morphology
Gross:
- May be solitary or multifocal
- Some well-circumscribed, others infiltrate adjacent parenchyma (ill-defined margins)
- May contain fibrosis, calcification; often cystic
Micro (HALLMARKS - HIGH YIELD):
-
Branching papillae with fibrovascular stalk covered by cuboidal epithelial cells (single to multiple layers)
-
Orphan Annie eye nuclei (ground-glass nuclei) - finely dispersed chromatin giving optically clear/empty appearance
- Plus: nuclear membrane irregularities → nuclear grooves (coffee-bean shapes) and pseudoinclusions (cytoplasm invaginating into nucleus)
-
Psammoma bodies - concentrically calcified structures within papillary cores or adjacent stroma
- Almost NEVER found in follicular or medullary carcinomas
- Strong indicator of PTC in FNA material
-
Lymphatic invasion commonly present; blood vessel involvement uncommon (contrast with follicular carcinoma)
-
Cervical lymph node metastases in up to 50% of cases
Clinical Features
- Usually presents as asymptomatic thyroid nodule; first manifestation may be enlarged cervical lymph node
- Nodules move freely with thyroid during swallowing
- Hoarseness, dysphagia, cough, dyspnea = advanced disease
- Cold mass on scintigraphy
- "Hot" nodules = almost never malignant (only do scintigraphy if TSH is low)
Prognosis
- Excellent - 10-year survival > 95%
- 5-20% have local/regional recurrences; 10-15% have distant metastases
- Prognosis worse with: age > 55, extrathyroidal extension, distant metastases
NIFTP (HIGH YIELD - new entity)
Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features (NIFTP)
- Encapsulated follicular variant of PTC with NO invasion
- Reclassified from malignant to a low-risk neoplasm (no longer called carcinoma)
- Distinguished from invasive encapsulated follicular variant of PTC by absence of capsular/vascular invasion
4. Follicular Thyroid Carcinoma (FTC)
Epidemiology
- 5-15% of primary thyroid cancers (US/iodine-sufficient areas)
- In iodine-deficient areas: rises to 25-40% of thyroid cancers
- Presents in older patients than PTC - peak incidence 40-60 years
Genetics
- RAS mutations (most common)
- PAX8-PPARG rearrangement (translocation) - characteristic of FTC
Morphology
Gross:
- Usually solitary, circumscribed or widely infiltrative
- Sharply demarcated lesions can be indistinguishable from follicular adenomas grossly
- Gray to tan to pink; may be translucent (large colloid-filled follicles)
- Degenerative changes: central fibrosis, coarse calcification
Micro (KEY DISTINCTION from adenoma):
- Uniform cells forming small follicles with colloid - resembles normal thyroid
- Nuclei LACK papillary carcinoma features; NO psammoma bodies
- Occasional oncocytic (Hürthle cell) variant - abundant granular eosinophilic cytoplasm
- Adenoma vs. Carcinoma: NO reliable cytologic difference on FNA - requires extensive histologic sampling of tumor capsule to identify:
- Capsular invasion and/or
- Vascular invasion (venous vessels within/just beyond capsule)
Spread Pattern (KEY CONTRAST WITH PTC)
- Hematogenous spread (not lymphatic) → distant metastases
- Lymph node involvement uncommon (opposite of PTC)
- Hematogenous mets most commonly to lung (and bone)
Prognosis
- Worse than PTC
- Minimally invasive FTC (capsular invasion only): excellent prognosis
- Widely invasive FTC: significantly worse
5. Medullary Thyroid Carcinoma (MTC)
Origin
- Arises from parafollicular C cells (NOT follicular epithelium)
- C cells secrete calcitonin
Epidemiology & Association
- 5% of thyroid carcinomas
- Sporadic (70%): usually presents in 5th-6th decade, typically solitary
- Familial (30%): associated with RET proto-oncogene mutations
- MEN-2A (Sipple syndrome): MTC + pheochromocytoma + parathyroid hyperplasia
- MEN-2B: MTC + pheochromocytoma + mucosal neuromas + marfanoid habitus
- Familial MTC (without MEN features)
- Familial cases: often bilateral and multicentric
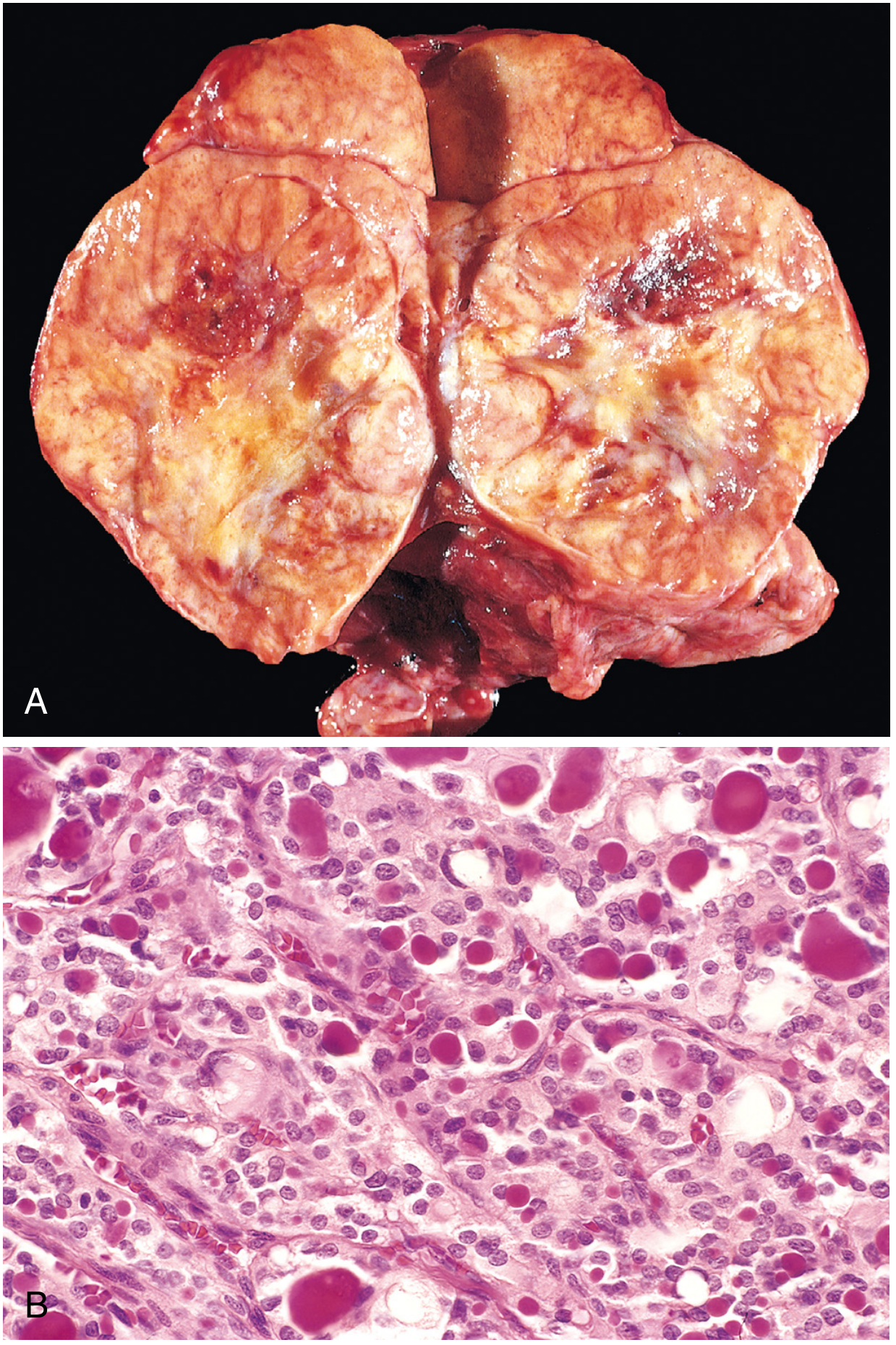
Morphology
- Polygonal to spindle-shaped cells in nests, trabeculae, or follicles
- Amyloid deposits in stroma (derived from calcitonin molecules) - distinctive feature
- C-cell hyperplasia precedes familial MTC (identified in prophylactic thyroidectomies)
- Bilateral/multicentric in familial cases
Clinical Features
- Sporadic: presents as neck mass ± compression effects (dysphagia, hoarseness)
- May secrete other peptide hormones → diarrhea (vasoactive intestinal peptide), flushing (calcitonin, serotonin)
- Screening: serum calcitonin levels or RET mutation testing for family members
- Members of MEN-2 kindreds with RET mutations → prophylactic thyroidectomy offered
Key Markers
- Serum calcitonin (elevated) - diagnostic marker and screening tool
- Amyloid in stroma (calcitonin-derived)
6. Anaplastic (Undifferentiated) Thyroid Carcinoma
Key Features
- Represents <5% of thyroid tumors but is the most aggressive
- Usually occurs in patients >65 years of age
- May arise from dedifferentiation of pre-existing differentiated carcinoma (PTC or FTC) or de novo
- Near-100% mortality; most patients die within 1 year of diagnosis
Genetics
- TP53 mutations (most common) - often with co-existing RAS or BRAF mutations (suggesting progression from differentiated carcinoma)
- TERT promoter mutations
Morphology
- Highly pleomorphic, undifferentiated cells - may be:
- Spindle cells
- Giant cells
- Mixed
- Extensive necrosis and mitotic figures
- Invades adjacent structures extensively
Clinical Features
- Rapidly enlarging, hard, fixed neck mass
- Often presents with airway obstruction, dysphagia, hoarseness at time of diagnosis
- Distant metastases common at presentation
High-Yield Comparison Table
| Feature | Papillary | Follicular | Medullary | Anaplastic |
|---|---|---|---|---|
| Frequency | 85% | 5-15% | 5% | <5% |
| Origin | Follicular cells | Follicular cells | C cells (parafollicular) | Follicular cells |
| Age | 25-50 | 40-60 | Variable | >65 |
| Spread | Lymphatic (LN mets in 50%) | Hematogenous (lung, bone) | Both | Direct invasion |
| Psammoma bodies | YES | No | No | No |
| Orphan Annie nuclei | YES | No | No | No |
| Amyloid stroma | No | No | YES | No |
| Calcitonin marker | No | No | YES | No |
| RET mutation | RET/PTC rearrangement | No | RET point mutation (MEN2) | TP53 |
| BRAF V600E | YES (most common) | No | No | Sometimes |
| RAS | Yes (follicular variant) | YES | No | Sometimes |
| PAX8-PPARG | No | YES | No | No |
| FNA diagnosis | Yes (reliable) | No - can't distinguish from adenoma | Yes | Yes |
| Prognosis | Excellent (>95% 10yr) | Good (minimally invasive) | Intermediate | Dismal (<5% 5yr) |
Nodule Evaluation: Hot vs. Cold (HIGH YIELD)
| Nodule Type | Radioiodine Uptake | Malignancy Risk |
|---|---|---|
| Cold (nonfunctional) | Less than normal thyroid | Up to 10% malignant |
| Warm/Hot (functional) | Equal or greater than normal | Malignancy very rare |
Rule: Always do scintigraphy only if TSH is low (otherwise not clinically indicated).
Key Exam Traps
| Trap | Correct Fact |
|---|---|
| FNA can distinguish follicular adenoma from carcinoma | WRONG - capsular/vascular invasion can only be assessed on surgical histology |
| Psammoma bodies in medullary or follicular carcinoma | Almost NEVER - strongly indicates papillary carcinoma |
| PTC spreads via blood | No - PTC spreads via lymphatics; FTC spreads via blood |
| MTC is derived from follicular cells | No - from C cells (parafollicular) |
| All hot nodules need biopsy | No - hot nodules are almost never malignant |
| Familial MTC = always bilateral | YES - bilateral/multicentric in familial cases |
| Anaplastic carcinoma - any chance of cure | Essentially no - near 100% fatality |
| NIFTP is a carcinoma | No - it was reclassified as a low-risk neoplasm |
Mnemonic: PFMA (types in frequency order)
- Papillary - 85% - Psammoma, Papillae, Paediatric/young adults
- Follicular - 5-15% - Fibrovascular invasion needed, Far (haematogenous) spread
- Medullary - 5% - MEN-2, Marker calcitonin, aMyloid
- Anaplastic - <5% - Awful prognosis, Aged patients, Aggressive
Sources: Robbins & Kumar Basic Pathology, pp. 735-740; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 1005-1012
This is a shared conversation. Sign in to Orris to start your own chat.